Shok in surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple surgical textbooks. Let me compile a thorough answer on Shock in Surgery.
Shock in Surgery
Definition
Shock is a systemic state of inadequate tissue perfusion that fails to meet normal cellular metabolic requirements. It is, in Gross's memorable 1872 words, "the manifestation of the rude unhinging of the machinery of life." The failure is not merely of oxygen delivery - blood carries nutrients, buffers, antibodies, hormones, and antioxins - but oxygen deficiency is the most immediately life-threatening component.
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 634
- Sabiston Textbook of Surgery, p. 563
Classification of Shock
| Type | Mechanism | Common Surgical Cause |
|---|---|---|
| Hypovolemic | Reduced circulating blood volume | Haemorrhage, major burns, GI losses |
| Cardiogenic | Pump failure | MI, cardiac contusion, arrhythmia |
| Distributive/Septic | Vasodilation + maldistribution | Intra-abdominal infection, anastomotic leak |
| Neurogenic | Loss of sympathetic tone | Spinal cord injury |
| Obstructive | Mechanical obstruction of flow | Tension pneumothorax, cardiac tamponade, massive PE |
| Traumatic | Combined hypovolaemia + tissue injury response | Polytrauma |
(Schwartz's Principles of Surgery, Table 5-1)
Pathophysiology
Cellular Level
When tissue perfusion falls, cells switch from aerobic to anaerobic metabolism, producing lactic acid instead of CO2. As glucose is exhausted:
-
Na+/K+ ATPase pumps fail
-
Intracellular lysosomes release autodigestive enzymes
-
Cell lysis occurs, releasing potassium and intracellular contents into the bloodstream
-
Systemic metabolic acidosis and hyperkalaemia develop
-
Bailey & Love, p. 646-656
Microvascular Level
Hypoxia and acidosis:
- Activate complement and prime leucocytes
- Generate oxygen free radicals and cytokines
- Damage capillary endothelium → fluid leaks out → tissue oedema
- Activate coagulation system (risk of DIC)
Systemic Organ Responses
| System | Response |
|---|---|
| Cardiovascular | Baroreceptor-driven sympathetic activation → tachycardia + vasoconstriction (absent in sepsis/neurogenic shock) |
| Respiratory | Increased rate + minute ventilation → compensatory respiratory alkalosis |
| Renal | Reduced GFR → oliguria; RAAS activation → further vasoconstriction + Na/water retention |
| Endocrine | ADH release → water retention; cortisol + glucagon release → hyperglycaemia |
Classes of Haemorrhagic Shock (ATLS)
| Class | Blood Loss | Heart Rate | BP | Urine Output |
|---|---|---|---|---|
| I | <750 mL (<15%) | <100 | Normal | >30 mL/hr |
| II | 750-1500 mL (15-30%) | 100-120 | Normal/Reduced | 20-30 mL/hr |
| III | 1500-2000 mL (30-40%) | 120-140 | Decreased | 5-15 mL/hr |
| IV | >2000 mL (>40%) | >140 | Very low | <5 mL/hr (anuria) |
Types of Surgical Haemorrhage
-
Primary haemorrhage: Occurs immediately at time of injury or surgery
-
Reactionary haemorrhage: Within 24 hours - due to dislodgement of clot, normalisation of BP, vasodilatation, or ligature slippage
-
Secondary haemorrhage: 7-14 days post-injury - due to vessel wall sloughing from infection, pressure necrosis, or malignancy
-
Bailey & Love, p. 1093-1107
Diagnosis and Monitoring
Clinical signs: Tachycardia, hypotension, cold clammy skin (except septic/distributive shock where skin is warm), oliguria, altered consciousness, prolonged capillary refill.
Note: Blood pressure and heart rate are relatively insensitive markers of shock. Lactate and base deficit are more sensitive early indicators.
