Are you bettwr than gpt in case of medical dr
- I'm connected to a curated medical textbook library (indexed with full-text search) covering pharmacology, pathology, anatomy, physiology, clinical medicine, and more
- I follow a medical-first routing rule - for any clinical/health question, I search authoritative textbooks before answering, rather than relying purely on training data
- I also cross-reference PubMed for recent peer-reviewed evidence (systematic reviews, RCTs, meta-analyses)
- I can retrieve and display medical images directly from textbooks - diagrams, histology slides, anatomy illustrations, clinical photos
| Feature | Orris | GPT (standard) |
|---|---|---|
| Textbook library search | Yes (indexed, cited) | No |
| PubMed integration | Yes (live search) | Depends on version/plugins |
| Image retrieval from textbooks | Yes | No |
| Cites specific sources | Yes, with page numbers | Sometimes |
| Up-to-date guidelines | Via PubMed | Via web browsing (GPT-4o) |
- My medical library has a fixed set of textbooks - very broad but not exhaustive
- For highly specialized or brand-new topics, GPT with web browsing may surface more recent content
- I'm not a substitute for a real clinician - neither is GPT
Premature ejaculation and it’s all treatment step by step
"premature ejaculation" treatment
Premature Ejaculation (PE): Complete Step-by-Step Guide
What Is PE?
-
Ejaculation that always or nearly always occurs within ~1 minute of vaginal penetration (lifelong PE) or a significant reduction from a previously normal latency (acquired PE)
-
Inability to delay ejaculation on all or nearly all penetrations
-
Negative personal consequences: distress, frustration, avoidance of sexual intimacy
-
Campbell-Walsh Urology, p. 2074
Types of PE
| Type | Description |
|---|---|
| Lifelong (Primary) PE | Present from first sexual encounter; ejaculation in <1-2 min; neurobiologic basis |
| Acquired (Secondary) PE | Develops after a period of normal ejaculation; often situational; linked to ED, anxiety, thyroid disease |
| Variable PE | Occasional early ejaculation; considered a natural variation, NOT a disorder |
| Subjective PE | Patient complains of PE but has normal latency (2-6 min); psychological/cultural basis |
- Campbell-Walsh Urology, p. 2074
Causes
- Genetic predisposition (serotonin transporter gene variants)
- Neurobiologic hypersensitivity of the ejaculatory reflex
- Low central serotonin neurotransmission
- Erectile dysfunction (performance anxiety leads to rushing to ejaculate)
- Hyperthyroidism
- Chronic prostatitis / chronic pelvic pain syndrome (CPPS)
- Psychological/relationship problems
- Sexual performance anxiety
STEP-BY-STEP EVALUATION
Step 1: Take a Full History
- Time between penetration and ejaculation?
- Is ejaculation in all partners or situational?
- How long has this been a problem - from first encounter or did it develop?
- Is erection normal before ejaculation?
- Any distress to patient or partner?
- Any associated urinary, thyroid, or prostate symptoms?
Step 2: Physical Examination
- Focused genital exam
- Assess for prostatitis, thyroid enlargement, neurological signs
Step 3: Investigations
- Thyroid function tests (if acquired PE is suspected)
- Urine culture (if lower urinary tract symptoms present)
- Erectile function assessment (IIEF questionnaire)
STEP-BY-STEP TREATMENT
FIRST LINE: Psychosexual / Behavioral Techniques
1. Stop-Start Technique (Semans Technique)
- Patient or partner stimulates the penis until ejaculation feels imminent
- Stimulation is stopped completely until the urge passes
- Repeat 3-4 times before allowing ejaculation
- Goal: Build awareness and voluntary control over the ejaculatory reflex
2. Squeeze Technique (Masters & Johnson)
- Same as stop-start, but when near ejaculation, the glans penis is firmly squeezed (by partner, for 10-20 seconds) to suppress the urge
