
IMG20260612170728.jpg
80 yr old male with h/o of accidental fall came with swelling over auricle for 2 days
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Diagnosis: Auricular Hematoma (Post-Traumatic)
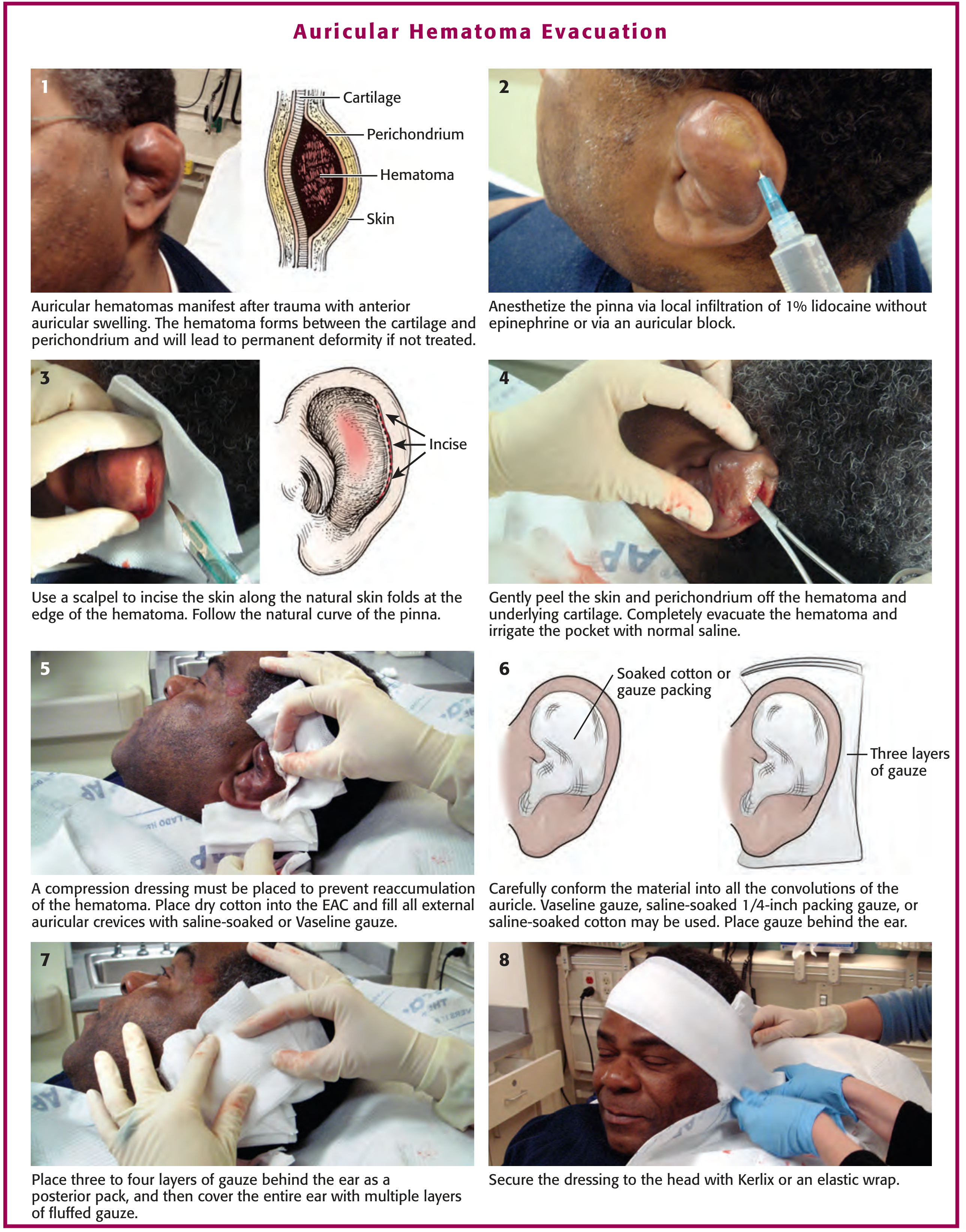
The clinical image shows a smooth, tense, fluctuant swelling over the anterior surface of the auricle with effacement of the normal auricular landmarks - classic appearance of an auricular hematoma following accidental fall.
Pathophysiology
Blunt trauma to the auricle causes a shearing injury that separates the auricular cartilage from its overlying perichondrium, creating a subperichondrial space into which blood collects. Since the avascular cartilage depends entirely on the perichondrium for its blood supply, this separation renders the cartilage ischemic. If untreated, fibrosis and neocartilage formation produce the permanent deformity known as "cauliflower ear."
