CASE 1: A 65-yo male was a diagnosed of case of chronic gouty arthritis. He was advised to take Ibuprofen as a remedy if ever he experiences an attack. Because of financial constraints, he was unable to follow up with his rheumatologist regarding his gout and will usually double or triple the dose of Ibuprofen if the pain becomes severe or difficult to handle. Recently, the patient encountered recurrent gouty flares and has been taking his medication almost daily with double or triple the dose. The patient was eating his dinner with his family when he suddenly experienced epigastric discomfort. He initially tolerated it and drank 2 glasses of water to relieve the pain. The pain was described to be stabbing and steady in character. Around 2 hours after, the patient noted an increase in the severity of pain, noted to be pale and diaphoretic and was screaming in pain. He was brought to a DMSF Hospital where you are the clinical clerk on duty. 1. Extract additional information regarding patient’s history. 2. Perform the necessary assessment needed to diagnose the disease. 3. Give your initial impression on the case. 4. Correlate the symptoms with the patient’s risk factors to develop the disease considered. 5. Provide the necessary diagnostic modalities necessary to confirm or reject your initial impression. 6. Enumerate your plans for the patient.from shwarts
Clinical Case Analysis: Perforated Peptic Ulcer
1. Additional History to Extract
- Onset: Exact time of the initial epigastric pain and the time it became severe
- Location: Epigastric initially - has it spread? Radiation to the shoulder (referred diaphragmatic irritation)?
- Duration and progression: Was there a sudden explosive onset (perforation "lightning bolt") vs. gradual worsening?
- Character: Patient described stabbing and steady - any worsening with movement or breathing?
- Alleviating/aggravating factors: Does leaning forward relieve anything? Does breathing worsen it?
- Associated symptoms: Nausea, vomiting, fever, chills, black or bloody stools (melena/hematochezia), dysphagia, early satiety, weight loss
- How long has the patient been taking Ibuprofen? (chronic daily use strongly implicates NSAID-induced PUD)
- What doses? (He self-escalates to 2-3x the recommended dose)
- Has he taken any gastroprotective agent (misoprostol, PPIs, H2 blockers) alongside the NSAID?
- Use of corticosteroids, anticoagulants, antiplatelet agents (aspirin)
- Prior episodes of epigastric pain, especially post-prandially or nocturnally?
- Prior diagnoses of gastritis, H. pylori infection, or peptic ulcer disease?
- Previous upper GI endoscopy or barium studies?
- History of similar pain in the past that resolved spontaneously (sealed perforations)?
- Smoking status (known risk factor for PUD and impaired healing)
