Short note on berlins edema
Reading File
Finding Sources
Searching the Web
Berlin's edema commotio retinae clinical features pathology treatment
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive short note on Berlin's edema, drawn from authoritative ophthalmology textbooks:
Berlin's Edema (Commotio Retinae)
Definition
Berlin's edema is the term specifically used when commotio retinae involves the posterior pole/macula. Commotio retinae (first described by Berlin in 1873) refers to traumatic retinal opacification following blunt or concussive injury to the globe. The name "edema" is a misnomer - the whitening is not due to extracellular fluid accumulation but rather structural disruption.
Fundus photograph showing commotio retinae with macular (Berlin's) edema:
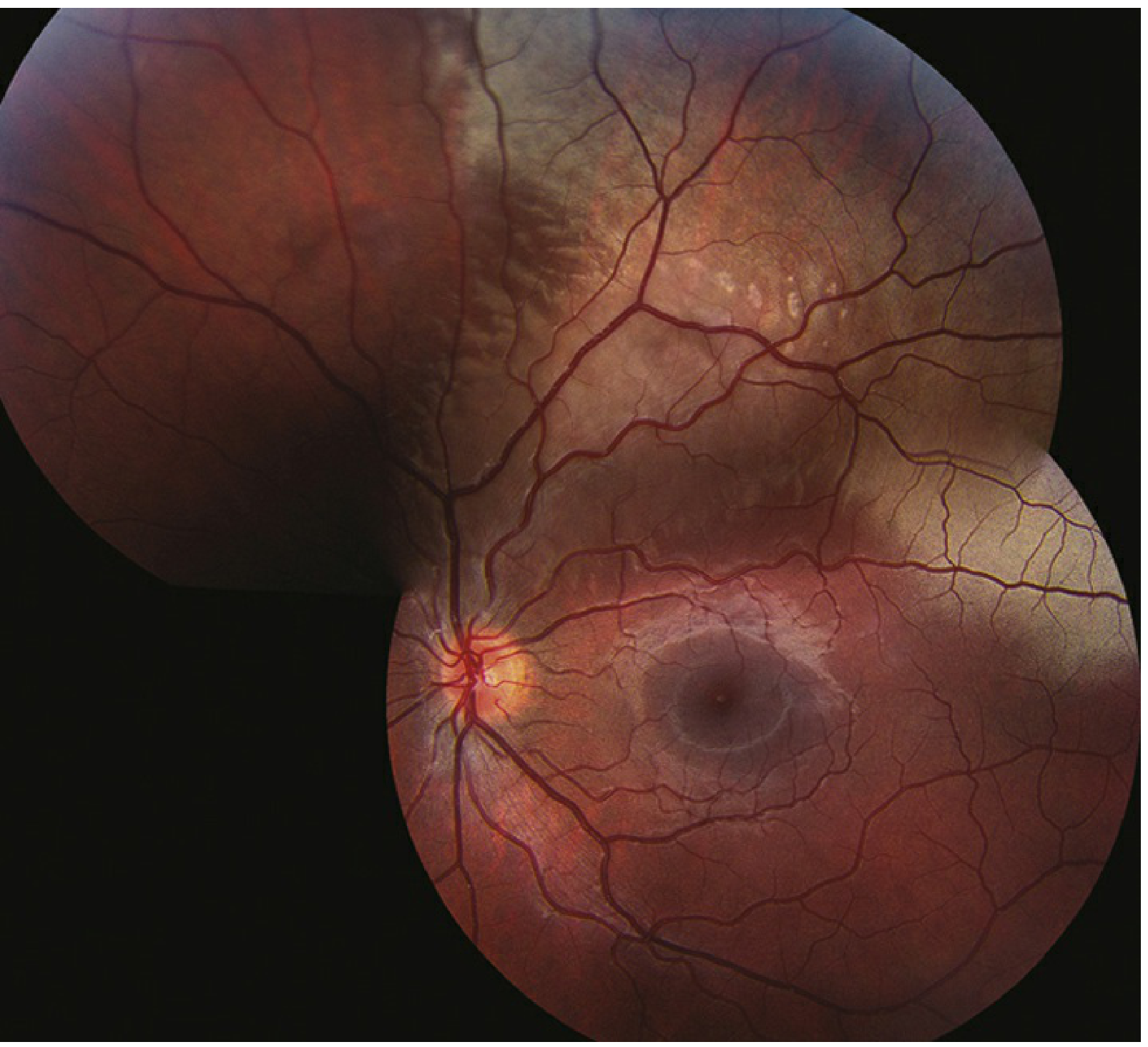
Commotio retinae (Berlin's edema) - note the confluent grey-white retinal whitening around the posterior pole with undisturbed retinal blood vessels. (Wills Eye Manual)
Etiology / Pathophysiology
- Caused by blunt trauma to the globe (direct or transmitted shock waves via contrecoup mechanism)
- Shock waves disrupt the photoreceptor outer segments, causing their fragmentation
- Also causes intracellular edema of the RPE (retinal pigment epithelium)
- The inner retinal layers may also be involved if the force is significant
- The whitening is due to intracellular disruption, NOT extracellular edema (hence the misnomer)
- Present in approximately 30% of all eye traumas presenting for hospital treatment
Symptoms
- Decreased or blurred vision (if macula involved)
- May be asymptomatic if only peripheral retina is affected
- History of recent ocular trauma is always present
- Note: Visual acuity does NOT always correlate with the degree of retinal whitening
Signs (Fundoscopy)
| Feature | Description |
|---|---|
| Retinal whitening | Confluent grey-white/cloudy opacification of involved area |
| Location | Most commonly temporal fundus; posterior pole in Berlin's edema |
| Blood vessels | Retinal vessels are undisturbed in the area of whitening |
| Cherry-red spot | May appear at the fovea (pseudo cherry-red spot) when Berlin's edema involves the macula - the fovea appears red because it lacks inner retinal layers |
| Hemorrhages | Intraretinal hemorrhages may be present with severe involvement |
OCT Findings
- Ellipsoid zone (IS/OS) disruption - the hallmark finding on spectral-domain OCT
- Hyperreflectivity of the outer retinal layers
- Confirms the level of photoreceptor damage and helps grade severity
Differential Diagnosis
- Retinal artery occlusion - whitening follows arterial distribution; no trauma history
