Gave the treatment for the PDR resistance
Reading File
Finding Sources
Finding Sources
Searching PubMed
pandrug-resistant treatment options
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information to provide a thorough answer on PDR (Pandrug-Resistant) organism treatment. Let me compile this.
Treatment of Pandrug-Resistant (PDR) Infections
Definition & Context
Pandrug-resistant (PDR) bacteria are organisms resistant to all available antibiotic classes. This sits at the extreme end of the resistance spectrum:
- MDR (Multidrug-Resistant): resistant to ≥3 antibiotic classes
- XDR (Extensively Drug-Resistant): susceptible to only 1-2 classes
- PDR (Pandrug-Resistant): resistant to ALL available antimicrobial agents
Most commonly involved organisms: Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, and other Gram-negative bacilli (GNB).
General Principles
- Source control is mandatory - drain abscesses, debride necrotic tissue, remove infected foreign bodies/catheters. This is often required for cure regardless of antibiotic choice.
- Culture before treating - obtain cultures from the infection site and blood before initiating antibiotics.
- Use combination therapy - with PDR organisms, combining agents (even with limited susceptibility) improves the probability that at least one agent will be active.
- Assess clinical response - in vitro testing may not always detect resistance; clinical monitoring is essential.
- Infection control measures - isolation, dedicated personnel, gowns and gloves to prevent spread (especially for PDR P. aeruginosa and Acinetobacter).
Drug Options for PDR/Near-PDR Gram-Negative Infections
Novel Beta-Lactam/Beta-Lactamase Inhibitor (BL/BLI) Combinations
These are now first-line options for carbapenem-resistant and PDR organisms:
| Agent | Dose | Activity Against |
|---|---|---|
| Ceftazidime-avibactam | 2.5 g IV q8h | ESBL, KPC, OXA-48, CRPA |
| Ceftolozane-tazobactam | 1.5-3 g IV q8h | ESBL, CRPA (not KPC/MBL) |
| Imipenem-cilastatin-relebactam | Standard dosing | ESBL, KPC, CRPA |
| Meropenem-vaborbactam | Standard dosing | ESBL, KPC, CRE |
| Sulbactam-durlobactam | Standard dosing | Acinetobacter baumannii (CRAB) |
Key: Ceftazidime-avibactam is the broadest, covering KPC and OXA-48 carbapenemases, but does NOT cover metallo-beta-lactamases (MBL/NDM).
Siderophore Cephalosporin - The Broadest Option
- Cefiderocol - Active against ESBL, KPC, OXA-48, MBL (NDM/VIM/IMP), CRPA, CRAB, and Stenotrophomonas maltophilia. This is the only agent with activity across ALL carbapenemase types. Use with caution outside UTIs and HABP/VABP due to limited clinical data.
"Last Resort" Agents
When newer agents are unavailable or organisms remain resistant:
| Agent | Dose | Notes |
|---|---|---|
| Colistin (Polymyxin E) | Loading: 5 mg/kg IV, then 2.5 mg × [1.5 × CrCl + 30] IV q12h | High nephrotoxicity risk; inactive vs. Proteae, Serratia |
| Polymyxin B | 2.5-3.0 mg/kg/day IV in 2 divided doses | Similar spectrum to colistin |
| Tigecycline | Standard dosing | Limited tissue penetration; suboptimal in blood/urine |
| Fosfomycin | IV formulation | Used in combination; resistance emerges rapidly with monotherapy |
Nephrotoxicity warning: Treatment with polymyxins, especially combined with other nephrotoxic agents, carries a HIGH risk of renal toxicity - monitor renal function closely.
By Organism
PDR/CRAB (Carbapenem-Resistant Acinetobacter baumannii)
- Preferred: Sulbactam-durlobactam (novel BLI with intrinsic activity against Acinetobacter)
- Alternative: Cefiderocol
- Last resort: Polymyxin B or colistin + carbapenem combination (even when resistant, high-dose carbapenem may provide synergy) ± tigecycline ± fosfomycin
PDR Pseudomonas aeruginosa (CRPA)
- Preferred: Ceftolozane-tazobactam, ceftazidime-avibactam, or imipenem-relebactam
- Alternative: Cefiderocol
- Combination: anti-pseudomonal beta-lactam + aminoglycoside (amikacin preferred) or ciprofloxacin
- Last resort: Colistin/Polymyxin B
PDR CRE (Carbapenem-Resistant Enterobacterales)
- KPC-producing: Ceftazidime-avibactam OR meropenem-vaborbactam OR imipenem-relebactam
- MBL-producing (NDM, VIM, IMP): Ceftazidime-avibactam + aztreonam, OR cefiderocol
- OXA-48: Ceftazidime-avibactam OR cefiderocol
PDR Stenotrophomonas maltophilia
- First-line: Cefiderocol
- Alternative: TMP-SMX (if susceptible), minocycline
Site-Specific Treatment
- Pneumonia (HABP/VABP): BL/BLI combination as the beta-lactam backbone + consider aminoglycoside or fluoroquinolone if resistant risk factors. Add vancomycin or linezolid if MRSA risk.
- Bacteremia: Treat aggressively with IV combination therapy; source control paramount.