- Shambaugh Surgery of the Ear, p. 1597
Clinical Features in This Patient
| Feature | Finding |
|---|---|
| Age | 80 yr - elderly, at higher risk for poor healing |
| Mechanism | Accidental fall (blunt trauma to pinna) |
| Duration | 2 days (still acute - within the treatable window) |
| Appearance | Smooth, tense anterior auricular swelling with loss of normal landmarks |
The 2-day duration is still within the acute treatment window (up to 7 days). Beyond 7 days, granulation tissue makes drainage difficult and specialist referral is mandatory.
Management
Step 1 - Anesthesia
Local infiltration with 1% lidocaine WITHOUT epinephrine (epinephrine causes vasoconstriction and may worsen cartilage ischemia), or an auricular nerve block.
Step 2 - Evacuation
Incision and Drainage (preferred over needle aspiration alone)
- Needle aspiration alone has a high reaccumulation rate and is no longer recommended by most authorities as sole treatment
- Incision: Use a No. 15 blade along the natural skin folds at the helical edge of the hematoma, following the curvature of the pinna
- Gently peel the skin and perichondrium off the hematoma and underlying cartilage
- Completely evacuate the hematoma and irrigate the pocket with normal saline
Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1535-1536
Step 3 - Pressure Dressing (CRITICAL to prevent reaccumulation)
This is the most important step. Without it, the hematoma will reaccumulate:
- Place dry cotton into the external auditory canal (EAC)
- Fill all auricular convolutions with Vaseline gauze or saline-soaked gauze, conforming to every crevice
- Place 3-4 layers of gauze behind the ear
- Cover the entire ear with multiple layers of fluffed gauze
- Secure to the head with Kerlix or an elastic wrap
Alternatively: Dental rolls (bolsters) sutured through-and-through to the anterior and posterior surfaces of the auricle are a well-validated method. The bolster is left in place for 4-7 days.
Roberts and Hedges' Clinical Procedures in Emergency Medicine - Fig. 63.23
Step 4 - Antibiotics
Prophylactic antistaphylococcal antibiotics are recommended (e.g., cefalexin or co-amoxiclav). In this elderly patient, consider the risk of infection given reduced immune response.
Step 5 - Follow-Up
Close follow-up is mandatory (every 24-48 hours in the first week) to detect and promptly drain any reaccumulation.
Special Considerations in an 80-Year-Old
- Anticoagulant use? Check if patient is on warfarin, aspirin, or DOACs - this increases bleeding risk and reaccumulation
- Diabetes or immunosuppression? Increases risk of secondary perichondritis (infection presenting with fever, erythema, and exquisite tenderness) - most commonly Pseudomonas aeruginosa; treat with ciprofloxacin
- Skin fragility: Use gentle pressure dressings to avoid pressure necrosis of the fragile elderly pinna skin
- Referral: If patient is on anticoagulants, has signs of infection, or you are not confident in the procedure, refer to ENT
If Left Untreated
Fibrosis + new cartilage formation = permanent "cauliflower ear" deformity. For chronic hematoma or established cauliflower ear, surgical debridement of fibrosis and cartilage is required by an ENT specialist.
- Textbook of Family Medicine 9e, p. 401
- K.J. Lee's Essential Otolaryngology
How to give auricular nerve block
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Auricular Nerve Block - Complete Guide
Nerve Supply of the External Ear (Know This First)
The pinna is supplied by 4 nerve branches - you must block all of them for complete anesthesia:
| Nerve | Origin | Area Supplied |
|---|---|---|
| Great auricular nerve | Cervical plexus (C2, C3) | Most of posteromedial, posterolateral, and inferior auricle |
| Lesser occipital nerve | Cervical plexus (C2) | Posterior auricle (minor contribution) |
| Auriculotemporal nerve | V3 (mandibular branch of trigeminal) | Anterosuperior and anteromedial auricle |
| Auricular branch of vagus (Arnold's nerve) | CN X | Concha and area around auditory meatus |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1526
Equipment
- 10 mL syringe
- 25- or 27-gauge needle, 5-7 cm long
- 1% lidocaine (preferred for most cases) OR 0.25% bupivacaine (for longer procedures)
- Do NOT use epinephrine if there is evidence of traumatized vascularity (as in hematoma). Epinephrine is acceptable only for a regional block in a non-traumatized area
Patient Positioning
Patient lies supine or sits upright in a comfortable position. Turn the head slightly to expose the ear.