- Alcohol use
- Coffee/tea consumption (acid secretagogues)
- Dietary habits at the time of symptom onset (eating triggers)
- Previous abdominal surgeries
- Comorbidities: diabetes, cardiovascular disease, chronic kidney disease (all affect surgical risk)
- History of H. pylori testing or treatment
- Peptic ulcer disease (genetic predisposition)
- Gastric or GI malignancy
- Functional status (for surgical risk assessment)
- Access to care/financial situation (important for follow-up planning)
- Hematemesis or melena (concurrent GI bleeding)
- Jaundice (to rule out hepatobiliary pathology)
- Urinary symptoms (to rule out renal colic)
- Chest symptoms (to rule out MI, which can mimic upper abdominal pain)
2. Physical Assessment
- Temperature (initially normal in perforation, pyrexia develops hours later as bacterial peritonitis supervenes)
- Blood pressure and pulse (tachycardia and hypotension indicate shock)
- Respiratory rate
- Oxygen saturation
- GCS/mentation
- Patient appears pale and diaphoretic (already noted) - this implies sympathetic activation and early shock
- Position: Is the patient lying still and rigidly? (peritoneal irritation makes patients afraid to move)
- Facial expression: grimacing, writhing (visceral pain) vs. lying very still (peritoneal pain)
- Inspection: Abdominal distension, absence of respiratory movements of the abdomen (a classic sign of peritonitis), visible peristalsis, surgical scars
- Auscultation (before palpation): Absence of bowel sounds (paralytic ileus from peritonitis - "silent abdomen")
- Percussion: Obliteration of liver dullness (pneumoperitoneum - free air under diaphragm), generalized tympany
- Palpation:
- Board-like rigidity - the hallmark of perforated peptic ulcer; the abdomen is tense and hard like a wooden board due to involuntary guarding
- Tenderness - initially epigastric, but generalizes as peritonitis spreads
- Rebound tenderness (positive Blumberg's sign)
- Does the pain radiate to the right iliac fossa? (gastric contents may track down the right paracolic gutter, mimicking appendicitis)
- Tachycardia is typically the first cardiovascular sign
- Hypotension in later/severe shock
- Reduced breath sounds at bases (sympathetic pleural effusion or referred pain guarding)
- Rule out pneumothorax
- Boggy tender mass or pelvic peritoneal irritation if fluid has tracked to the pelvis
3. Initial Impression
Perforated Peptic Ulcer (most likely duodenal) with secondary Generalized Peritonitis
- Middle-aged to elderly male with chronic NSAID overuse
- Sudden onset severe, steady, stabbing epigastric pain
- Progressive deterioration over 2 hours
- Pallor and diaphoresis (signs of shock/sympathetic activation)
- Screaming in pain (extreme peritoneal irritation)