- Intra-abdominal infection: BL/BLI (e.g., ceftazidime-avibactam or ceftolozane-tazobactam) + metronidazole for anaerobic coverage; 7-10 days duration.
- UTI: Ceftazidime-avibactam, meropenem-vaborbactam, or cefiderocol (most clinical data exist here).
- Osteomyelitis: Extended 6-week course; surgical drainage if neurological compromise, instability, or treatment failure.
Emerging/Investigational Strategies
Recent reviews highlight additional options being explored for PDR organisms (nanotechnology approaches and phage therapy):
- Bacteriophage therapy - lytic phages targeting specific resistant strains; used compassionately in some PDR cases
- Nanoparticle-based antibiotics - still investigational
- Antibiotic recycling - fosfomycin and rifampin as adjuncts in combination regimens
Key Takeaways
- PDR infections leave few or no ideal options - combination therapy is the rule.
- Cefiderocol is the broadest single agent covering all carbapenemase types.
- Ceftazidime-avibactam is preferred for KPC/OXA-48-producing CRE.
- Colistin/Polymyxin B remain last-resort salvage agents but carry significant nephrotoxicity.
- Antimicrobial stewardship and infection control are the best tools to prevent PDR emergence and spread.
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Treatment of GNB Infections, p. 1326
- The Washington Manual of Medical Therapeutics, Activity of Novel Gram-Negative Antibiotics vs. Resistant Organisms
- Goldman-Cecil Medicine, P. aeruginosa chapter - Infection Control
- Harrison's (Fishman's Pulmonary), HAP/VAP Empirical Antibiotic Treatment Table
Pneumocystis infectione
Reading File
Finding Sources
Searching PubMed
Pneumocystis jirovecii pneumonia treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have thorough information. Let me compile the comprehensive answer.
Pneumocystis jirovecii Infection (PCP)
Overview
Pneumocystis jirovecii (formerly P. carinii) is an obligate ascomycetous, extracellular yeast-like fungus that is tropic to mammalian lung tissue. It causes Pneumocystis pneumonia (PCP) - an opportunistic infection almost exclusively in immunocompromised hosts. A critical feature: it lacks ergosterol in its cell membrane (uses cholesterol instead), making it intrinsically resistant to azoles and amphotericin B.
Epidemiology & Risk Factors
In HIV/AIDS:
- Still the most common AIDS-defining opportunistic infection in the US
- ~95% of adult cases occur when CD4+ count < 200 cells/μL (or CD4% < 14%)
- Other risk factors: prior PCP, oropharyngeal candidiasis, HIV RNA detectable despite ART
Non-HIV immunocompromised (now 60-70% of new cases in developed world):
- Prolonged high-dose corticosteroids
- Chemotherapy recipients
- Solid organ transplant (especially renal transplant)
- Hematopoietic stem cell transplant (HSCT)
- Autoimmune diseases on immunosuppressants
- Hematologic malignancies
Transmission: Person-to-person via aerosolized droplets; likely also reactivation of latent infection. Serologic studies show 85-100% of the US population has anti-Pneumocystis antibodies by age 3.
Clinical Presentation
| Feature | HIV-Positive | HIV-Negative |
|---|---|---|
| Onset | Subacute (weeks) | More acute (days) |
| CD4 threshold | <200 cells/μL | Variable |
| Organism burden | High | Low |
| Classic triad | Fever + dry cough + progressive dyspnea | Same, but faster decline |
| LDH | Elevated (non-specific but supportive) | Elevated |
| SpO2 | Often desaturates on exertion | Often desaturates on exertion |
Diagnosis
Imaging
- Chest X-ray: Bilateral, symmetric, perihilar interstitial infiltrates progressing to diffuse alveolar pattern (classic "ground-glass" appearance)
- HRCT chest: Ground-glass opacities - more sensitive when CXR is normal (present in 0-39% of PCP cases!)
- Nodules with/without cavitation, miliary pattern occasionally seen
- Adenopathy and pleural effusions are rare - suggest alternative diagnosis
Lab Markers (Supportive, Not Diagnostic)
- LDH: Elevated - non-specific but useful; very high LDH suggests more severe disease
- 1,3-β-D-glucan: Sensitive peripheral marker - elevated in PCP; helps distinguish infection from colonization when PCR is positive
Microbiologic Diagnosis (Required for Definitive Dx)
P. jirovecii cannot be cultured - diagnosis depends on organism visualization or molecular detection:
| Method | Specimen | Sensitivity | Notes |
|---|---|---|---|
| Methenamine silver (GMS) stain | BAL | 63-100% (HIV+), 46-100% (HIV-) | Cyst walls |
| Giemsa / Diff-Quik | BAL | Variable | Stains both cysts AND trophozoites |
| Immunofluorescence (IFA) | BAL | 71-100% | Higher specificity than PCR |
| PCR | BAL, induced sputum, oral wash | 91-100% (highly sensitive) | May be positive in colonization |
| Induced sputum | Non-invasive | Less than BAL | First step; if negative, proceed to bronchoscopy |
| Oral wash PCR | Very non-invasive | 54-100% | Useful initial test (HIV+) |
Gold standard: BAL + immunofluorescence or PCR. In HIV-negative patients, BAL silver stain alone has only 46% sensitivity - always add PCR/IFA.
