Haemoglobin
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Now I have enough from the textbooks to give a thorough answer. Let me compile it.
Haemoglobin
Structure
Haemoglobin (Hb) is a tetrameric protein found in red blood cells. Each molecule consists of:
- 4 globin chains - in adult Hb A: 2 alpha (α) and 2 beta (β) subunits
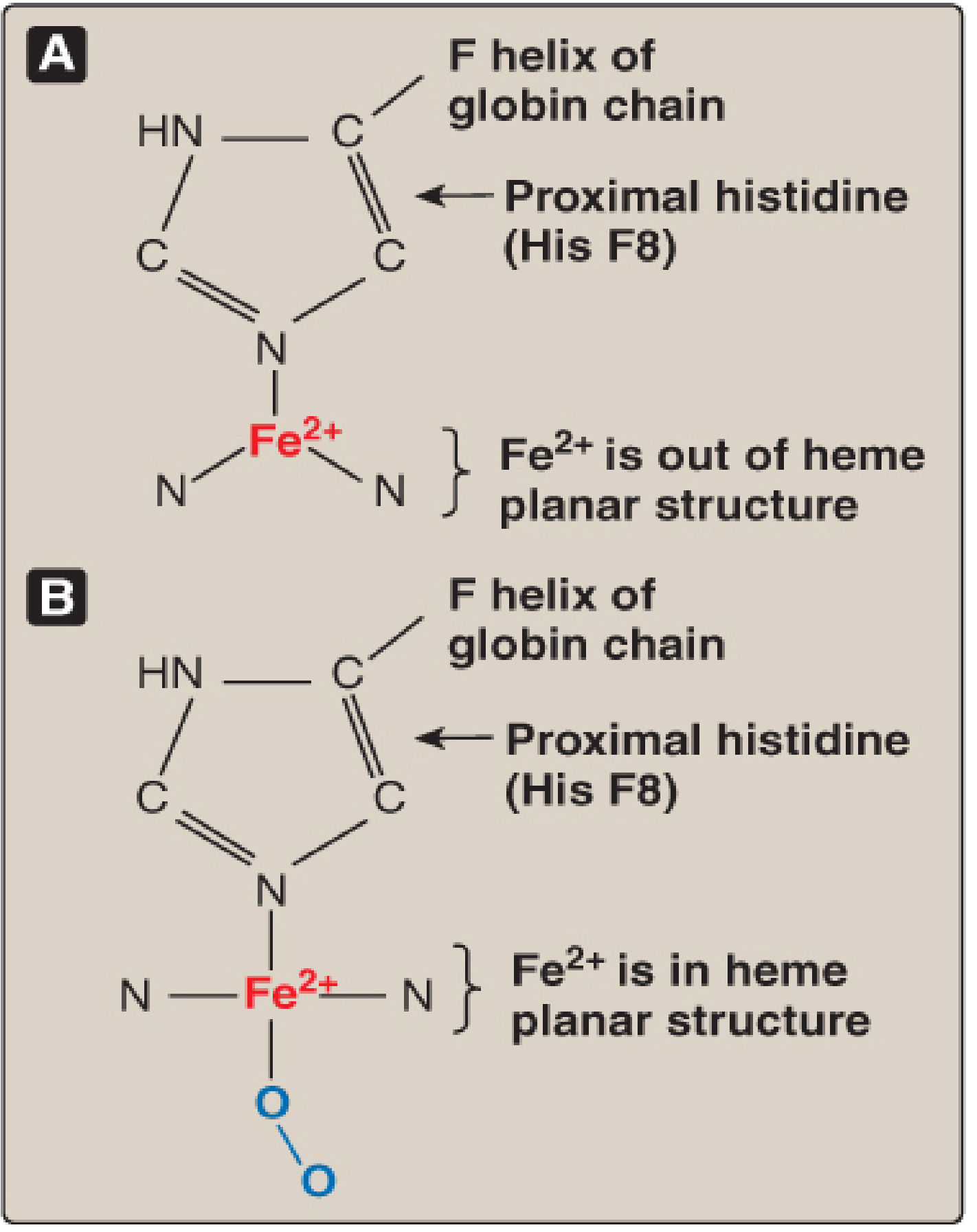
- 4 haem groups - one per subunit; each haem is a porphyrin ring with a central Fe²⁺ (ferrous iron) ion
The iron is anchored to the globin chain via the proximal histidine (His F8) on the F helix. When deoxygenated, Fe²⁺ sits slightly out of the plane of the porphyrin ring, pulling the proximal histidine and the attached helix with it. On O₂ binding, Fe²⁺ snaps into the plane, triggering a conformational shift that propagates across the whole tetramer - the structural basis of cooperative binding:
T and R States (Conformational States)
Haemoglobin exists in two interconvertible forms:
| State | Description | O₂ affinity |
|---|---|---|
| T (tense/deoxy) | Constrained by salt bridges between subunits | Low |
| R (relaxed/oxy) | Salt bridges broken after O₂ loading | High |
Cooperative binding means the affinity of haemoglobin for the last O₂ molecule bound is ~300 times greater than for the first.