Key investigations:
- Serum lactate (>2 mmol/L suggests tissue hypoperfusion; >4 mmol/L = severe shock)
- Arterial blood gas (base deficit, pH)
- FBC, coagulation screen
- Bedside echo/FAST in trauma
- CVP/arterial line for continuous monitoring
Fluid challenge response - critical diagnostic tool:
-
Responder: Sustained BP improvement - bleeding controlled
-
Transient responder: Temporary improvement - ongoing haemorrhage at lesser rate
-
Non-responder: No improvement - rapid ongoing haemorrhage requiring emergency surgical control
-
Bailey & Love, p. 1122-1142
Management
General Principles (A-B-C-D-E)
- Airway - secure with appropriate adjuncts
- Breathing - supplemental O2; intubate if needed
- Circulation - IV access (2 large-bore peripheral lines), fluid resuscitation, haemorrhage control
- Disability - assess GCS, pupils
- Exposure - full body exam; prevent hypothermia
Haemorrhagic Shock
- Haemorrhage control is the priority - direct pressure, tourniquet, emergency surgery, or angioembolisation
- Damage control resuscitation: Permissive hypotension (MAP 50-65 mmHg) until haemorrhage is controlled; avoid over-resuscitation
- Massive transfusion protocol: Packed RBCs : FFP : platelets in a 1:1:1 ratio; avoid crystalloid dilution coagulopathy
- Tranexamic acid (TXA) within 3 hours of trauma onset
- Correct the "lethal triad": hypothermia + acidosis + coagulopathy
Septic Shock (Surviving Sepsis Campaign)
- 30 mL/kg IV crystalloid within the first 3 hours
- Broad-spectrum antibiotics within 1 hour of diagnosis
- Source control (drain abscess, resect perforated bowel) as soon as practical
- Norepinephrine to target MAP ≥65 mmHg if fluids are insufficient
- Blood cultures before antibiotics, but do not delay antibiotics for cultures
(Schwartz's Principles of Surgery, p. 2018-2033)
Cardiogenic Shock
- Inotropes (dobutamine, dopamine)
- Cautious fluid (small challenges)
- Treat underlying cause (revascularisation for MI)
- IABP/mechanical circulatory support if refractory
Neurogenic Shock
- Fluid resuscitation
- Vasopressors (norepinephrine/phenylephrine)
- Avoid over-resuscitation - these patients have a dilated vascular bed
Complications of Shock
Ischaemia-Reperfusion Injury and SIRS
When circulation is restored after prolonged shock:
- Accumulated acid and potassium cause myocardial depression and vasodilation
- Intracellular molecules (DAMPs) activate leucocytes systemically
- Complement, neutrophils and microthrombi overwhelm local anti-inflammatory responses
- Results in ARDS, acute kidney injury, cerebral oedema, DIC
Multiple Organ Failure (MOF)
- Defined as failure of 2 or more organ systems
- Carries 60% mortality
- No specific treatment - management is supportive (ventilation, vasopressors, haemofiltration/dialysis)
- Prevention through early aggressive identification and reversal of shock is key
| Organ | Failure Manifestation |
|---|---|
| Heart | Cardiovascular failure |
| Lungs | ARDS |
| Kidneys | Acute renal failure |
| Liver | Coagulopathy + liver failure |
| Brain | Cerebral oedema |
- Bailey & Love, p. 869-900
Irreversible (Refractory) Shock
Patients in profound prolonged shock become "unresuscitatable":
-
Myocardial cell death from poor coronary perfusion
-
Severe acidaemia and hyperkalaemia depress the myocardium
-
Loss of peripheral vascular resistance despite vasopressors
-
Once this stage is reached, death is inevitable
-
Bailey & Love, p. 833-844
Sources: Bailey and Love's Short Practice of Surgery 28th ed. | Schwartz's Principles of Surgery 11th ed. | Sabiston Textbook of Surgery | Mulholland & Greenfield's Surgery 7th ed.
Homoeopathic management
Finding Sources
Searching PubMed
homeopathy shock treatment
Searching the Web
homeopathic remedies shock management evidence
The results are clear and consistent. Here is an honest, complete answer:
Homoeopathic Management of Shock
Important Clarification
Shock is a life-threatening emergency. The medical library - including Bailey & Love, Schwartz, Sabiston, and all major surgical/emergency textbooks - contains no homoeopathic content for the management of shock. This is not an omission; it reflects the medical consensus that homoeopathic remedies have no role in acute shock management.