Treatment
FIRST-LINE: Trimethoprim-Sulfamethoxazole (TMP-SMX)
Drug of choice for mild, moderate, AND severe PCP.
| Parameter | Details |
|---|---|
| Dose | TMP: 15-20 mg/kg/day (range); SMX: 75-100 mg/kg/day |
| Divided doses | Every 6-8 hours (3-4 times daily) |
| Route | IV preferred for moderate-severe; switch to PO after clinical improvement |
| Duration | 21 days (HIV+); at least 14-21 days (HIV-) |
Common adverse effects (especially in HIV+, often week 2):
- Rash (can treat through mild rash by reducing dose by half or desensitizing)
- Fever, nausea, vomiting
- Elevated aminotransferases
- Hyperkalemia
- Bone marrow suppression (anemia, neutropenia)
- Rare: Stevens-Johnson syndrome, toxic epidermal necrolysis, septic shock-like syndrome
Note: Patients who develop PCP despite TMP-SMX prophylaxis can usually still be treated with TMP-SMX.
ALTERNATIVE REGIMENS (for TMP-SMX allergy/intolerance)
| Agent(s) | Dose | Severity | Key Side Effects |
|---|---|---|---|
| Pentamidine IV | 4 mg/kg/day IV (max 300 mg/day) | Severe | Nephrotoxicity, hypotension, electrolyte abnormalities, life-threatening cardiac arrhythmias |
| Clindamycin + Primaquine | Clindamycin 450-600 mg PO q6-8h OR 900 mg IV q8h; Primaquine 15-30 mg oral base/day | Mild-Moderate-Severe | Methemoglobinemia, diarrhea; check G6PD before primaquine |
| Dapsone + TMP | Dapsone 100 mg/day PO + TMP 5 mg/kg/day | Mild-Moderate | Methemoglobinemia, G6PD hemolysis; may be tolerated in sulfa allergy |
| Atovaquone suspension | 750 mg PO BID (with fatty food) | Mild-Moderate | Variable absorption (take with fatty food), rash, GI intolerance |
Severity guide - Mild: PaO2 >70 mmHg or A-a gradient <35; Moderate: PaO2 50-70 mmHg; Severe: PaO2 <70 mmHg or A-a gradient >35.
ADJUNCTIVE CORTICOSTEROIDS (Critical for Severe Disease)
Corticosteroids improve survival in HIV+ patients with hypoxia (PaO2 < 70 mmHg on room air, or A-a gradient > 35).
| Drug | Dose | Schedule |
|---|---|---|
| Prednisone | 40 mg PO twice daily | Days 1-5 |
| 40 mg PO once daily | Days 6-10 | |
| 20 mg PO once daily | Days 11-21 | |
| IV methylprednisolone | 75% of prednisone dose | If unable to take PO |
Adjunctive steroids also possibly helpful in HIV-negative patients with severe PCP, though evidence is less robust.
IRIS (Immune Reconstitution Inflammatory Syndrome)
- HIV+ patients starting both PCP treatment and ART simultaneously may develop a paradoxical worsening (fever, worsening infiltrates) - rarely respiratory failure
- IRIS is a diagnosis of exclusion; rarely requires stopping ART
Mechanical Ventilation (Severe/ICU)
- Acute respiratory failure from PCP carries ~30-50% mortality even with mechanical ventilation
- Use lung-protective ventilation strategies (same as ARDS)
- ART may be beneficial even in ICU setting
Prophylaxis
Primary Prophylaxis (Prevention before first episode)
Indications:
- HIV+ adults/adolescents with CD4 < 200 cells/μL or CD4% < 14%
- Non-HIV: prolonged immunosuppression (solid organ transplant, HSCT, long-term steroids, etc.)
Prophylaxis Regimens
| Agent | Dose | Notes |
|---|---|---|
| TMP-SMX (1st line) | 1 DS tablet daily OR 1 SS tablet daily OR 1 DS tablet 3x/week | Also protects against Toxoplasma |
| Dapsone | 100 mg/day PO | Check G6PD first |
| Dapsone + Pyrimethamine + Leucovorin | Dapsone 50 mg/day + Pyrimethamine 50 mg/week + Leucovorin 25 mg/week | For TMP-SMX intolerant; better Toxoplasma coverage |
| Atovaquone suspension | 1500 mg/day PO with food | Well tolerated |
| Aerosolized pentamidine | 300 mg monthly by nebulizer | Increased breakthrough risk at CD4 <100 cells/μL |
Stopping Prophylaxis (HIV+)
- May discontinue primary prophylaxis when CD4 rises > 200 cells/μL for at least 3 months on ART
- Consider stopping at CD4 100-200 cells/μL if HIV RNA undetectable for 3-6 months
Secondary Prophylaxis (after first episode)
- Same agents as primary
- Discontinue when CD4 > 200 cells/μL for ≥3 months on ART
- Caution with aerosolized pentamidine for secondary prophylaxis (higher breakthrough risk)
Recent Evidence Update (2024-2025)
A 2025 network meta-analysis (Hatzl et al., PMID 39732393) comparing treatment regimens for PCP in HIV+ patients confirmed TMP-SMX remains superior. A 2024 systematic review (Prosty et al., PMID 38583518) on prophylaxis confirmed TMP-SMX as the most effective prophylactic agent. A 2024 meta-analysis (Brown et al., PMID 38860786) validated PCR on respiratory specimens as highly sensitive for PCP diagnosis in immunocompromised patients.