- Retinal detachment - retina is elevated; associated retinal break or dialysis
- White without pressure - benign peripheral finding, bilateral, no trauma
- Chorioretinitis slopetaria - caused by high-velocity projectile, bare sclera visible
- Cherry-red spot DDx - Tay-Sachs, Niemann-Pick (present early in life, bilateral, metabolic)
- Myelinated nerve fiber layer - develops postnatally, feathered edges
Workup
- Complete ophthalmic evaluation
- Dilated fundus examination - essential
- Scleral depression (avoid if ruptured globe, hyphema, microhyphema, or iritis is present)
- OCT - ellipsoid zone disruption confirms diagnosis and grades severity
Treatment
- No specific treatment is required; the condition is self-limited
- Observation
- Some centers use oral/topical corticosteroids or anti-inflammatory agents (not evidence-based standard of care)
Prognosis & Follow-up
- Mild cases: Good prognosis; spontaneous resolution in approximately 4-6 weeks with restoration of normal fundal appearance
- Severe/macular cases: May result in:
- Chronic visual impairment
- RPE atrophy or hyperpigmentation
- Progressive pigmentary degeneration
- Macular hole formation (either at time of injury or after resolution)
- Follow-up: Dilated fundus exam repeated in 1-2 weeks; patient instructed to return immediately if retinal detachment symptoms develop (flashes, floaters, field loss)
Key Points to Remember
- Berlin's edema = commotio retinae of the posterior pole/macula
- Mechanism: photoreceptor outer segment fragmentation + RPE intracellular edema
- It is NOT true edema - the name is a misnomer
- Key sign: retinal whitening with undisturbed blood vessels
- Pseudo cherry-red spot at fovea distinguishes it from central retinal artery occlusion (history of trauma is key)
- OCT shows ellipsoid zone disruption
- Self-limiting, no treatment needed; but macular involvement can leave permanent visual deficit
Sources: Kanski's Clinical Ophthalmology 10th ed., p.933 | Wills Eye Manual, pp.149-151 | EyeWiki - Commotio Retinae
Blood retinal barrier
Finding Sources
Searching the Web
blood retinal barrier inner outer components tight junctions clinical significance breakdown
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a detailed short note on the Blood-Retinal Barrier (BRB):
Blood-Retinal Barrier (BRB)
Definition
The blood-retinal barrier is a specialized selective permeability system that separates the neural retina from the systemic circulation, maintaining the unique microenvironment required for optimal retinal cell function. It is analogous to the blood-brain barrier and is part of the broader blood-ocular barrier.