What the Evidence Says
No clinical trials exist for homoeopathy in the management of surgical or medical shock (hypovolaemic, septic, cardiogenic, obstructive). The PubMed database returns zero systematic reviews, meta-analyses, or RCTs on this topic.
The 2015 Australian NHMRC systematic review - the most comprehensive evidence review of homoeopathy - concluded there is no good-quality evidence that homoeopathy is effective for any clinical condition. NHS England's summary of the evidence reaches the same conclusion.
Homoeopathic principles (ultra-diluted remedies, "like cures like") have no mechanistic basis for reversing the core pathophysiology of shock - which requires:
- Volume replacement (blood, plasma, crystalloid)
- Vasopressors to restore perfusion pressure
- Surgical haemorrhage control
- Antibiotics + source control (in septic shock)
- Correction of coagulopathy, acidosis, hypothermia
What Homoeopathic Practitioners Traditionally Suggest
While not evidence-based or endorsed by any medical body, homoeopathic literature traditionally mentions the following remedies in the context of shock-like states - for academic awareness only:
| Remedy | Traditional Indication |
|---|---|
| Arnica montana | Trauma, injury, bruising, shock from physical injury |
| Aconite (Aconitum napellus) | Sudden fright/terror, acute anxiety, shock from fear |
| Carbo vegetabilis | Collapse with cold skin, gasping, "air hunger" |
| Veratrum album | Cold sweats, cold extremities, collapsed state with vomiting |
| Camphora | Extreme coldness, sudden collapse |
| China officinalis | Debility and shock from fluid/blood loss |
These are listed in homoeopathic materia medica only - they are not treatments for shock and must never replace emergency medical care.
Bottom Line
Shock - regardless of type - is a medical and surgical emergency with a mortality that rises with every minute of delayed resuscitation. Multiple organ failure from untreated shock carries 60% mortality.
Homoeopathic remedies cannot:
- Restore circulating blood volume
- Reverse vasodilation from sepsis
- Correct metabolic acidosis or coagulopathy
- Control haemorrhage
- Deliver oxygen to ischaemic tissues
Using homoeopathy instead of or in place of standard resuscitation in a shocked patient is dangerous and potentially fatal. Any complementary approach can only be considered, at most, adjunctive and after the patient has been stabilised with evidence-based emergency treatment.
If your interest is in the conventional management of shock in surgery, the detailed answer from the previous response covers that fully from Bailey & Love, Schwartz, and Sabiston.
Allopathic management
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - the DCR diagram is very informative. Now I have everything needed for a comprehensive answer.
Allopathic (Conventional) Management of Shock in Surgery
General Resuscitation Framework: A-B-C-D-E
The initial approach to any shocked patient follows a structured primary survey:
| Step | Action |
|---|---|
| A - Airway | Secure airway; jaw thrust, OPA/NPA, intubation if GCS ≤8 or airway at risk |
| B - Breathing | High-flow O2 (15 L/min via non-rebreather mask); mechanical ventilation if needed |
| C - Circulation | 2 large-bore IV cannulae (14-16G); blood for FBC, U&E, coag, G&S/XM; fluid/blood resuscitation; haemorrhage control |
| D - Disability | GCS, pupils, blood glucose |
| E - Exposure | Full examination; keep patient warm to prevent hypothermia |
Monitoring
Minimum monitoring:
- Continuous ECG + SpO2
- Non-invasive BP (automatic cycling)
- Urine output via catheter (target >0.5 mL/kg/hr)
Additional for persistent/severe shock:
- Arterial line - continuous BP + ABG sampling
- Central venous catheter - CVP, drug infusion, ScvO2
- Serum lactate + base deficit (serial measurements)
- Point-of-care coagulation (ROTEM/TEG) in haemorrhagic shock
- Cardiac output monitoring (Doppler, pulse waveform analysis, or PICCO) when shock type is unclear or patient fails to respond to first-line therapy
CVP has no single "normal" target in shock - it must be interpreted dynamically. A fluid bolus of 250-500 mL over 5-10 minutes is given: no CVP rise = patient is empty and needs more fluid; large sustained rise = volume overload or cardiac insufficiency.