Sources: Fishman's Pulmonary Diseases and Disorders, Ch. 134; Murray & Nadel's Textbook of Respiratory Medicine, Ch. 123; Goldman-Cecil Medicine, Pneumocystis chapter; Katzung's Basic & Clinical Pharmacology, 16th ed.
How does G6PD deficiency affect PCP treatment choices?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have all the detail needed. Here is the full answer.
G6PD Deficiency and PCP Treatment
The Core Mechanism
Glucose-6-phosphate dehydrogenase (G6PD) is the rate-limiting enzyme of the pentose phosphate pathway. Its main role in red blood cells is generating NADPH, which in turn keeps glutathione in its reduced (active) form. Reduced glutathione is the RBC's primary defense against oxidative stress.
When G6PD is deficient:
- NADPH production fails under oxidant challenge
- Glutathione is depleted
- Oxidative damage goes unchecked
- Hemoglobin is oxidized to methemoglobin and forms Heinz bodies
- RBCs are destroyed (hemolytic anemia)
Several PCP treatment and prophylaxis drugs are potent oxidants and directly trigger this cascade in G6PD-deficient patients.
Drugs Affected by G6PD Status
1. Dapsone - AVOID / Use with Extreme Caution
Dapsone is used in two PCP contexts:
- Treatment: Dapsone 100 mg/day + TMP (alternative to TMP-SMX)
- Prophylaxis: Dapsone alone, or dapsone + pyrimethamine + leucovorin
Why it's dangerous in G6PD deficiency:
Dapsone is metabolized by N-hydroxylation to dapsone hydroxylamine, a potent oxidant. Within RBCs, this metabolite:
- Generates reactive oxygen species (ROS)
- Oxidizes oxyhemoglobin → methemoglobin
- Creates Heinz bodies (denatured hemoglobin visible on peripheral smear)
- Labels RBCs for splenic destruction → hemolytic anemia
These effects are dose-dependent and affect all patients to some degree, but are dramatically amplified in G6PD-deficient individuals. A drop of 1-2 g/dL hemoglobin is anticipated even in normal patients; in G6PD deficiency this can become severe or life-threatening.
Mandatory pre-screening rule: G6PD deficiency must be ruled out BEFORE starting dapsone. This is listed as a required pre-therapy laboratory test alongside CBC and reticulocyte count.
2. Primaquine - AVOID
Primaquine is used in the combination:
- Treatment: Clindamycin + primaquine (oral base 15-30 mg/day)
Primaquine is one of the classic triggers of G6PD-related hemolysis - this was first recognized when ~10% of African American males given primaquine as an antimalarial during the Korean War developed acute hemolytic anemia. It exerts the same oxidant mechanism as dapsone.
Rule: Screen for G6PD deficiency before prescribing primaquine. If G6PD deficient, this regimen is contraindicated.
Note: The treatment table in Fishman's Pulmonary explicitly flags both dapsone+TMP and clindamycin+primaquine with "Methemoglobinemia, G6PD" as the key consideration.
Treatment Decision Framework by G6PD Status
| PCP Severity | Normal G6PD | G6PD Deficient |
|---|---|---|
| All severities (1st line) | TMP-SMX | TMP-SMX (safe - no change) |
| Mild-Moderate (alt) | Dapsone + TMP | AVOID dapsone |
| Mild-Moderate (alt) | Clindamycin + Primaquine | AVOID primaquine |
| Mild-Moderate (alt) | Atovaquone 750 mg PO BID | Safe - preferred alternative |
| Severe (alt) | IV Pentamidine | IV Pentamidine (safe - no G6PD concern) |
| Severe (alt) | Clindamycin + Primaquine | AVOID primaquine |
Key practical point:
- TMP-SMX remains the drug of choice regardless of G6PD status - it does not carry oxidant risk to RBCs
- In a G6PD-deficient patient intolerant of TMP-SMX with mild-moderate PCP: atovaquone is the go-to alternative
- In a G6PD-deficient patient with severe PCP who cannot tolerate TMP-SMX: IV pentamidine is the preferred salvage (but carries its own toxicities - nephrotoxicity, arrhythmias, hypotension)
Prophylaxis in G6PD Deficiency
The same logic applies to prophylaxis choices:
| Prophylaxis Regimen | G6PD Concern |
|---|---|
| TMP-SMX (1st line) | No - safe |
| Dapsone alone | Yes - screen first; avoid if deficient |
| Dapsone + Pyrimethamine + Leucovorin | Yes - avoid if G6PD deficient |
| Atovaquone suspension | No - safe, good alternative |
| Aerosolized pentamidine | No - safe (systemic absorption minimal) |
For a G6PD-deficient patient who cannot tolerate TMP-SMX for prophylaxis, atovaquone suspension (1500 mg/day with food) or aerosolized pentamidine (300 mg monthly) are the preferred alternatives.