- Released, then stimulation resumes after 30 seconds
- Repeat before ejaculation
3. Sensate Focus Therapy
- Structured exercises to reduce performance anxiety
- Couple engages in non-goal-oriented touching (no intercourse initially)
- Gradually progresses to include genital touching, then intercourse
- Builds intimacy and reduces anxiety
Note: Psychosexual CBT (Cognitive Behavioral Therapy) has a limited role as first-line monotherapy but plays a key role as an adjunct to pharmacotherapy, especially in acquired PE. - Campbell-Walsh Urology, p. 2087
SECOND LINE: Topical Anesthetic Agents
4. Lidocaine-Prilocaine Cream (EMLA Cream)
- Applied to glans penis 20-30 minutes before intercourse
- Washed off before penetration to prevent partner's vaginal numbness
- Reduces penile sensitivity, significantly increases IELT
- Well tolerated; minimal systemic absorption
5. Lidocaine 150mg Metered-Dose Spray (Fortacin/PSD502)
- Applied 5 minutes before intercourse
- The only EMA-approved topical treatment specifically for PE
- Clinical trials show 5-6 fold increase in IELT
- Less messy and more practical than cream
THIRD LINE: Oral Pharmacotherapy
6. Daily SSRIs (Selective Serotonin Reuptake Inhibitors)
| Drug | Dose | IELT Fold-Increase |
|---|---|---|
| Paroxetine | 10-40 mg/day | Greatest efficacy (~8-12 fold) |
| Sertraline | 50-200 mg/day | Moderate |
| Fluoxetine | 20-40 mg/day | Moderate |
| Clomipramine (TCA) | 12.5-50 mg/day | Moderate |
- Full effect takes 1-2 weeks
- Side effects: nausea, fatigue, decreased libido, anorgasmia, sexual dysfunction
- Paroxetine has the highest efficacy among daily SSRIs
7. On-Demand Dapoxetine (FDA / EMA recognized)
- Dapoxetine 30-60 mg, taken 1-3 hours before intercourse
- Only SSRI with a short half-life specifically designed for on-demand use
- 2-3 fold increase in IELT vs placebo
- Side effects: nausea, dizziness, headache, diarrhea
- Not FDA-approved in the USA but approved in many countries
8. On-Demand SSRIs (Off-Label)
- Clomipramine 25 mg or paroxetine 20 mg taken 3-4 hours before sex
- Less effective than daily dosing but preferred by some patients
9. On-Demand Tramadol (Off-Label)
- 50 mg taken 2 hours before intercourse
- Centrally acting opioid analgesic; delays ejaculation via serotonin/noradrenaline reuptake inhibition
- Moderate efficacy (~2.5 fold IELT increase)
- Inferior to daily paroxetine
- Risk of dependence - use with caution; not recommended as routine treatment
- Campbell-Walsh Urology, p. 2087
FOURTH LINE: Treatment of Underlying Cause (Acquired PE)
10. Treat Erectile Dysfunction First
- If ED is driving PE (patient rushes to ejaculate before losing erection), treating ED with a PDE-5 inhibitor (sildenafil, tadalafil) may resolve PE
- PDE-5 inhibitors may also independently modestly prolong IELT
11. Treat Hyperthyroidism
- If thyroid disease is causative, treatment of hyperthyroidism often resolves acquired PE
12. Treat Chronic Prostatitis/CPPS
- Antibiotics, alpha-blockers (e.g., tamsulosin), anti-inflammatory agents
- A 2024 meta-analysis (PMID: 39692416) found that silodosin (a selective alpha-1 blocker) is a promising treatment for PE
13. Treat Psychological/Relationship Issues
- Psychosexual counseling for couples
- Individual CBT for performance anxiety, depression
- Referral to sex therapist when indicated
FIFTH LINE: Emerging / Surgical Treatments (Selected Cases)
14. Selective Dorsal Neurectomy / Cryoablation
- Surgical procedure to reduce penile hypersensitivity by cutting/freezing dorsal penile nerves
- A 2025 meta-analysis (PMID: 40488424) confirms clinical efficacy with acceptable safety
- Reserved for refractory cases; irreversible - must be discussed carefully
15. Hyaluronic Acid Penile Glans Injection
- Injection of hyaluronic acid into the glans to reduce sensitivity
- Evidence is emerging; considered experimental