| Condition | Arguments For | Arguments Against |
|---|---|---|
| Perforated peptic ulcer | NSAID use, sudden onset, epigastric, progressive severity, shock | - |
| Acute pancreatitis | Epigastric pain, sudden onset, age | No alcohol or gallstone history mentioned; pain character less consistent |
| Acute MI (inferior/posterior) | Epigastric pain, diaphoresis, pallor, age | No chest radiation, no cardiac history - but must be excluded |
| Acute cholecystitis/perforation | Epigastric/RUQ pain | No fatty food trigger, no fever at onset, different character |
| Mesenteric ischemia | Severe abdominal pain, elderly | Pain disproportionate to findings classically, needs vascular risk factors |
| Aortic dissection/rupture | Sudden severe pain, shock, older male | More tearing, radiation to back, usually pulsatile mass |
4. Symptom-Risk Factor Correlation
| Patient Finding | Risk Factor / Mechanism | Consequence |
|---|---|---|
| Daily Ibuprofen at 2-3x dose | NSAIDs inhibit COX-1 → reduced prostaglandin E2 synthesis → loss of mucosal protection (decreased mucus, bicarbonate, blood flow) | Mucosal barrier breakdown → peptic ulceration |
| Chronic daily NSAID use | Direct topical irritation of gastric mucosa + systemic prostaglandin suppression | Gastric/duodenal ulcer formation; impaired ulcer healing |
| No gastroprotective co-therapy | Absence of PPI or misoprostol | No buffering of NSAID-induced mucosal damage |
| Advanced age (65 years) | Reduced mucosal prostaglandin reserve, decreased tissue repair capacity | Higher risk of ulceration and perforation; atypical presentations possible |
| Male sex | Males have higher gastric acid output than females | Greater acid-peptic injury |
| No H. pylori testing/treatment | H. pylori + NSAID use = synergistic ulcer risk | Greater than 90% of serious PUD complications attributable to H. pylori, NSAIDs, and/or smoking (Schwartz's Surgery, 11th Ed.) |
| Financial constraints/no follow-up | Unmonitored disease progression, self-medication escalation | Peptic ulcer disease left untreated until catastrophic complication |
| Sudden onset pain during eating | Eating stimulates acid secretion; a pre-existing ulcer already at the perforation point | Final stress event leading to frank perforation |
| 2-hour progressive worsening | Initial perforation of sterile gastric contents → peritoneal chemical irritation → then bacterial contamination spreads | Classical biphasic course of perforated peptic ulcer |
| Pallor and diaphoresis | Sympathetic nervous system activation, early hypovolemic/septic shock | SIRS/sepsis from peritoneal contamination |
5. Diagnostic Modalities
Bedside / Immediate
- Complete vital signs (BP, HR, RR, SpO2, temperature)
- IV access + blood draw (simultaneous with history and examination)