Components
The BRB has two distinct anatomical and functional barriers:
1. Inner BRB (iBRB)
Formed by the tight junctions (zonula occludentes) between non-fenestrated retinal capillary endothelial cells.
Structural components of retinal capillaries:
- Endothelial cells - form a single layer on the basement membrane; linked by tight junctions; no fenestrations (unlike choriocapillaris)
- Basement membrane - lies beneath endothelial cells; plays only a minor role in barrier function
- Pericytes - lie external to endothelial cells; have contractile pseudopodal processes that envelop the capillaries; participate in autoregulation of microvascular circulation; play only a minor role in barrier function
The inner BRB prevents passage of both bound and free fluorescein (and other macromolecules) across the vessel wall into the retinal extravascular space.
Retinal capillary supply: supply the inner two-thirds of the retina; the outer third is supplied by the choriocapillaris.
Diagram - Inner BRB (intact vs disrupted):
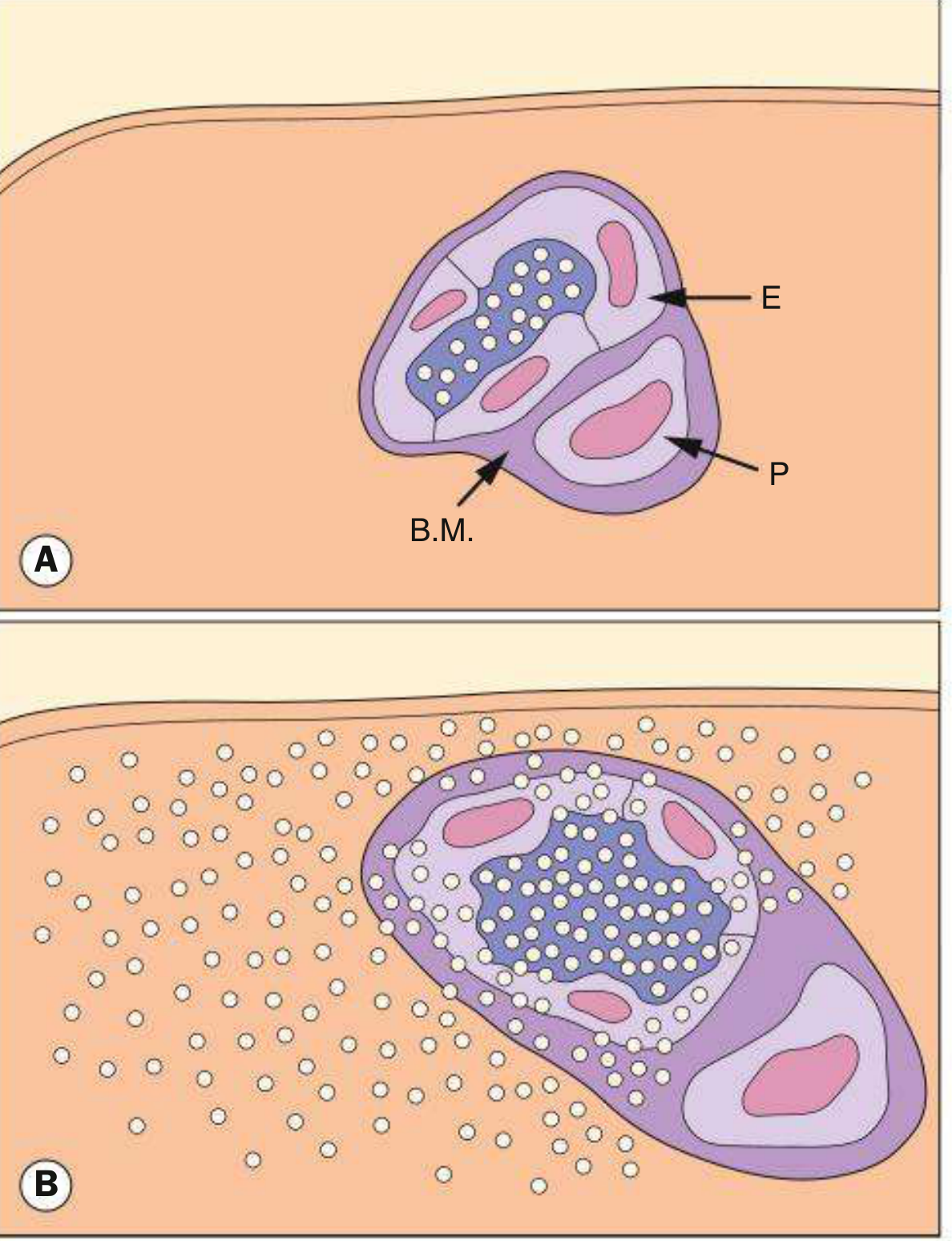
Fig. 14.5 Inner blood-retinal barrier. (A) Intact - E = endothelial cell, P = pericyte, B.M. = basement membrane. (B) Disrupted - fluorescein leaks freely into retinal tissue. (Kanski's Clinical Ophthalmology)
2. Outer BRB (oBRB)
Formed by the tight junctions (zonula occludentes) between RPE (retinal pigment epithelium) cells, located at the level of Bruch's membrane.
How it works:
- The choriocapillaris is fenestrated - unbound fluorescein and small molecules escape into extravascular space freely
- These molecules cross Bruch's membrane but are blocked at the RPE tight junctions
- The RPE also actively pumps ions and water out of the subretinal space (inward transport of nutrients, outward transport of metabolic waste)
Diagram - Outer BRB:
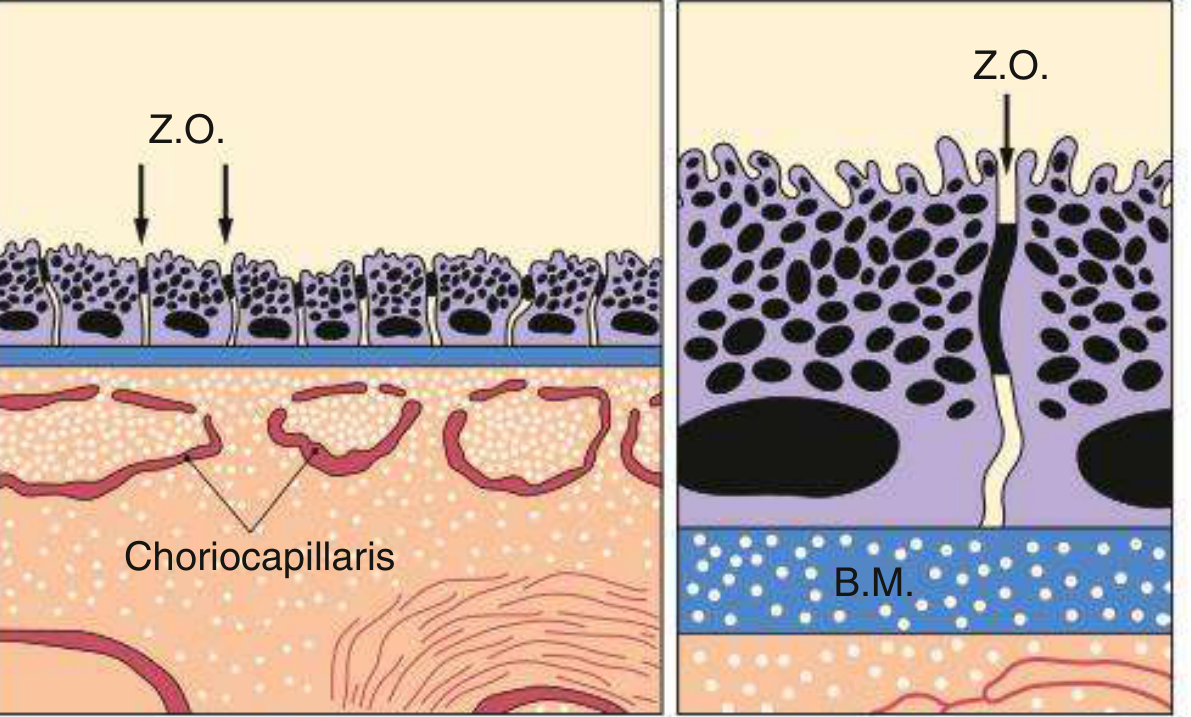