Monitoring if Dapsone is Unavoidable
If no alternatives exist and dapsone must be used (despite G6PD concern), mandatory monitoring includes:
Before starting: G6PD level, CBC with differential, reticulocyte count, LFTs, renal function
During therapy:
- CBC + reticulocytes: weekly for month 1, then twice monthly for months 2-3
- A hemoglobin drop of 1-2 g/dL is anticipated and tolerable; more than that warrants dose reduction or drug switch
- Monitor reticulocyte count to gauge compensatory erythropoiesis
- If reticulocyte count is markedly elevated, the bone marrow is at maximum compensation - further dose increases are not safe
- Methemoglobin levels: only check if patient is symptomatic (dyspnea, cyanosis)
- Patients should carry a medication card alerting emergency providers to the hemolytic/methemoglobin-generating potential of the drug
Timing caveat: G6PD assay should be obtained when the patient is well, not immediately after a hemolytic episode - newly released reticulocytes have higher G6PD activity, which can give a falsely normal result right after hemolysis.
Sources: Fishman's Pulmonary Diseases and Disorders, Treatment Table 134-2; Fitzpatrick's Dermatology 5e, Dapsone - Hemolysis and Methemoglobinemia section, Initiating and Monitoring Dapsone Therapy; The Washington Manual of Medical Therapeutics, G6PD Deficiency Treatment; Frameworks for Internal Medicine, Hemolytic Anemia
Treatment for thyroid strom
Finding Sources
Searching PubMed
thyroid storm treatment management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I have all the information needed for a complete, well-structured answer.
Treatment of Thyroid Storm (Thyrotoxic Crisis)
Overview
Thyroid storm is a life-threatening emergency - untreated mortality approaches 100%; with prompt treatment, mortality is still 10-30%. It represents severe thyrotoxicosis with multiorgan dysfunction. Death results from arrhythmias, congestive heart failure, respiratory failure, DIC, or hypoxic brain injury.
Clinical diagnosis - do NOT wait for lab confirmation. The Burch-Wartofsky score (1993) helps stratify likelihood:
| System | Features Scored |
|---|---|
| Fever | 99°F (+5) → ≥104°F (+30) |
| Tachycardia | 90-109 bpm (+5) → ≥140 bpm (+25) |
| CNS | Agitation (+10) → Coma (+30) |
| GI/hepatic | Diarrhea/nausea (+10) → Jaundice (+20) |
| Heart failure | Pedal edema (+5) → Pulmonary edema (+25) |
| Precipitant | Present (+10) |
Score ≥45: thyroid storm; 25-44: impending storm; <25: unlikely storm
Treatment - The "5-Step" Framework
The order of drug administration is critical. Iodine given before thionamides can paradoxically worsen thyroid storm by providing substrate for hormone synthesis.
Correct Sequence:
Step 1: Beta-blocker → Step 2: Thionamide (PTU/MMI) → wait 1 hour → Step 3: Iodine → Step 4: Corticosteroid → Step 5: Treat precipitant
STEP 1 - Block Peripheral Adrenergic Effects (Give FIRST)
Goal: Control tachycardia, tremor, hyperpyrexia, agitation; propranolol also blocks T4→T3 conversion
| Drug | Dose | Notes |
|---|---|---|
| Propranolol (preferred) | 60-80 mg PO q4h OR 0.5-1 mg IV slow test dose, then 1-2 mg IV q15 min to effect; then 1-2 mg IV q3h | Non-selective; also blocks T4→T3 conversion; onset ~1h PO |
| Metoprolol | 25-50 mg PO q6h | β1-selective; use in mild asthma/COPD |
| Esmolol | 50-100 μg/kg/min infusion | Short-acting; preferred if concerns about beta-blockade (asthma, pulmonary edema) |
| Reserpine (if BB contraindicated) | 2.5-5 mg IM q4h | Monitor for hypotension |
Caution: Atrial fibrillation is often refractory to rate control until antithyroid therapy is started. In patients with heart failure, use diuretics + ACE inhibitors alongside.
STEP 2 - Inhibit Thyroid Hormone Synthesis (Give BEFORE Iodine)
Goal: Block iodine organification and thyroglobulin synthesis
| Drug | Dose | Preferred In |
|---|---|---|
| PTU (Propylthiouracil) - preferred | 500-1000 mg loading dose, then 250 mg PO/NG q4h | First-trimester pregnancy; also blocks T4→T3 conversion |
| Methimazole | 60-80 mg/day in divided doses | Second/third trimester pregnancy; longer duration of action |
Route: PO or nasogastric tube preferred; rectal enema (pharmacy-prepared) is an alternative for unconscious/intubated patients - same dose for all routes.
Why PTU over methimazole in storm? PTU has the dual action of blocking synthesis AND inhibiting peripheral T4→T3 conversion via type 1 deiodinase (Dio1). Methimazole has longer duration but lacks this T4→T3 blocking effect. PTU is generally preferred in acute thyroid storm for this reason.
Methimazole is available IV outside the US, but not recommended by current American Thyroid Association guidelines.