Technique: Circumferential Field Block (Most Common Method)
This is a simple "ring block" around the base of the ear using 4 injection points:
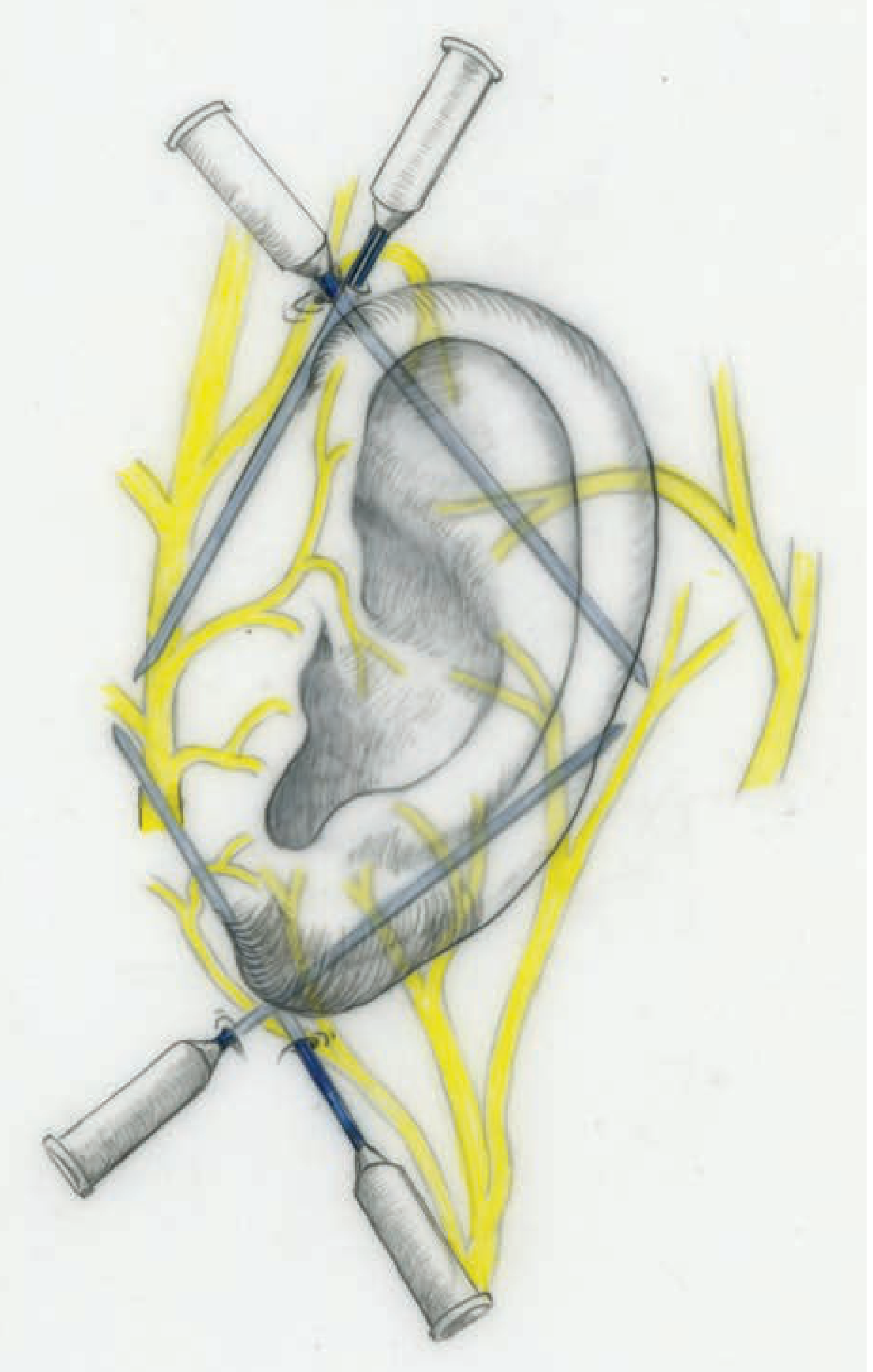
Tintinalli's Emergency Medicine - Fig. 36-17: The four needles encircle the auricular base, with yellow lines showing the nerve distribution
Injection 1 - Inferior (Starting Point)
Raise a wheal in the subcutaneous space inferior to the auricle at the lobule. This is your starting point.