16. Botulinum Toxin-A Injection
- A 2025 meta-analysis (PMID: 40445933) shows botulinum toxin-A injections significantly increase IELT
- Mechanism: reduces bulbocavernosus muscle contractility
- Still investigational; not standard care
COMBINATION THERAPY
- Topical anesthetic + daily SSRI - additive effect
- Pharmacotherapy + psychosexual therapy - addresses both the biological and psychological components
- Partner involvement is strongly recommended throughout treatment
"Psychosexual CBT has a limited role as a first-line treatment for PE but has an important role as an adjunct to pharmacotherapy." - Campbell-Walsh Urology, p. 2087
Summary Treatment Ladder
Step 1: Psychosexual/behavioral techniques (stop-start, squeeze, sensate focus)
↓ (if insufficient)
Step 2: Topical anesthetics (EMLA cream, lidocaine spray)
↓ (if insufficient)
Step 3: Oral pharmacotherapy
- On-demand: Dapoxetine 30-60mg OR Tramadol 50mg
- Daily: Paroxetine > Sertraline/Fluoxetine/Clomipramine
↓ (treat underlying cause if acquired PE)
Step 4: Treat ED (PDE5i), hyperthyroidism, prostatitis as appropriate
↓ (refractory cases)
Step 5: Surgical options (dorsal neurectomy, botulinum toxin, hyaluronic acid) - specialist only
- Always involve the partner in the treatment plan when possible
- No drug is currently FDA-approved in the USA specifically for PE (all pharmacotherapy is off-label except dapoxetine in other countries)
- Lifelong PE responds better to pharmacotherapy; acquired PE responds better to addressing the cause + CBT
- Reassess thyroid function and erectile function in all new cases of acquired PE
Okay if its primary pe
"lifelong premature ejaculation" treatment SSRIs
Primary (Lifelong) PE - Step-by-Step Treatment
Key Distinction: Why Primary PE is Different
- Hyposensitivity of 5-HT2c receptors AND/OR hypersensitivity of 5-HT1a receptors in the brain
- Low central serotonergic tone in the ejaculatory control pathways
- Likely genetic component (present from the very first sexual encounter)
"Men with L-PE are best managed with PE pharmacotherapy" - Campbell-Walsh Urology, p. 2083
Step-by-Step Treatment for Primary PE
STEP 1: Confirm the Diagnosis
- Ejaculation within <1-2 minutes of penetration
- Present since the very first sexual experience
- Occurs with every or nearly every partner (not situational)
- Causes personal distress or relationship difficulty
- No history of normal ejaculatory control
STEP 2: Education & Counseling (Before Starting Drugs)
- Explain the neurobiologic nature of lifelong PE to reduce shame and self-blame
- Reassure that it is a recognized medical condition with effective treatment
- Set realistic expectations: drugs significantly prolong latency but do not cure - most patients need long-term treatment
- Involve partner if willing - partner cooperation improves outcome
STEP 3: First-Line Drug Treatment - Daily SSRI
Option A: Paroxetine (PREFERRED - highest efficacy)
- Dose: Start 10 mg/day, increase to 20-40 mg/day after 2 weeks if tolerated
- IELT effect: 8-12 fold increase (strongest of all oral agents)
- Onset of ejaculatory delay: within 1-2 weeks, maximum effect by 3-4 weeks
- Side effects: nausea, fatigue, reduced libido, anorgasmia, weight gain, discontinuation syndrome (must taper, never stop abruptly)
Option B: Sertraline
- Dose: 50-200 mg/day
- Moderate efficacy; fewer sexual side effects than paroxetine
- Good tolerability profile
Option C: Fluoxetine
- Dose: 20-40 mg/day
- Long half-life (easier to manage if a dose is missed)
- Takes longer to reach full effect (2-4 weeks)
Option D: Clomipramine (TCA - if SSRIs not tolerated)
- Dose: 12.5-50 mg/day
- Effective but more side effects (dry mouth, constipation, cardiac effects)
- Used when SSRIs are contraindicated or failed
Clinical tip: Try each drug for at least 4-6 weeks at adequate dose before declaring failure and switching.
