ECG
Reading File
Asking for Preferences
Finding Sources
Searching the Web
10 classic disease ECG patterns cardiology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have a comprehensive set of information and images. Let me compose the full answer covering 10 classic disease ECG patterns:
ECG Patterns in 10 Classic Diseases
Sources: Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine; Goldberger's Clinical Electrocardiography
1. STEMI (ST-Elevation Myocardial Infarction)
Mechanism: Transmural ischemia shifts the ST vector toward the epicardial (outer) surface, producing ST elevation in overlying leads with reciprocal ST depression in mirror leads.
Key ECG findings:
- Hyperacute T waves - earliest sign; tall, broad, peaked T waves before ST rise
- ST elevation - convex (domed) or straight, ≥1 mm in limb leads, ≥2 mm in precordial leads (≥1.5 mm in V2-V3 for women)
- Pathological Q waves - develop within hours-days; indicate necrosis
- T-wave inversions - follow in the evolving phase
- Reciprocal ST depression in anatomically opposite leads
Localization:
| Territory | ST Elevation | Reciprocal Depression |
|---|---|---|
| Anterior | V1-V4 | II, III, aVF |
| Inferior | II, III, aVF | I, aVL, V1-V3 |
| Lateral | I, aVL, V5-V6 | V1-V3 |
| Posterior | None (mirror image) | V1-V3 (tall R + ST depression) |
| RV | V3R-V4R | - |


2. Pericarditis
Mechanism: Diffuse epicardial inflammation causes global ST elevation without reciprocal changes (except aVR).
Key ECG findings (4 stages):
- Stage 1 - Diffuse saddle-shaped (concave up) ST elevation in most leads; PR depression (most specific finding); ST elevation in aVR is absent or depressed
- Stage 2 - ST returns to baseline, T waves flatten
- Stage 3 - Diffuse T-wave inversions
- Stage 4 - Normalization
Distinguishing from STEMI:
- Pericarditis: concave (saddle-shaped) ST elevation in all leads except aVR/V1; PR segment depression; no reciprocal depression; no Q waves
- STEMI: convex (domed) elevation, localized territory, reciprocal changes, Q waves develop
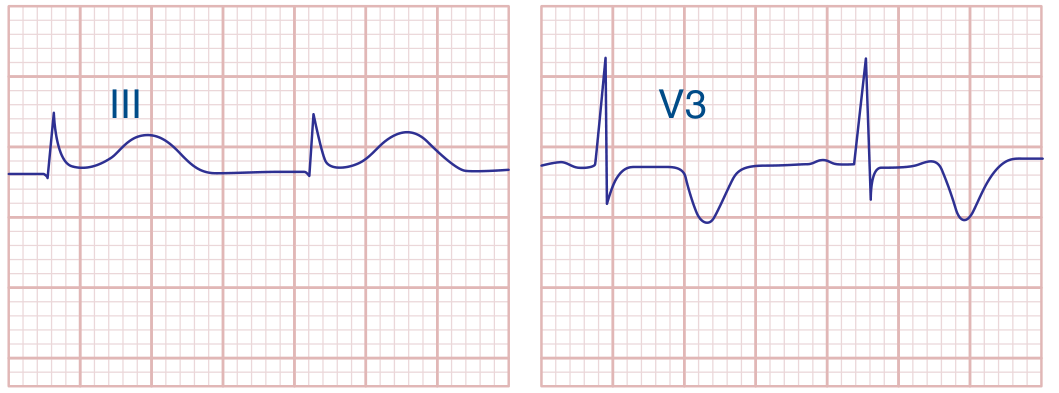
3. Pulmonary Embolism
Mechanism: Acute right heart strain due to pulmonary hypertension.
Key ECG findings:
- S1Q3T3 pattern - S wave in lead I, Q wave and T-wave inversion in lead III (classic but only ~20% sensitive)
- Sinus tachycardia - most common finding
- Right axis deviation
- New RBBB (complete or incomplete)
- T-wave inversions in V1-V4 (right heart strain - more sensitive)
- P pulmonale (tall peaked P in II)
- Atrial fibrillation (can precipitate)
Note: ECG is not diagnostic for PE alone - it helps support clinical suspicion. Normal ECG does not exclude PE.