STEP 3 - Block Thyroid Hormone Release (Give ≥1 HOUR After Thionamide)
Goal: Rapidly block release of stored thyroid hormone (Wolff-Chaikoff effect)
| Drug | Dose | Notes |
|---|---|---|
| SSKI (Saturated Solution KI) | 1-2 drops PO/PR three times daily | 50 mg iodide/drop |
| Lugol's solution | 5-7 drops PO/PR three times daily | 8 mg iodide/drop |
| Sodium iodide | IV - per endocrinology dosing | If oral/NG route not available |
| Lithium carbonate (if iodine-allergic) | 300 mg PO/NG four times daily | Also drug of choice for iodine-induced storm (amiodarone, contrast) |
Critical rule: Iodine given BEFORE thionamides can precipitate or worsen thyroid storm by flooding the gland with substrate for synthesis. Always wait at least 1 hour after the thionamide dose.
STEP 4 - Inhibit T4→T3 Conversion + Treat Relative Adrenal Insufficiency
Goal: Corticosteroids block peripheral conversion of T4 to active T3, and address the increased cortisol demand in critically ill patients
| Drug | Dose |
|---|---|
| Hydrocortisone (preferred) | 300 mg IV loading dose, then 100 mg IV three times daily |
| Dexamethasone | 2-4 mg IV four times daily |
When corticosteroids are combined with PTU and iodide, T3 levels can normalize within 48 hours.
STEP 5 - Identify and Treat the Precipitating Event
Common precipitants to investigate and treat:
| Category | Examples |
|---|---|
| Systemic | Infection (most common), trauma, surgery |
| Cardiovascular | MI, pulmonary embolism, stroke |
| Endocrine | DKA, hyperosmolar coma |
| Drug/hormone | Radioactive iodine therapy, amiodarone, contrast, thyroid hormone ingestion, thionamide withdrawal |
| Obstetric | Labor, eclampsia, hyperemesis gravidarum |
Empirical antibiotics if infection is suspected as precipitant. Up to 25% of cases have no identifiable precipitant.
SUPPORTIVE MEASURES (Simultaneous with Above)
| Goal | Intervention |
|---|---|
| Hyperthermia | Cooling blanket, fans, ice packs, ice lavage; Acetaminophen |
| Avoid aspirin | Aspirin displaces T4/T3 from protein binding → raises free hormone levels |
| Fluid resuscitation | D5/0.9% NS - replaces insensible + GI losses, replenishes depleted glycogen |
| Agitation/seizures | Lorazepam or diazepam (also reduce central sympathetic outflow) |
| Electrolytes | Replace guided by labs |
ADJUNCT / REFRACTORY THERAPIES
| Therapy | Use | Mechanism |
|---|---|---|
| Cholestyramine | Severe/refractory storm | Anion exchange resin - blocks enterohepatic recirculation of thyroid hormone |
| Plasmapheresis | Life-threatening, pre-surgical preparation, refractory cases | Physically removes circulating thyroid hormone |
| ECMO | Cardiovascular collapse, rapid deterioration | Hemodynamic support |
Radioactive iodine and surgery are contraindicated during active thyroid storm - they can precipitate further crisis. Only considered after sustained euthyroid state is established.
SPECIAL SITUATIONS
Pregnancy:
- PTU preferred in first trimester (methimazole is teratogenic in T1 - aplasia cutis risk)
- Methimazole preferred in second and third trimesters (PTU carries hepatotoxicity risk)
- Beta-blockers: use cautiously; propranolol acceptable short-term; esmolol can cause fetal bradycardia
- Avoid radioactive iodine (absolute contraindication)
Amiodarone-induced thyroid storm:
- Type 1 (excess iodine stimulation): Stop amiodarone + thionamide therapy
- Type 2 (destructive thyroiditis): Corticosteroids; amiodarone cessation case-by-case
- Lithium preferred over iodine (iodine-induced storm)
Drugs to AVOID in Thyroid Storm
| Drug | Reason to Avoid |
|---|---|
| Aspirin | Displaces T3/T4 from protein binding → raises free hormone |
| Amiodarone | Contains iodine → can worsen hyperthyroidism |
| Iodinated contrast | Same as amiodarone |
| Pseudoephedrine, albuterol, ketamine | Increase sympathetic tone → worsen adrenergic effects |
Sources: Rosen's Emergency Medicine, Thyroid Storm Management Box 117.3; Cummings Otolaryngology, Thyroid Storm; Goodman & Gilman's Pharmacological Basis of Therapeutics; Tintinalli's Emergency Medicine
What is thyroid strom
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have comprehensive content. Here is the full answer.
Thyroid Storm (Thyrotoxic Crisis)
Definition
Thyroid storm is a rare, life-threatening form of severe thyrotoxicosis characterized by multiorgan dysfunction. It represents the most extreme end of the hyperthyroidism spectrum - not simply "more hyperthyroidism," but a qualitative shift to a systemic crisis with dramatically higher mortality.