Injection 2 - Anteroinferior to Anterosuperior
From the inferior wheal, redirect the needle anteriorly and superiorly in the subcutaneous plane (just anterior to the tragus). Inject 2-3 mL while slowly withdrawing the needle. This blocks the auriculotemporal nerve (anterior supply).
Injection 3 - Posteroinferior to Posterosuperior
From the same inferior entry point, redirect the needle posteriorly and superiorly along the posterior sulcus (the groove between the ear and the mastoid). Inject 3-4 mL while slowly withdrawing toward the superior pole. This blocks the great auricular nerve and lesser occipital nerve (posterior supply).
Injection 4 - Superior
From a point superior to the auricle, inject 2-3 mL subcutaneously both anterior and posterior to complete the ring superiorly. Begin each new injection in an area already anesthetized to minimize pain.
Total volume: ~10-12 mL distributed around the ear base.
Simpler 2-Point Technique (Roberts & Hedges)
For faster anesthesia covering most of the auricle:
- Posterior sulcus: Insert needle behind the inferior pole of the auricle, advance superiorly along the crescent-shaped posterior contour - inject 3-4 mL while withdrawing. Blocks great auricular + lesser occipital branches.
- Anterior to tragus: Place 3-4 mL just superior and anterior to the cartilaginous tragus. Blocks the auriculotemporal nerve.
Key Points
-
Always aspirate before injecting to avoid intravascular injection (superficial temporal artery is anterior)
-
Inject in the subcutaneous plane - not intradermally, not deep
-
Wait 3-5 minutes for onset before proceeding with the procedure
-
For the hematoma drainage in your elderly patient: use 1% lidocaine without epinephrine, as the auricle vascularity is already compromised
-
Begin each new injection within the previously anesthetized zone to reduce pain
-
Tintinalli's Emergency Medicine, p. 287
-
Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1526-1527
Do i need to suture the incised wound
Finding Sources
Reading File
The answer from the textbook is clear and nuanced - here's the full picture:
Do You Need to Suture the Incised Wound?
Short answer: Not in the traditional sense - but sutures are used to secure the bolster/dental roll, not to primarily close the skin.
What the Evidence Says
There are two methods of wound management after I&D, and both avoid primary skin closure:
Method 1 - Non-surgical Compression Dressing (simpler, no sutures through skin)
After evacuating and irrigating the hematoma:
- Apply antibiotic ointment to the incision
- The wound edges are not sutured closed
- Fill all auricular crevices with Vaseline gauze
- Apply a multi-layer compression bandage over the entire ear secured with Kerlix
The pressure dressing reapproximates the perichondrium to cartilage mechanically. No skin sutures needed.
Method 2 - Surgical Dental Roll Bolster (sutures used as compression, not wound closure)
This is the preferred method for reliable compression. The sutures here serve a completely different purpose - they hold the dental rolls in place, not close the wound:
- Apply antibiotic ointment to the incision
- Pass a 4-0 nylon suture through-and-through the full thickness of the ear over the hematoma site
- Wrap the suture around a dental roll on the posterior surface, then pass the needle back through the pinna
- Wrap and tie around a second dental roll on the anterior surface - this creates firm compression of the drained cavity
- A second suture may secure a third dental roll
- The dressing must firmly reapproximate perichondrium to cartilage without compromising vasculature
- Remove in 1 week
The incision itself is left to heal by secondary intention under the antibiotic ointment.
Why Not Close the Incision Primarily?
| Reason | Explanation |
|---|---|
| Allows drainage | Any residual blood/seroma can still egress through the open wound |
| Infection risk | Closed dead space over cartilage risks perichondritis if infected |
| Secondary intention heals well | The small incision along natural skin folds heals with minimal scarring |
| Pressure does the work | Reapproximation is mechanical, not suture-dependent |
Post-procedure
- Antistaphylococcal antibiotics (e.g., cefalexin) - mandatory
- Inspect wound at 24 hours for reaccumulation
- Watch for signs of vascular compromise or infection (erythema, warmth, fever)
- If infection develops: remove dressing, surgical drainage, and IV antibiotics
- Remove dental roll bolster at 1 week
Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1536-1537
Bottom line for your 80-year-old patient: Use the dental roll bolster technique with through-and-through 4-0 nylon sutures for reliable compression. The skin incision itself is left open under antibiotic ointment. Given his age and the 2-day-old hematoma, the bolster method is more reliable than a simple dressing alone.
This is a shared conversation. Sign in to Orris to start your own chat.