Fig. 14.4 Outer blood-retinal barrier showing RPE cells with tight junctions (Z.O. = zonula occludentes) blocking leakage from the fenestrated choriocapillaris through Bruch's membrane (B.M.). (Kanski's Clinical Ophthalmology)
Summary Table
| Feature | Inner BRB | Outer BRB |
|---|---|---|
| Formed by | Retinal capillary endothelial cell tight junctions | RPE cell tight junctions |
| Location | Within retinal capillaries | Between RPE and subretinal space |
| Barrier type | Non-fenestrated endothelium | Fenestrated choriocapillaris blocked by RPE |
| Blood supply | Retinal circulation | Choroidal circulation (choriocapillaris) |
| Layer supplied | Inner 2/3 of retina | Outer 1/3 of retina (photoreceptors) |
| Additional support | Pericytes, basement membrane (minor role) | Bruch's membrane |
Additional Functions of Outer BRB (RPE)
- Phagocytosis of shed photoreceptor outer segments (daily turnover)
- Storage, metabolism and transport of vitamin A in the visual cycle
- Inward transport of metabolites (amino acids, glucose) to photoreceptors
- Outward transport of metabolic waste products
- Dense melanin pigment absorbs stray light and reduces optical scatter
Breakdown of BRB - Clinical Significance
Inner BRB Breakdown
Causes leakage on FFA - hyperfluorescence that increases in both size and intensity over time:
| Mechanism | Examples |
|---|---|
| Dysfunction/loss of existing tight junctions | Diabetic retinopathy (background DR), retinal vein occlusion (RVO), cystoid macular oedema (CME), disc swelling |
| Primary absence of tight junctions (new vessels) | Macular neovascularization (MNV), proliferative diabetic retinopathy, Coats disease, tumours |
Outer BRB Breakdown
Causes pooling of fluorescein in an anatomical space on FFA:
| Site of pooling | Example |
|---|---|
| Subretinal space | Central serous chorioretinopathy (CSCR) - slow, well-defined pooling |
| Sub-RPE space | Pigment epithelial detachment (PED) - hyperfluorescence increases in intensity but NOT in size |