STEP 4: On-Demand Option - Dapoxetine
- Dapoxetine 30 mg or 60 mg taken 1-3 hours before anticipated intercourse
- The only SSRI with a short half-life (1.5 hours) designed specifically for on-demand PE use
- 2-3 fold IELT increase vs placebo (less effective than daily paroxetine but no daily drug burden)
- Side effects: nausea, dizziness, headache, diarrhea - usually mild and transient
- A 2025 systematic review (PMID: 41020367) confirms that dapoxetine combined with non-pharmacological therapy gives superior results vs dapoxetine alone in lifelong PE
STEP 5: Add Topical Anesthetic (If Drug Alone Insufficient)
Lidocaine-Prilocaine Cream (EMLA)
- Apply a thin layer to the glans penis 20-30 minutes before sex
- Wash off before penetration (to avoid partner numbness)
- Reduces glans sensitivity
Lidocaine Metered-Dose Spray (Fortacin / PSD502)
- Apply 5 minutes before intercourse (more convenient than cream)
- 5-6 fold IELT increase in trials
- Combination of topical + SSRI gives synergistic benefit
STEP 6: Add Behavioral Therapy as Adjunct
- Stop-Start technique - during intercourse, pause stimulation when ejaculation is imminent; resume after urge passes; repeat 3-4 times
- Squeeze technique - partner squeezes the glans firmly for 10-20 seconds when ejaculation is imminent
- Pelvic floor exercises - strengthening the bulbocavernosus and ischiocavernosus muscles may improve voluntary control
STEP 7: Assess Response and Escalate if Needed
| Scenario | Action |
|---|---|
| Good response | Consider gradual drug withdrawal to see if sustained; if relapse, restart long-term |
| Partial response | Increase SSRI dose OR add topical agent OR switch to combination |
| No response to one SSRI | Switch to another SSRI (response to paroxetine vs sertraline can differ) |
| SSRI side effects intolerable | Switch to dapoxetine (on-demand) or clomipramine |
STEP 8: On-Demand Tramadol (Off-Label, Last Oral Resort)
- Tramadol 50 mg taken 2 hours before sex
- Modest efficacy (~2.5 fold IELT increase)
- Risk of dependence and addiction - use very cautiously and short-term only
- Inferior to paroxetine
STEP 9: Long-Term Management
- Long-term or indefinite pharmacotherapy
- Periodic reassessment (every 3-6 months)
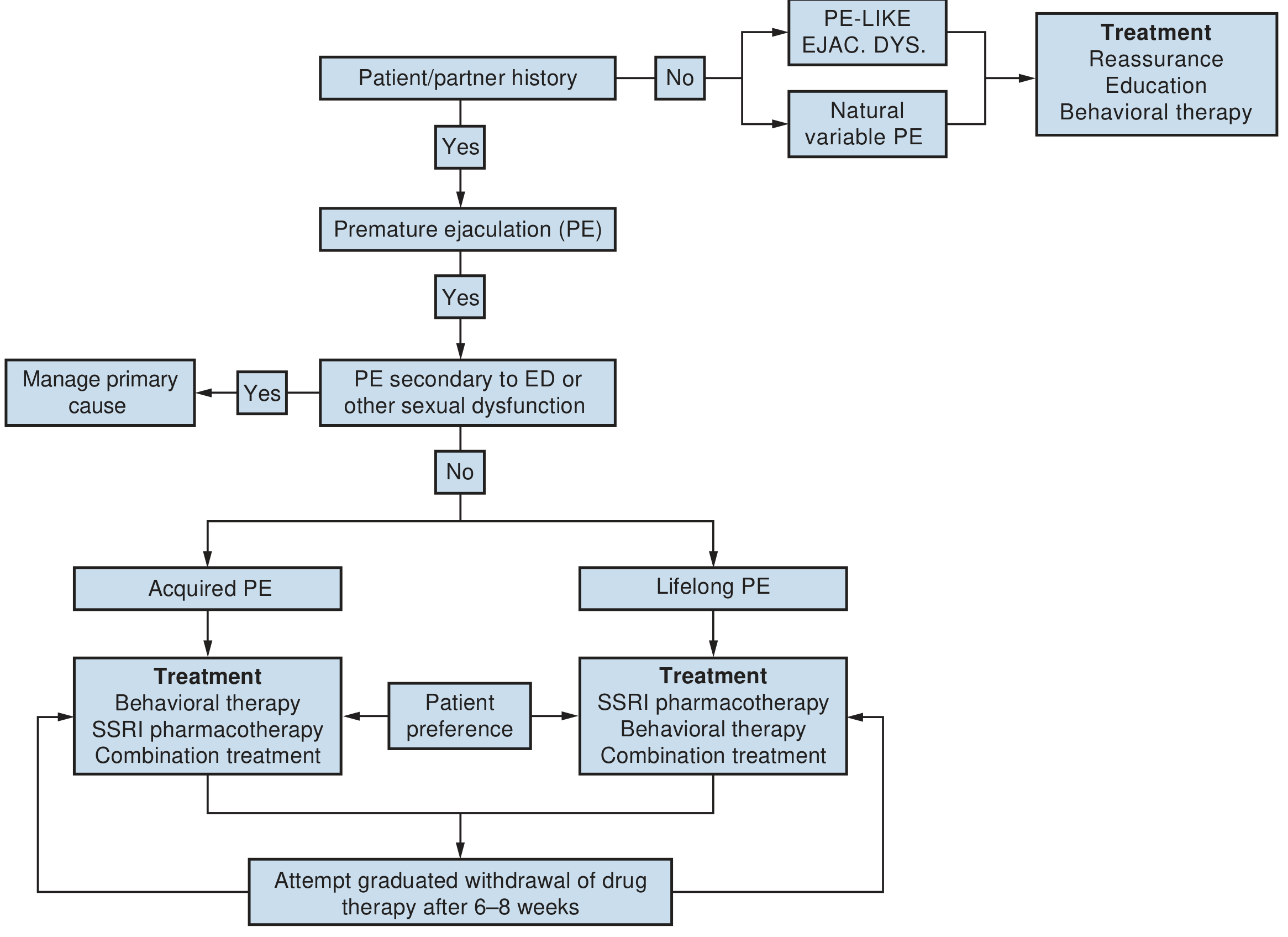
- Attempt gradual drug withdrawal after 6-8 weeks of treatment to reassess if it is still needed (as shown in the algorithm above)
- Psychological support for any residual self-esteem or relationship issues
Summary: Treatment Priority for Primary/Lifelong PE