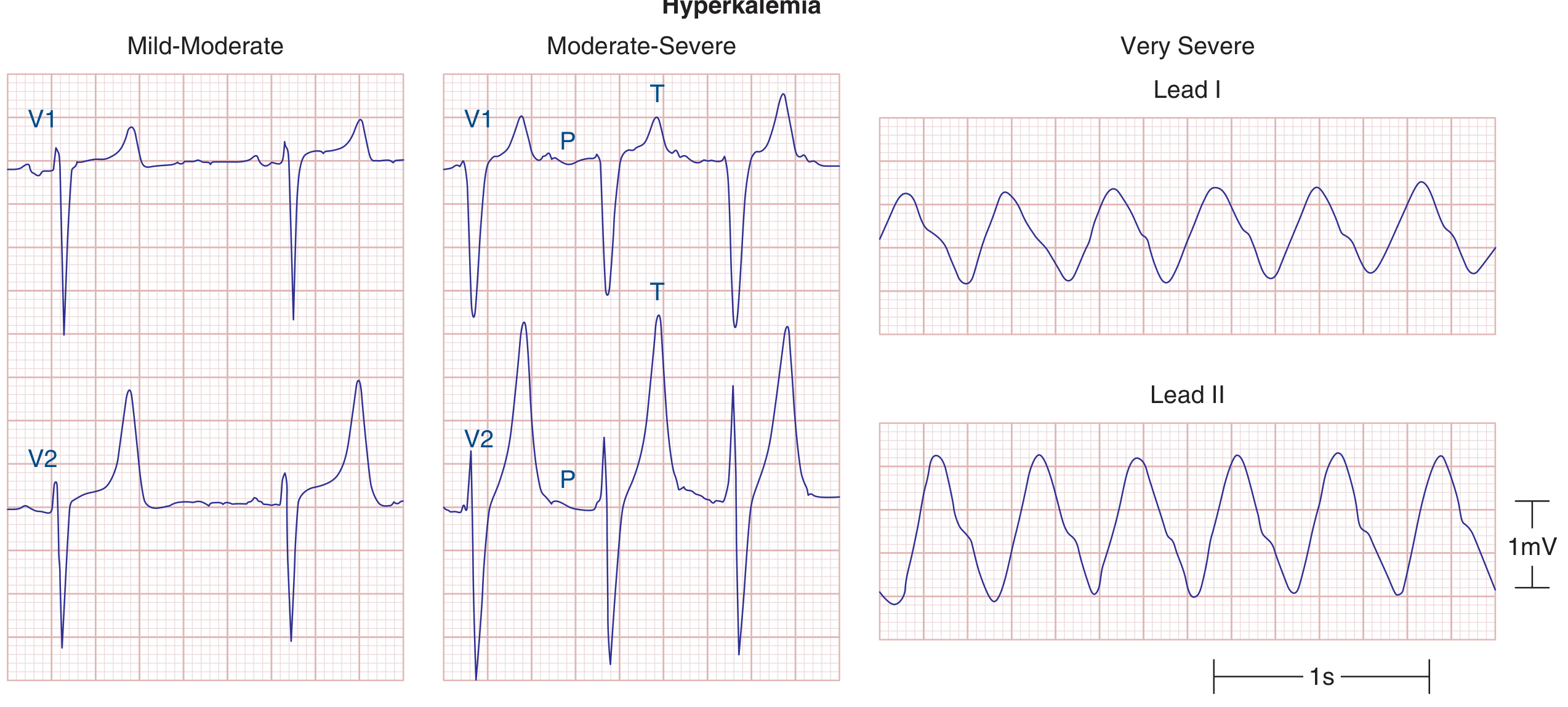
4. Hyperkalemia
Mechanism: Elevated extracellular K+ progressively reduces resting membrane potential and slows conduction throughout the heart.
Sequential ECG changes (K+ levels):
- 5.5-6.5 mEq/L: Peaked ("tented"), narrow, symmetric T waves - earliest sign
- 6.5-8 mEq/L: PR prolongation → P-wave flattening/disappearance; QRS widening
- >8 mEq/L: Wide bizarre QRS merges with T wave → sine-wave pattern → asystole
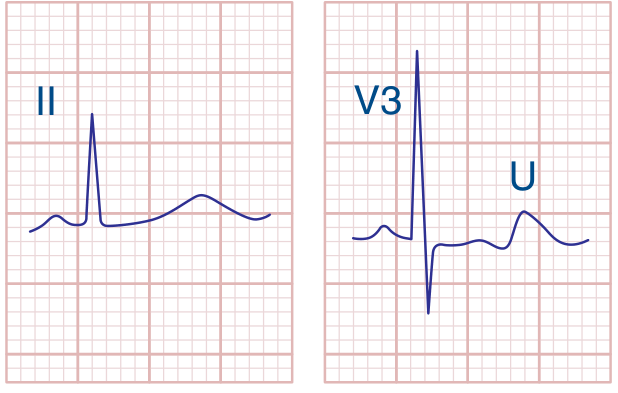
5. Hypokalemia
Mechanism: Low K+ prolongs ventricular repolarization (phase 3 action potential).