- ECG - to rule out inferior MI (mandatory in a 65-year-old male with epigastric pain and diaphoresis)
Laboratory Tests
| Test | Purpose |
|---|---|
| CBC with differential | Leukocytosis (peritonitis), anemia (concurrent bleeding), thrombocytopenia |
| Serum amylase and lipase | To exclude acute pancreatitis (may be mildly elevated in perforation, but not to levels seen in pancreatitis) |
| BMP/Electrolytes + Creatinine | Baseline renal function, electrolyte disturbances |
| LFTs + bilirubin | Exclude hepatobiliary etiology |
| PT/INR, aPTT | Coagulation status pre-operatively |
| Serum lactate | Assess severity of shock and tissue hypoperfusion |
| Blood type and crossmatch | Pre-operative preparation |
| ABG | Acid-base status; metabolic acidosis indicates severity of shock |
| Troponin | To rule out ACS given the presentation |
| Urinalysis | Exclude renal/urological cause |
| H. pylori testing | Urea breath test or stool antigen (or intraoperative biopsy); guides post-operative management |
| Blood cultures | If febrile or sepsis suspected |
| Serum glucose | Baseline (diabetic patient perioperative risk) |
Imaging
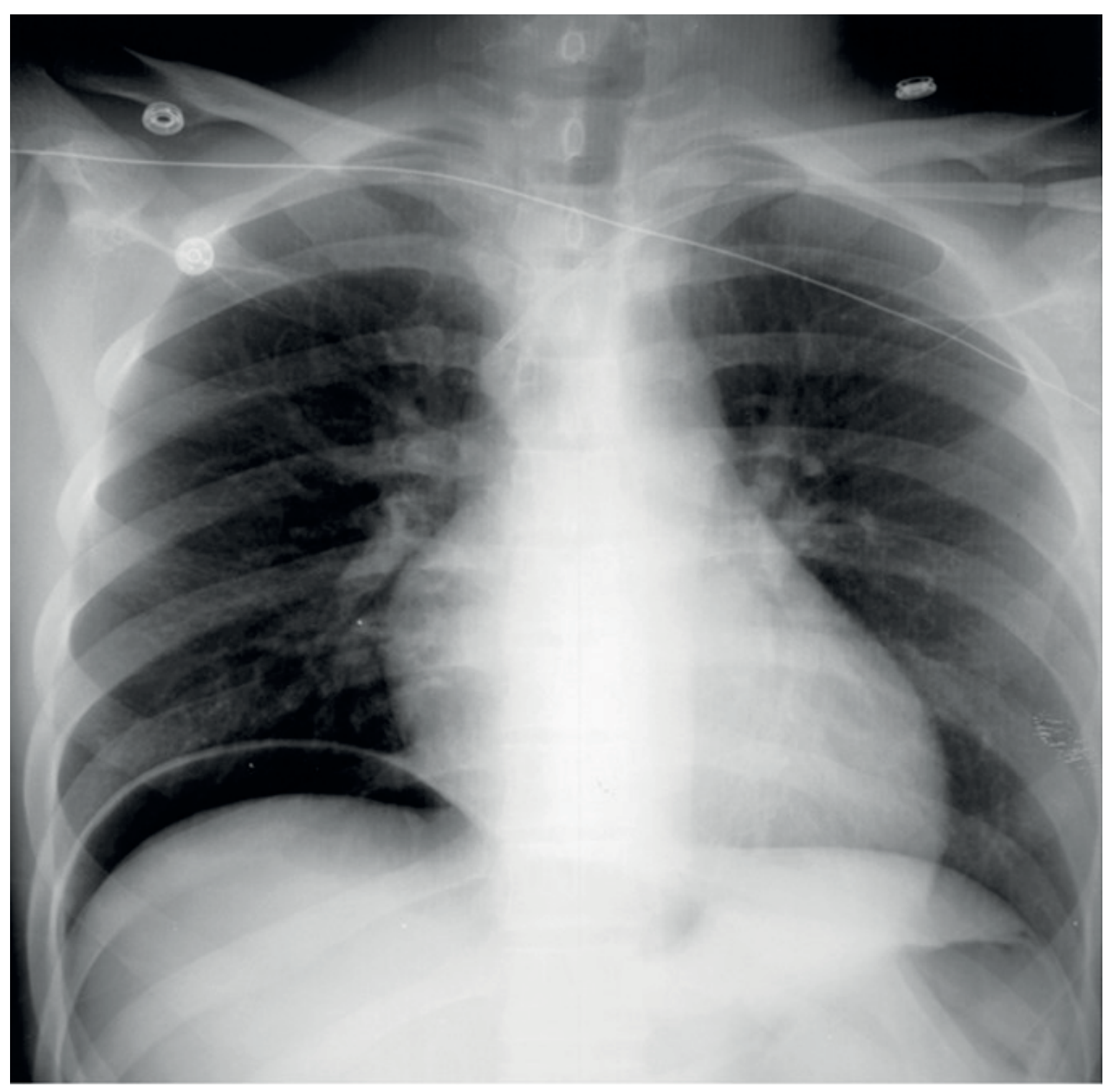
- The first imaging investigation of choice
- Reveals free gas (pneumoperitoneum) under the diaphragm in >50% of perforated peptic ulcer cases
- A negative CXR does not exclude perforation
- Now the most commonly used and most accurate modality
- Confirms pneumoperitoneum, identifies the site of perforation, shows extent of peritoneal contamination, rules out other diagnoses
- Can identify sealed perforations and guide non-operative management
- May also show free air, though less sensitive than CXR
- Can detect free peritoneal fluid
- NOT performed acutely in suspected perforation (risk of worsening leak with insufflation)
- Reserved for stable patients after perforation has been excluded or post-operatively for H. pylori
6. Management Plans
A. Immediate Resuscitation ("ABCDE")
- Airway: Ensure patent; prepare for intubation if GCS deteriorates
- Breathing: Supplemental oxygen via face mask (maintain SpO2 >95%)
- Circulation:
- Two large-bore IV cannulae
- Aggressive IV crystalloid resuscitation (Normal Saline or Lactated Ringer's)
- Correct electrolyte imbalances
- Vasopressors if refractory shock (after adequate volume resuscitation)
- Disability: GCS, pain assessment
- Exposure: Full abdominal examination; insert urinary catheter (monitor urine output hourly; target >0.5 mL/kg/hr)
B. Analgesia
- Do NOT withhold analgesia out of fear of masking signs. Bailey and Love's explicitly states: "Analgesia should not be withheld for fear of removing the signs of an intra-abdominal catastrophe. In fact, adequate analgesia makes the clinical signs more obvious."