STEP 1: Confirm diagnosis (lifelong, from first encounter, with all partners)
STEP 2: Educate patient + involve partner
STEP 3: Daily SSRI → Paroxetine (first choice) or Sertraline/Fluoxetine
STEP 4: If daily drugs refused → Dapoxetine on-demand
STEP 5: Add topical anesthetic (EMLA or lidocaine spray) for extra effect
STEP 6: Add behavioral therapy (stop-start / squeeze) as adjunct
STEP 7: Review at 6-8 weeks → dose-adjust or switch if needed
STEP 8: Tramadol if SSRIs completely contraindicated (use cautiously)
STEP 9: Long-term plan - most patients need continued treatment
Bottom line for primary PE: Pharmacotherapy (SSRI) is the cornerstone - not behavioral therapy alone. Behavioral therapy is helpful as an add-on but cannot correct the underlying neurobiologic deficit by itself.
In general in how many months or years the patient improves without need of medication anymore
"premature ejaculation" long-term outcome drug discontinuation remission
"premature ejaculation" SSRI withdrawal recurrence
lifelong primary premature ejaculation spontaneous remission without medication prognosis
Honest Prognosis: Will Primary PE Ever Go Away Without Medication?
What the Evidence Actually Says
Primary PE Has No Definitive Cure
"Lifelong premature ejaculation has no definitive cure. In many cases, pharmacological therapy must be continued indefinitely, as discontinuation may lead to the recurrence of premature ejaculation."
What Happens When You Stop Medication?
In a clinical series of 32 men on paroxetine 20 mg/day for 2 months:
- 28 out of 32 patients (87.5%) had PE recurrence within 2-3 weeks after stopping therapy
- AUA Pharmacologic Management of PE Guidelines
Success Rates Are Moderate, Relapses Are Common
- Treatment success rates: 30% to 70%
- Relapses are common
- Some men need lifelong therapy
The Practical Timeline Reality
| Scenario | What to Expect |
|---|---|
| On daily SSRI | Good control within 1-4 weeks; maintained as long as drug is taken |
| Stop drug after 6-8 weeks | ~87% relapse within 2-3 weeks |
| Long-term behavioral therapy alone | Modest sustained improvement possible, but rarely drug-free "cure" for lifelong PE |
| Combination drug + behavioral therapy | Best chance of sustained improvement; a 2025 meta-analysis (PMID: 41020367) shows this combination gives superior long-term outcomes vs drugs alone |
| Acquired PE (not primary) | Much better - treating the cause (ED, thyroid, prostatitis) can fully resolve it |
Is There Any Hope of Coming Off Medication?