- Untreated mortality: approaches 100%
- With prompt treatment: mortality still 10-30% (up to 50% in cardiovascular presentations)
- Death occurs from arrhythmias, congestive heart failure, respiratory failure, DIC, hypoxic brain injury, or sepsis
Pathophysiology
The mechanism for the shift from uncomplicated hyperthyroidism to thyroid storm is not fully understood, but involves:
- Adrenergic hyperactivity - either from increased release of thyroid hormones or increased receptor sensitivity to catecholamines
- Higher levels of free thyroid hormones - circulating T4 and T3 (bound to protein) are freed by precipitating factors; free fraction rises disproportionately
- Excess T3 effect at the cellular level - T4 is converted to active T3, which enters cell nuclei, binds thyroid hormone-responsive elements, and drives hypermetabolism in every tissue
- Precipitant-mediated amplification - stress, infection, trauma, or surgery frees hormones from binding sites and increases receptor sensitivity, multiplying the effect
Key: The total thyroid hormone level in storm may not be higher than in uncomplicated hyperthyroidism - it is the free fraction and tissue sensitivity that distinguish the two states.
Precipitating Factors
Thyroid storm almost always occurs in a patient with pre-existing but often unrecognized or undertreated hyperthyroidism who then faces an acute physiologic stressor:
| Category | Examples |
|---|---|
| Systemic insult | Infection (most common), trauma, surgery |
| Cardiovascular | Myocardial infarction, pulmonary embolism, stroke |
| Endocrine | Diabetic ketoacidosis, hyperosmolar coma |
| Obstetric | Labor and delivery, eclampsia, hyperemesis gravidarum, preeclampsia |
| Drug/hormone-related | Radioactive iodine therapy, iodine administration (contrast, amiodarone), thyroid hormone ingestion, withdrawal of antithyroid medication, thyroid gland palpation |
| Unknown | Up to 25% of cases have no identifiable precipitant |
Clinical Features
Thyroid storm is a clinical diagnosis - do NOT wait for lab confirmation before treating.
The four main organ systems affected:
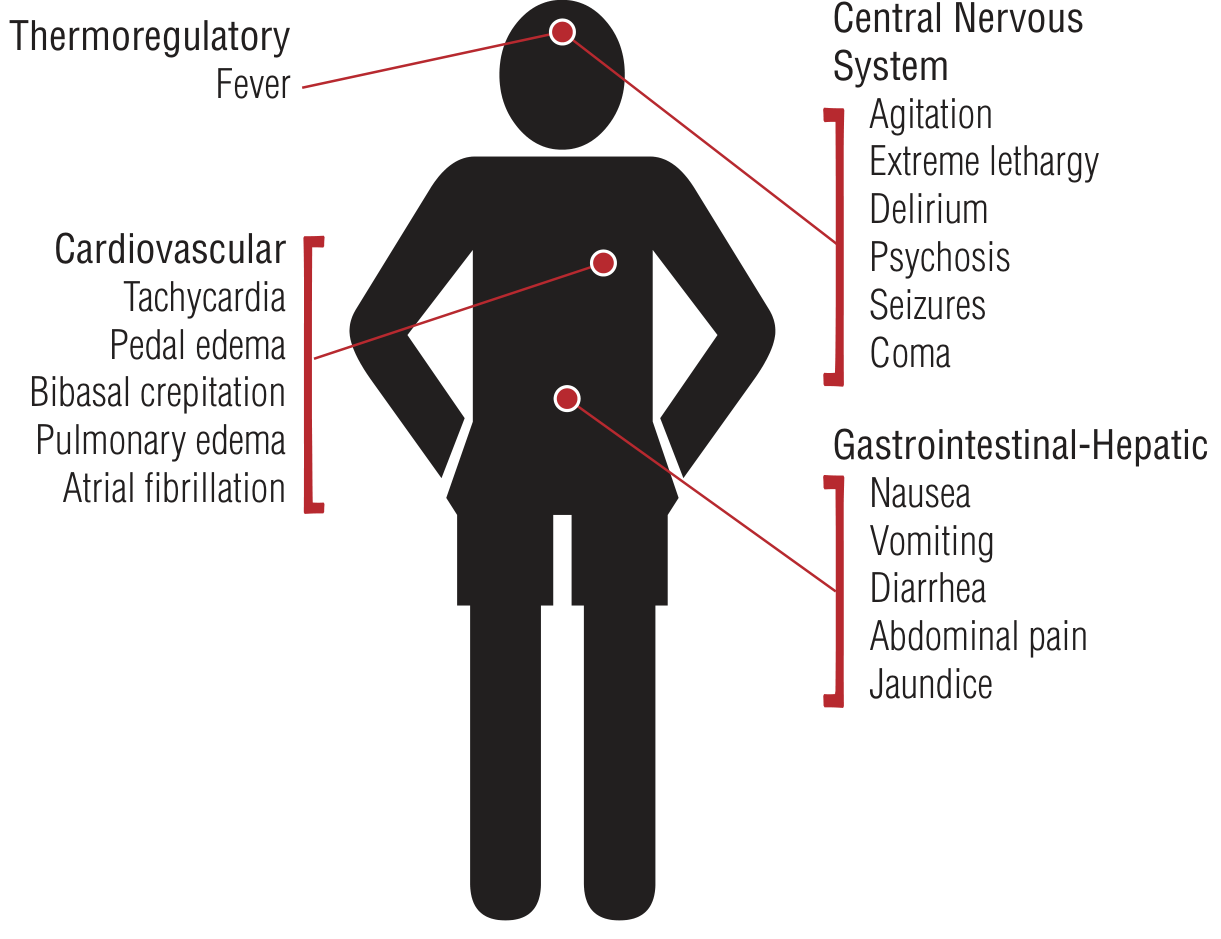
1. Thermoregulatory
- Marked fever: 104°-106°F (40°-41°C) - often the first sign of impending crisis in a known hyperthyroid patient
- Profuse sweating
2. Cardiovascular
- Extreme tachycardia - characteristically out of proportion to the degree of fever
- Atrial fibrillation in 10-35% of cases
- Widened pulse pressure (high cardiac output + reduced peripheral vascular resistance)
- Elevated systolic BP (due to direct inotropic/chronotropic effects of T3 on the heart)
- Congestive heart failure, pulmonary edema, bibasal crepitations, pedal edema
- Hypotension and cardiovascular collapse in severe cases
- Takotsubo (stress) cardiomyopathy can occur as a manifestation
3. Central Nervous System
- Agitation, anxiety, irritability (early)
- Delirium, acute psychosis
- Tremor, weakness
- Seizures
- Coma (late/terminal)
4. Gastrointestinal-Hepatic
- Nausea, vomiting, diarrhea
- Abdominal pain
- Jaundice (hepatic failure with cholestatic jaundice - less common but poor prognostic sign)