- IV opioid analgesia (morphine or fentanyl) titrated to effect
- Antiemetics (ondansetron or metoclopramide)
C. Nasogastric Tube (NGT)
- Insert to decompress the stomach and prevent further leakage of gastric contents into the peritoneal cavity
- Reduces vomiting and aspiration risk
D. Nothing by Mouth (NPO)
- Strict NPO status in preparation for surgery and to reduce GI secretions
E. Antibiotics
- Broad-spectrum IV antibiotics covering Gram-negative enteric organisms and anaerobes
- e.g., Cefuroxime + Metronidazole, or Piperacillin-Tazobactam
- Start as early as possible (sepsis bundle: within 1 hour of sepsis recognition)
F. Acid Suppression
- IV Proton Pump Inhibitor (e.g., IV Pantoprazole or Omeprazole) - reduces gastric acid secretion, aids ulcer healing post-operatively
G. Surgical Intervention (Definitive Treatment)
- Confirm the diagnosis and find the perforation
- Thorough peritoneal toilet (wash out all gastric contents, pus, and food debris)
- Close the perforation
| Situation | Preferred Procedure |
|---|---|
| Most common approach | Simple patch closure (Graham patch / omental patch) - suture closure of perforation reinforced with a pedicled omental patch, followed by post-op H. pylori eradication + PPI |
| Stable low-risk patient with chronic DU and H. pylori+ | Patch closure + Highly Selective Vagotomy (HSV) |
| Stable patient with DU + failed H. pylori therapy | Patch closure + Vagotomy + Drainage (V+D) |
| Gastric ulcer | Biopsy + patch, or wedge excision + closure (to exclude malignancy) |
| Massive perforation not amenable to primary closure | Distal gastrectomy + Roux-en-Y reconstruction |
H. Post-Operative Care
- ICU/HDU monitoring
- Continue IV antibiotics until clinical improvement, then step down to oral
- IV PPI converted to oral PPI (minimum 4-8 weeks)
- H. pylori testing and eradication therapy if positive (amoxicillin + clarithromycin + PPI for 14 days, or bismuth quadruple therapy) - this is essential to prevent recurrence
- Permanent discontinuation of NSAIDs - educate patient about NSAID risks
- If NSAIDs are unavoidable in the future (for gout): switch to a selective COX-2 inhibitor + add a PPI
- Nutritional support
- DVT prophylaxis
- Wound care
- Repeat endoscopy at 6-8 weeks (especially for gastric ulcers) to confirm healing and re-biopsy
I. Gout Management Revision
- Refer to rheumatology post-recovery
- Switch pain management for gouty flares: Colchicine (first-line) or corticosteroids (if colchicine contraindicated) - NOT NSAIDs
- Consider urate-lowering therapy (allopurinol, febuxostat) for chronic gout prevention
- This eliminates the need for recurrent NSAID use that caused this complication
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 67 - Complications of peptic ulceration, Perforated peptic ulcer
- Schwartz's Principles of Surgery, 11th Edition, Chapter 26 - Stomach and Duodenum: Pathophysiology, Etiology, and Perforated Peptic Ulcer
- Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7th Edition, Chapter 45 - Perforation and Surgical Treatment
- Robbins & Kumar Basic Pathology - Peptic Ulcer Disease pathogenesis
Give ans 2 specific for my patient directly from Schwartz
Answer 2: Physical Assessment - Directly from Schwartz, Applied to This Patient
What Schwartz Says About Clinical Manifestations of PUD
"More than 90% of patients with PUD complain of abdominal pain. The pain is typically nonradiating, burning in quality, and located in the epigastrium... A history of PUD, use of NSAIDs, over-the-counter antacids, or antisecretory drugs is suggestive of the diagnosis. Other signs and symptoms include nausea, bloating, weight loss, stool positive for occult blood, and anemia."
- Schwartz's Principles of Surgery, 11th Ed., §Clinical Manifestations
What Schwartz Says About NSAID Risk Specifically
"Chronic use of NSAIDs (including aspirin) increases the risk of peptic ulcer disease about fivefold and upper GI bleeding at least twofold. Complications of PUD (specifically hemorrhage and perforation) are much more common in patients taking NSAIDs. More than half of patients who present with peptic ulcer hemorrhage or perforation report the recent use of NSAIDs, including aspirin. Many of these patients remain asymptomatic until they develop these life-threatening complications."
- Schwartz's, §Nonsteroidal Anti-Inflammatory Drugs in Peptic Ulcer Disease
What Schwartz Says About Factors Increasing NSAID-Complication Risk
"Factors that clearly put patients at increased risk for NSAID-induced GI complications include age >60, prior GI event, high NSAID dose, concurrent steroid intake, and concurrent anticoagulant intake. ANY patient taking NSAIDs or aspirin who has one or more of these risk factors should receive concomitant acid-suppressive medication, preferably PPI."