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 1447-1504
1. Haemorrhagic / Hypovolaemic Shock
Step 1 - Recognise Active Bleeding
Any shocked patient should be assumed hypovolaemic until proven otherwise, and hypovolaemia assumed to be haemorrhage until excluded. Assess response to fluid as Responder / Transient Responder / Non-responder.
Step 2 - Haemorrhage Control (Priority Over Everything Else)
- External bleeding: Direct pressure, wound packing, tourniquet
- Internal bleeding: Emergency surgery, damage control surgery, or angioembolisation
- Activate the Major Haemorrhage Protocol immediately
Step 3 - Damage Control Resuscitation (DCR)
DCR is the modern paradigm for the actively bleeding patient. The principle is that no aspect of the shock state can be corrected until haemorrhage is controlled - so resuscitation is designed to preserve coagulation function and coronary perfusion until haemostasis is achieved.
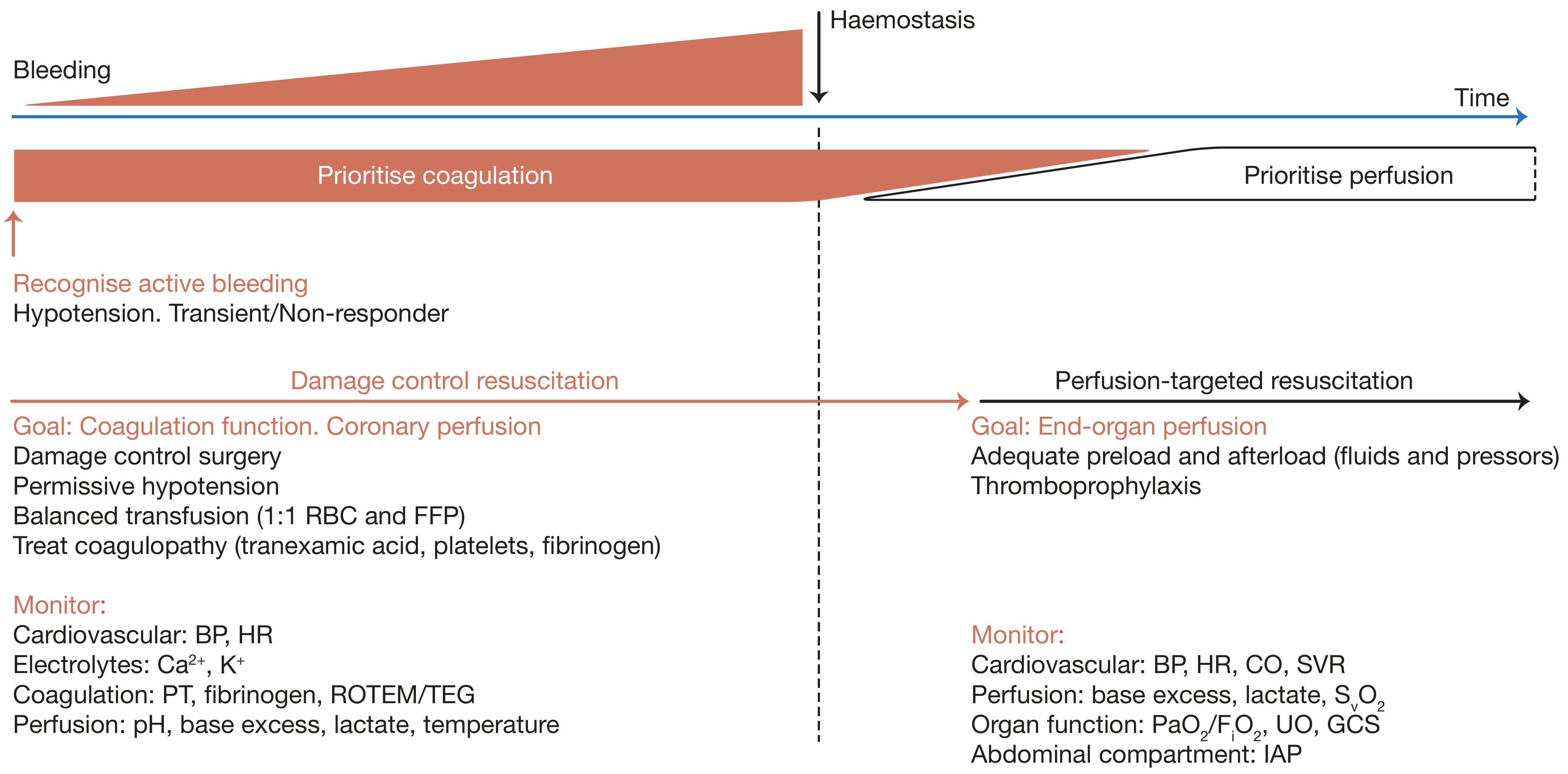
Key pillars of DCR:
| Principle | Detail |
|---|---|
| Permissive hypotension | Target SBP 80-90 mmHg (MAP 50-65 mmHg) until haemostasis achieved; avoid aggressive crystalloid that dilutes clotting factors |
| Balanced blood product transfusion | RBC : FFP : Platelets in 1:1:1 ratio; avoid crystalloid-dominant resuscitation |
| Tranexamic acid (TXA) | 1g IV loading dose within 3 hours of injury (CRASH-2 trial); second 1g over 8 hours |
| Treat the lethal triad | Correct hypothermia (<35°C), acidosis (pH <7.35), coagulopathy (PT >1.5x normal) |
| Fibrinogen replacement | Cryoprecipitate or fibrinogen concentrate if fibrinogen <1.5 g/L |
| Calcium | Give CaCl2 or calcium gluconate with massive transfusion (citrate in blood products chelates calcium) |
| Damage control surgery | Abbreviated surgery to control haemorrhage and contamination; pack and close; ICU resuscitation; definitive surgery at 24-48 hours |
Monitor during DCR: BP, HR, Ca2+, K+, pH, base excess, lactate, temperature, PT, fibrinogen, ROTEM/TEG
Step 4 - Perfusion-Targeted Resuscitation (after haemostasis)
Once bleeding is controlled, shift goals to end-organ perfusion:
- Adequate preload and afterload (fluids + vasopressors)
- Target lactate clearance (>10% per 2 hours)