Key Points
- The BRB maintains the immune-privileged status of the retina
- The inner BRB is more analogous to the blood-brain barrier (non-fenestrated endothelium)
- The outer BRB relies on RPE tight junctions to compensate for the fenestrated choriocapillaris
- FFA (fluorescein angiography) is the classical method to assess BRB integrity - leakage or pooling indicates breakdown
- Diabetes is the most common systemic cause of inner BRB breakdown (leading to diabetic macular oedema)
- CSCR is the classic example of outer BRB breakdown (RPE tight junction dysfunction)
Sources: Kanski's Clinical Ophthalmology 10th ed., pp. 581-584, 933 | PMC - Tight Junctions of the Outer Blood Retina Barrier
Teleophthalmology - role and application short note
Finding Sources
Searching the Web
teleophthalmology role applications diabetic retinopathy screening ROP glaucoma 2024
Finding Sources
Searching PubMed
teleophthalmology applications screening
Searching the Web
teleophthalmology definition types store-and-forward synchronous applications advantages limitations India
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10699065
Reading Article
PMID: 38053188
Reading Web Page
https://ascrs.org/-/media/ascrs-website/government-relations…
Searching the Web
teleophthalmology ROP screening AI artificial intelligence glaucoma AMD applications 2023 2024
Here is a comprehensive short note on Teleophthalmology, synthesized from authoritative sources:
Teleophthalmology - Role and Applications
Definition
Teleophthalmology is the practice of ophthalmology using electronic communication technology to exchange medical information remotely - for screening, diagnosis, chronic disease management, and remote monitoring of patients who are geographically separated from the clinician. It is a subspecialty application of telemedicine within eye care.