- Schwartz's, §Nonsteroidal Anti-Inflammatory Drugs in Peptic Ulcer Disease
- Age 65 (>60) ✓
- High NSAID dose (self-escalating to 2-3x the prescribed dose) ✓
- Received NO PPI cover ✗ - the failure that enabled this perforation
What Schwartz Says About Perforated Peptic Ulcer Specifically
"Perforation is the second most common complication of peptic ulcer, but nowadays it is a much more common indication for operation than bleeding. NSAID and/or aspirin use have been inextricably linked with perforated PUD, especially in the elderly population. Surgery is almost always indicated for ulcer perforation, although occasionally nonsurgical treatment can be used in the stable patient without peritonitis in whom radiologic studies document a sealed perforation."
- Schwartz's, §Perforated Peptic Ulcer (Fig. 26-44)
Physical Assessment Findings to Expect in This Patient (Per Schwartz Framework)
| Examination Component | Expected Finding in This Patient | Schwartz Basis |
|---|---|---|
| General appearance | Pale, diaphoretic, writhing then lying very still | Signs of sympathetic activation from peritoneal contamination |
| Vital signs | Tachycardia, hypotension developing, tachypnea, low-grade or no fever initially | Perforation of sterile gastric contents initially; fever develops as bacterial peritonitis supervenes |
| Abdomen - inspection | Not moving with respiration; no visible peristalsis | Peritoneal irritation causing voluntary splinting |
| Abdomen - auscultation | Absent or markedly diminished bowel sounds | Paralytic ileus from peritonitis |
| Abdomen - percussion | Loss of liver dullness (pneumoperitoneum); generalized tympany | Free intraperitoneal gas |
| Abdomen - palpation | Board-like rigidity, generalized tenderness, rebound tenderness greatest in epigastrium | Involuntary guarding from peritoneal contamination with gastric acid |
| Rectal exam | Tenderness anteriorly (pelvic peritoneum) | If gastric contents have tracked to pelvis |
"Surgery is almost always indicated for ulcer perforation." - Schwartz's
Ok perfect now give ans that i can put in my ppt presentation
PHYSICAL ASSESSMENT
65 y/o Male | Chronic NSAID Use | Acute Abdomen
VITAL SIGNS
- BP: Hypotension (developing) - sign of early shock
- HR: Tachycardia - first cardiovascular sign of peritonitis
- RR: Tachypnea - pain-driven, peritoneal splinting
- Temp: Afebrile initially - pyrexia develops hours later as bacterial peritonitis supervenes
- SpO2: May be reduced - pain-limited breathing
GENERAL SURVEY
- Pale and diaphoretic (already noted on presentation)
- Lying very still - movement worsens peritoneal pain
- Screaming / extreme distress
- Abdomen does NOT move with respiration
ABDOMINAL EXAMINATION
- Abdominal rigidity visible
- No respiratory movement of abdomen
- Absent or markedly diminished bowel sounds - paralytic ileus
- Loss of liver dullness - free gas (pneumoperitoneum)
- Generalized tympany
- Board-like rigidity - hallmark finding
- Epigastric tenderness maximal, generalizing to entire abdomen
- Positive rebound tenderness (Blumberg's sign)
- Guarding - involuntary
- Anterior tenderness - pelvic peritoneal irritation if fluid has tracked inferiorly
ECG
- Must be done in a 65-year-old male presenting with epigastric pain + diaphoresis
- Rule out inferior/posterior MI before attributing pain to abdomen
Schwartz, 11th Ed.: "NSAID and/or aspirin use have been inextricably linked with perforated PUD, especially in the elderly population. Surgery is almost always indicated for ulcer perforation."
"Many of these patients remain asymptomatic until they develop these life-threatening complications."
- Age >60 ✓
- High/supratherapeutic NSAID dose ✓
- No concomitant PPI ✓ (the preventable failure)