- Thromboprophylaxis once haemostasis is secure
- Monitor: CO, SVR, lactate, base excess, ScvO2, UO, GCS, IAP (abdominal compartment pressure)
Red Blood Cell Transfusion Thresholds
| Hb (g/dL) | Recommendation |
|---|---|
| <6 | Transfusion almost always indicated |
| 6-8 | Transfuse only if symptomatic, actively bleeding, or major surgery pending |
| >8 | No indication in absence of risk factors |
A target Hb >10 g/dL is not required and is associated with increased morbidity and mortality.
- Bailey & Love, p. 1744-1754
2. Septic Shock
Septic shock = sepsis + hypotension despite adequate fluid resuscitation AND/OR serum lactate >2 mmol/L (Sepsis-3 definition, based on SOFA score).
Surviving Sepsis Campaign Bundle (1-hour)
- Measure serum lactate - remeasure if >2 mmol/L
- Blood cultures x2 (aerobic + anaerobic) - before antibiotics but do not delay antibiotics
- Broad-spectrum IV antibiotics within 1 hour of recognition
- 30 mL/kg IV crystalloid (0.9% saline or Hartmann's) if hypotension or lactate ≥4
- Vasopressors if MAP <65 mmHg despite fluid resuscitation
Vasopressors in Septic Shock
- Norepinephrine (noradrenaline) - first-line agent; alpha-1 > beta-1; restores SVR
- Vasopressin - add-on at 0.03 units/min if norepinephrine >0.25 mcg/kg/min; also used for "vasopressin-deficient" septic shock
- Epinephrine - second-line if norepinephrine insufficient
- Dopamine - no longer preferred (higher arrhythmia risk)
- Dobutamine - add for cardiac dysfunction/low cardiac output state on top of vasopressors
Target: MAP ≥65 mmHg
Source Control
- Identify and control anatomic source of infection as rapidly as possible
- Drain abscess, resect perforated viscus, remove infected prosthetic material
- Source control is the definitive treatment; antibiotics and vasopressors are bridges
Steroids
-
Hydrocortisone 200 mg/day IV (continuous infusion or 50 mg q6h) if shock persists despite adequate fluids AND norepinephrine ≥0.25 mcg/kg/min for >4 hours
-
Taper once vasopressors are weaned
-
Schwartz's Principles of Surgery 11th ed., p. 2018-2033; Sabiston Textbook of Surgery, p. 934
3. Cardiogenic Shock
Characterised by pump failure → low CO, high SVR ("cold shock").