It has gained particular momentum since the COVID-19 pandemic, which acted as a catalyst for widespread adoption, and is now further transformed by Artificial Intelligence (AI) integration.
Types / Delivery Methods
| Type | Description | Example |
|---|---|---|
| Asynchronous ("Store-and-Forward") | Clinical data (images, reports) captured and stored, then transmitted to a specialist at a different time and location for review | Retinal photos taken by a nurse in a diabetes clinic; ophthalmologist reviews them remotely and sends a report |
| Synchronous (Real-Time) | Live, two-way audio-video interaction between patient and clinician simultaneously | Live video consultation for urgent eye complaints or post-operative review |
| Hybrid | Combination of both - real-time interaction supplemented by pre-captured data/images | Remote clinic where technician takes images while specialist reviews them live on a video call |
| AI-Enabled | Automated algorithmic interpretation of images/data - no real-time specialist needed | FDA-approved AI system (IDx-DR) reads fundus photographs autonomously for diabetic retinopathy |
Asynchronous (store-and-forward) is currently the dominant and most scalable model, particularly for population-level screening programs, as it does not require simultaneous presence of doctor and patient.
Applications
1. Diabetic Retinopathy (DR) Screening
The largest and most established application of teleophthalmology.
- Non-mydriatic fundus cameras or smartphone-based funduscopy at primary care/diabetes clinics
- Images transmitted to ophthalmologists or AI engines for grading
- Identifies patients needing urgent referral vs. routine follow-up
- Shown to increase screening rates, reduce false-positive referrals, and improve follow-up compliance
- AI tools (e.g., IDx-DR, EyeArt) can autonomously detect referable DR with high sensitivity
2. Retinopathy of Prematurity (ROP) Screening
- ROP screening traditionally required an ophthalmologist to physically examine premature neonates in the NICU
- Wide-field retinal cameras (e.g., RetCam) capture images of the infant retina
- Images transmitted to a remote ROP specialist for grading
- Particularly valuable in LMICs (low- and middle-income countries) such as India where ROP specialists are scarce
- AI-based screening for ROP is now validated and expanding in these settings
3. Glaucoma Monitoring
- Remote optic disc imaging, OCT of the optic nerve, and visual field testing results transmitted for specialist review
- Allows monitoring of stable glaucoma patients between clinic visits
- Reduces unnecessary referrals from primary/optometric care
4. Age-Related Macular Degeneration (AMD)
- OCT images and fundus photos transmitted for remote assessment
- Monitoring of treated AMD patients (anti-VEGF) between injections
- Aids in timely detection of disease progression or new CNV
5. Refractive Error Assessment & School Screening
- Automated refraction devices used in community/school settings
- Data transmitted remotely for prescription generation
- Cost-effective method for mass screening of children
6. Emergency Ophthalmology / Triage
- Anterior segment photography, slit-lamp photography for triage of acute red eye, trauma
- Helps emergency physicians get rapid ophthalmology input without immediate on-call attendance
- Identification of conditions requiring urgent transfer vs. conservative management
7. Post-Operative Monitoring
- Remote monitoring of cataract and retinal surgery patients
- Slit-lamp photographs and visual acuity assessments transmitted to surgeon
- Reduces unnecessary follow-up visits for uncomplicated cases
8. Diabetic Macular Edema (DME) and Retinal Vein Occlusion
- OCT-based remote monitoring for macular edema activity
- Helps determine anti-VEGF injection timing without every visit requiring specialist presence
9. Pediatric Ophthalmology
- Remote vision screening and amblyopia detection