Plus the background signs of hyperthyroidism:
- Goiter, exophthalmos/ophthalmopathy (if Graves' disease)
- Lid lag, stare
- Tremor, hyperreflexia
- Warm, moist skin
Diagnosis
Clinical Diagnosis Tool: Burch-Wartofsky Point Scale (BWPS)
Used to distinguish thyrotoxicosis from impending/frank thyroid storm:
| Parameter | Range | Points |
|---|---|---|
| Fever (°F) | 99-99.9 | 5 |
| 100-100.9 | 10 | |
| 101-101.9 | 15 | |
| 102-102.9 | 20 | |
| 103-103.9 | 25 | |
| ≥104 | 30 | |
| Tachycardia (bpm) | 90-109 | 5 |
| 110-119 | 10 | |
| 120-129 | 15 | |
| 130-139 | 20 | |
| ≥140 | 25 | |
| CNS effects | Mild agitation | 10 |
| Delirium/psychosis/extreme lethargy | 20 | |
| Seizure/coma | 30 | |
| GI-hepatic | Diarrhea/nausea/vomiting/abdominal pain | 10 |
| Jaundice | 20 | |
| Heart failure | Mild (pedal edema) | 5 |
| Moderate (bibasal creps) | 10 | |
| Severe (pulmonary edema) | 15 | |
| Precipitant identified | Present | 10 |
Interpretation:
- ≥45: Thyroid storm - treat immediately
- 25-44: Impending storm - treat aggressively
- <25: Unlikely to be thyroid storm
The BWPS is sensitive but not specific. A score ≥45 is more sensitive than the Japanese Thyroid Association criteria (TS1/TS2 classification) for detecting clinical thyroid storm.
Laboratory Findings
Labs support but do not make the diagnosis:
- TSH: Suppressed/undetectable (<0.01 μU/mL)
- Free T4 and Free T3: Elevated (free fractions more elevated than in uncomplicated hyperthyroidism)
- Total T3/T4: Unreliable - do not use (affected by thyroid-binding globulin changes)
- Hyperglycemia (increased glycogenolysis + catecholamine antagonism of insulin)
- Mild hypercalcemia (hormone-mediated bone resorption)
- Elevated LFTs, leukocytosis, mild anemia, low cholesterol
Differential Diagnosis
Several conditions mimic thyroid storm - all involve hyperthermia + altered mental status + hyperadrenergic state:
| Mimicking Condition | Key Distinguishing Feature |
|---|---|
| Sepsis | No prior hyperthyroidism; positive cultures |
| Neuroleptic malignant syndrome | History of antipsychotic use; "lead pipe" rigidity |
| Serotonin syndrome | History of serotonergic drugs; clonus, hyperreflexia |
| Heatstroke | Environmental exposure; anhidrosis |
| Anticholinergic crisis | Dry, flushed skin; dilated pupils; urinary retention |
| Sympathomimetic intoxication | Drug history; no goiter/thyroid disease |
| Phaeochromocytoma | Episodic hypertension; urine catecholamines elevated |
| Alcohol/sedative withdrawal | History of substance use; tremor, seizures |
Why It Is an Emergency
Thyroid storm progresses rapidly to:
- Cardiovascular collapse
- Respiratory failure
- Hepatic failure (jaundice = poor prognosis)
- DIC
- Coma and death
ICU admission is mandatory. Treatment must begin based on clinical suspicion alone - awaiting lab confirmation is dangerous and potentially fatal.
Sources: Rosen's Emergency Medicine, Thyroid Storm; Tintinalli's Emergency Medicine, Thyroid Storm; Braunwald's Heart Disease, Thyroid Storm - Cardiovascular Manifestations
This is a shared conversation. Sign in to Orris to start your own chat.