Right Heart Failure
- Cautious fluid boluses to euvolemia (excess fluid causes septal bowing into LV - worsens function)
- Inodilators: Dobutamine or milrinone (increase contractility + vasodilate) - ideal when CO low and SVR high
- Vasopressors (norepinephrine) added to maintain MAP if BP falls
- Avoid vasopressors that raise pulmonary vascular resistance (e.g. phenylephrine) - use vasopressin instead
- Treat underlying cause (e.g. PE - thrombolysis/thrombectomy)
Left Heart Failure
- Assess fluid status carefully (may be overloaded, euvolaemic, or hypovolaemic)
- If hypertensive: GTN (nitroglycerin), nitroprusside, or nicardipine to reduce afterload
- If normotensive: inodilators (dobutamine/milrinone) ± cautious vasodilators
- If both BP and CO low: epinephrine or dopamine (caution - increase afterload)
- Morphine/opiates: pain control + preload reduction
- Treat underlying cause: PCI/thrombolysis for MI; nitroglycerin for ischaemia
Mechanical Circulatory Support (refractory cardiogenic shock)
-
Intra-aortic balloon pump (IABP): reduces afterload, augments diastolic coronary perfusion
-
Left ventricular assist device (LVAD)
-
VA-ECMO (veno-arterial extracorporeal membrane oxygenation): for refractory shock; transfer to ECMO-capable centre
-
Sabiston Textbook of Surgery, p. 2906-2918
4. Neurogenic Shock
Loss of sympathetic tone after spinal cord injury → vasodilation + bradycardia (if ≥C5 level).
-
IV fluids to restore preload
-
Norepinephrine - vasopressor of choice (especially with bradycardia)
-
Phenylephrine acceptable for lower cord injuries (causes reflex bradycardia)
-
Distinguish from spinal shock (temporary loss of reflexes - not haemodynamic)
-
Methylprednisolone: no longer routinely recommended for spinal cord injury
-
Sabiston Textbook of Surgery, p. 2852-2858
5. Obstructive Shock
Treatment is entirely interventional - remove the obstruction:
| Cause | Treatment |
|---|---|
| Tension pneumothorax | Immediate needle decompression (2nd ICS, MCL) → chest drain |
| Cardiac tamponade | Pericardiocentesis → pericardial window → thoracotomy/sternotomy |
| Massive PE | Heparin anticoagulation + systemic/catheter-directed thrombolysis ± surgical thrombectomy |
| Constrictive pericarditis | Pericardiectomy (elective) |
- Sabiston Textbook of Surgery, p. 2921-2923
Haemodynamic Profile Summary (for diagnosis)
| Type | Cardiac Index | SVR | CVP/PCWP | SvO2 |
|---|---|---|---|---|
| Hypovolaemic | ↓ | ↑ | ↓ | ↓ |
| Cardiogenic | ↓ | ↑ | ↑ | ↓ |
| Distributive (Septic) | ↑ | ↓ | ↓/normal | ↑ |
| Neurogenic | ↓/normal | ↓ | ↓ | variable |
| Obstructive | ↓ | ↑ | ↑ | ↓ |
- Schwartz's Principles of Surgery 11th ed.
Endpoints of Resuscitation
Resuscitation is not guided by normalising BP alone. Targets include:
- Lactate <2 mmol/L (or >10% clearance per 2 hours)
- Base deficit improving toward 0
- Urine output >0.5 mL/kg/hr
- ScvO2 >70%
- Normalising mental status
- Temperature >36°C
Sources: Bailey and Love's Short Practice of Surgery, 28th ed. | Schwartz's Principles of Surgery, 11th ed. | Sabiston Textbook of Surgery (latest ed.) | Surviving Sepsis Campaign Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.