Key ECG findings:
- Prominent U waves (>1 mm, usually best seen in V2-V3) - hallmark
- ST depression
- T-wave flattening or inversion
- Apparent QT prolongation (actually QU prolongation - U wave merges with T)
- Risk of Torsades de Pointes (TdP)
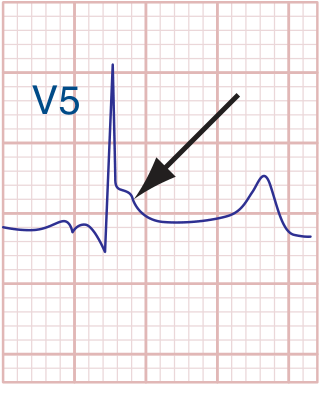
6. Hypothermia
Mechanism: Cold slows all cardiac electrical activity; abnormal early repolarization creates the Osborn wave.
Key ECG findings:
- J (Osborn) wave - pathognomonic; a positive deflection at the J point (end of QRS), most prominent in V4-V6 and inferior leads; size correlates with degree of hypothermia
- Bradycardia (sinus or junctional)
- PR, QRS, and QT prolongation
- Atrial fibrillation with slow ventricular rate
- Muscle tremor artifact (shivering)
7. Brugada Syndrome
Mechanism: Sodium channel mutation (SCN5A) causes abnormal repolarization in the right ventricular outflow tract.
Key ECG findings (two types):
- Type 1 (Brugada pattern, diagnostic): Coved (downsloping) ST elevation ≥2 mm with T-wave inversion in V1-V3; resembles RBBB but terminal S waves may be absent
- Type 2: Saddle-back ST elevation ≥2 mm in V1-V3 (not diagnostic alone; requires pharmacologic challenge)
Clinical significance: Risk of polymorphic VT/VF and sudden cardiac death in structurally normal hearts. Unmasked by fever, sodium channel blockers (flecainide, procainamide challenge used for diagnosis).
8. Wolff-Parkinson-White (WPW)
Mechanism: Accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting the ventricle before normal conduction arrives.
Key ECG findings (during sinus rhythm):
- Short PR interval (<120 ms) - AV node bypassed
- Delta wave - slurred initial QRS upstroke (pre-excitation of ventricle via accessory pathway)
- Wide QRS (>120 ms) - fusion of delta wave + normal QRS
- Secondary ST-T changes (discordant to delta wave direction)
Risk: In the setting of AF, impulses can conduct rapidly down the accessory pathway (bypassing AV node) → very fast ventricular rates → VF. Look for irregularly irregular wide-complex tachycardia with varying QRS morphology.
9. Left Bundle Branch Block (LBBB)
Mechanism: Block of the left bundle forces right-to-left ventricular activation instead of normal simultaneous activation.
Diagnostic criteria:
- QRS duration ≥120 ms
- Broad, notched (M-shaped) R waves in I, aVL, V5-V6 (lateral leads)
- rS or QS pattern in V1 (no septal Q wave)
- Absent septal Q waves in I, V5-V6
- Secondary discordant ST-T changes (T wave opposite to last QRS deflection)
Clinical note: New LBBB in the context of chest pain is treated as STEMI equivalent. Sgarbossa criteria help detect true STEMI within LBBB: concordant ST elevation ≥1 mm, concordant ST depression ≥1 mm in V1-V3, or excessive discordant ST elevation >5 mm.
10. Subarachnoid Hemorrhage (CNS Injury Pattern)
Mechanism: Massive catecholamine surge from hypothalamic stimulation causes diffuse myocardial injury (neurogenic stunned myocardium).
Key ECG findings:
- Deep, diffuse T-wave inversions - often wide and symmetric ("cerebral T waves"), most prominent in precordial leads
- Marked QT prolongation (QTc often >600 ms)
- Prominent U waves
- May mimic anterior ischemia or Wellens' pattern
- Can be associated with troponin elevation (stress cardiomyopathy/takotsubo) without obstructive CAD
Quick Reference Summary
| Disease | Most Characteristic ECG Finding |
|---|---|
| STEMI | Localized ST elevation + reciprocal depression → Q waves |
| Pericarditis | Diffuse concave ST elevation + PR depression (no reciprocal) |
| Pulmonary Embolism | S1Q3T3, sinus tachycardia, RV strain pattern |
| Hyperkalemia | Peaked T waves → wide QRS → sine wave |
| Hypokalemia | Prominent U waves, QU prolongation |
| Hypothermia | Osborn (J) waves + bradycardia |
| Brugada Syndrome | Coved ST elevation V1-V3 (Type 1) |
| WPW | Short PR + delta wave + wide QRS |
| LBBB | Broad notched R in I/V5/V6, rS in V1, ≥120 ms QRS |
| Subarachnoid Hemorrhage | Deep, wide T inversions + marked QT prolongation |
Sources: Harrison's Principles of Internal Medicine 22E, p. 1916-1918; Tintinalli's Emergency Medicine, Table 49-6; Goldberger's Clinical Electrocardiography 10th ed.
This is a shared conversation. Sign in to Orris to start your own chat.