- They have combined drug treatment with intensive behavioral therapy (stop-start, squeeze, pelvic floor training) - the learned control can persist to some degree
- They have addressed psychological contributors (performance anxiety, relationship issues) through CBT/sex therapy
- Their PE was on the milder end of the spectrum (1-2 min IELT, not <30 seconds)
Bottom Line
| Type | Drug-free remission? |
|---|---|
| Primary/Lifelong PE | Unlikely - most need long-term or indefinite pharmacotherapy. Behavioral skills can help but rarely eliminate the need for drugs entirely |
| Acquired/Secondary PE | Yes - once the underlying cause is treated, many men no longer need PE-specific medication |
How much chances the conditions will Improve on medication?
"premature ejaculation" SSRI dapoxetine efficacy IELT improvement
PMID: 40326158
premature ejaculation medication success rate percentage patients improve SSRI dapoxetine clinical data
Chances of Improvement on Medication - Real Clinical Data
The Short Answer
1. How Much Does Ejaculation Time (IELT) Actually Increase?
| Drug | Average IELT Increase vs Baseline | vs Placebo |
|---|---|---|
| Paroxetine (daily) | +5.64 minutes (best of all drugs) | Most effective overall |
| Dapoxetine 60 mg | +2.7 minutes from baseline | ~3x fold increase |
| Dapoxetine 30 mg | +2.3 minutes from baseline | ~2.5x fold increase |
| Topical anesthetics | Significant increase | 5-6x fold |
| Tramadol | +2.49 minutes | ~2.5x fold |
A man ejaculating in 30-45 seconds could go to 3-6 minutes on paroxetine. That is a transformative change for most patients.
2. What Percentage of Patients Feel "Better"?
| Outcome | Placebo | Dapoxetine 30mg | Dapoxetine 60mg |
|---|---|---|---|
| PE rated "better" or "much better" | 13.9% | 30.7% | 38.3% |
| PE rated "at least slightly better" | 36.0% | 62.1% | 71.7% |
| Partners satisfied ("good"/"very good") | 24.0% | 37.5% | 44.7% |
3. Dapoxetine - Real-World "Effectiveness" Rate
64.2% of patients achieved the predefined therapeutic threshold of meaningful IELT improvement
- Mean IELT increased by +1.63 minutes from baseline
- Consistent across all age groups and BMI categories
4. Distress Reduction - Often the Most Important Outcome
| Outcome | Placebo | Dapoxetine 30mg | Dapoxetine 60mg |
|---|---|---|---|
| "Quite a bit / extreme" personal distress | 39% | 28.2% | 22.2% |
| Interpersonal difficulty | 23.8% | 16.0% | 12.3% |
5. The Honest Catch - Dropout Rate is High
| Timepoint | % who stopped taking dapoxetine |
|---|---|
| 1 month | 26.4% |
| 3 months | 61.6% |
| 6 months | 79.1% |
| 12 months | 87.3% |
| 24 months | 90.1% |
- Cost (30%)
- Frustration that PE is not "cured" and drug is needed every time (25%)
- Side effects (11.6%)
- Perceived poor efficacy (9.8%)
Summary: What to Tell a Patient
| Question | Answer |
|---|---|
| Will my ejaculation time increase? | Yes - almost certainly. Most men get 2-6x improvement in IELT |
| Will I feel better overall? | ~60-70% yes - at least partial improvement |
| Will I feel "much better"? | ~30-40% report marked improvement |
| Will my distress and anxiety reduce? | Yes - significant reduction in personal and relationship distress |
| Is paroxetine or dapoxetine better? | Paroxetine gives the largest IELT increase (+5.64 min) but requires daily dosing; dapoxetine is on-demand and more convenient |
| Combination (drug + topical + therapy)? | Best overall results - additive effects |
Bottom line: Medication has a high chance of meaningful improvement in ejaculation time and quality of life. The key is setting the right expectation - it controls PE very well, but it is a management tool, not a permanent cure for primary PE.