- Photoscreening devices used by non-ophthalmologists; images reviewed remotely
Role in Healthcare Systems
| Context | Role |
|---|---|
| Rural/underserved areas | Extends specialist reach to remote populations without access to ophthalmologists |
| Primary care integration | GP/diabetes nurses perform imaging; specialists provide remote grading |
| NICU/neonatal care | Remote ROP specialist avoids need for bedside examination in all cases |
| COVID-19 / Pandemic | Maintained continuity of eye care with minimal physical contact |
| Developing countries | Addresses specialist shortfall through hub-and-spoke telemedicine models |
| Education & training | Remote mentoring, case discussion, grand rounds |
| Research | Remote data collection, multi-center studies, epidemiological surveys |
AI in Teleophthalmology
AI has transformed teleophthalmology from a purely "image transfer" model to one with autonomous diagnostic capability:
- DR screening: FDA-approved AI (IDx-DR) autonomously reads fundus photos - first AI diagnostic device approved without specialist oversight
- ROP: AI grading of retinal images in NICUs, validated in India for LMICs
- Glaucoma: AI analysis of optic disc photos and OCT data
- AMD: Deep learning models for CNV detection on OCT
- Keratoconus: Automated corneal topography analysis available for decades
- Scheduling/billing: AI-assisted front-office tasks to improve clinic efficiency
- Home monitoring: AI watchdog algorithms that flag deteriorating home-monitoring data for physician review
Advantages
- Increased access to specialist care for rural, remote, and underserved populations
- Cost-effectiveness - reduces travel costs for patients, reduces unnecessary referrals
- Scalability - population-level screening programs feasible
- Reduced patient burden - fewer clinic visits, convenience
- Timely triage - emergency cases identified and prioritized efficiently
- Addresses specialist shortage - one specialist can review images from multiple remote sites
- Improved follow-up compliance compared to in-person model for chronic disease
Limitations
| Category | Limitation |
|---|---|
| Image quality | Poor-quality images (3-22% of cases) are a major cause of false referrals; require better equipment and trained technicians |
| Technology access | Lack of infrastructure, internet connectivity in remote areas |
| Digital literacy | Patients and staff may lack confidence with technology |
| Data security | HIPAA compliance, patient privacy and cloud data security concerns |
| Incomplete examination | Certain assessments (IOP measurement, slit-lamp examination, anterior segment, gonioscopy) require physical presence |
| Legal/liability | Medicolegal framework for remote diagnosis still evolving |
| Reimbursement | Insurance reimbursement policies for telemedicine vary by country/region |
| Human element | Reduced personal patient-physician interaction |
| Equipment cost | Initial setup of imaging devices at peripheral sites can be expensive |
Key Points to Remember
- Three delivery modes: Store-and-forward (asynchronous), Real-time (synchronous), Hybrid
- Diabetic retinopathy screening is the most established and widely deployed application
- ROP telemedicine is life-changing in LMICs where neonatology-trained specialists are few
- AI integration enables fully autonomous screening - IDx-DR is the first FDA-approved autonomous AI diagnostic system
- Teleophthalmology addresses the global maldistribution of ophthalmologists
- Limitations center around image quality, technology access, data security, and incomplete physical examination
- Post-COVID, teleophthalmology has entered mainstream practice and is now an integral part of modern eye care delivery
Sources: ASCRS Introduction to Tele-Ophthalmology | Than et al., Int J Retina Vitreous 2023 (PMID: 38053188) - Teleophthalmology and retina review | MDPI J Clin Med 2023 - Efficacy in underserved populations
This is a shared conversation. Sign in to Orris to start your own chat.