The Oxygen-Dissociation Curve
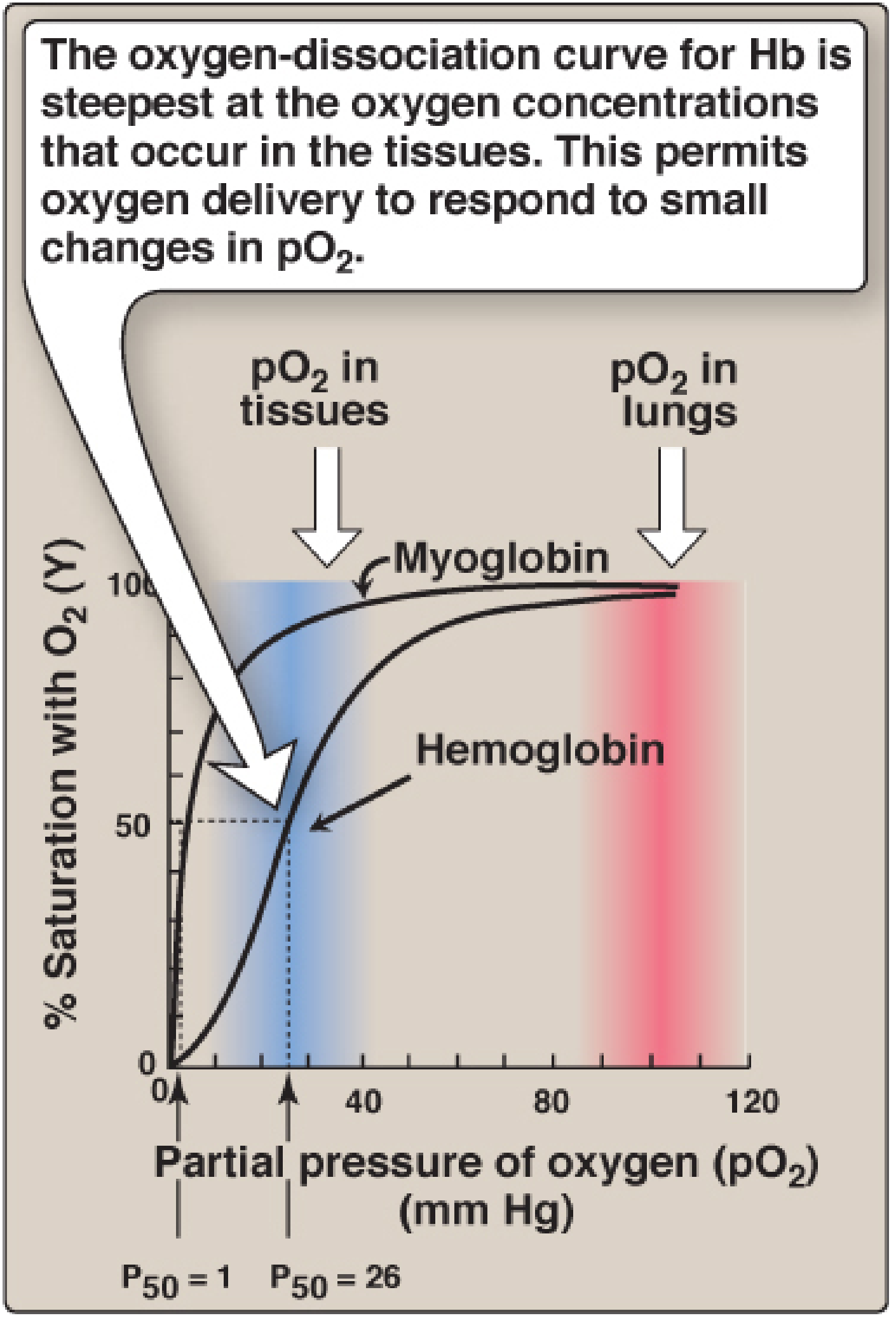
- Haemoglobin curve: sigmoidal - reflects cooperative O₂ binding
- Myoglobin curve: hyperbolic - no cooperativity (monomeric)
- P50 (pO₂ at half-saturation): ~26 mm Hg for Hb vs. ~1 mm Hg for myoglobin
- In arterial blood (pO₂ ~95 mm Hg): Hb is ~97% saturated
- In venous blood at rest (pO₂ ~40 mm Hg): Hb is ~75% saturated
- Each 100 mL of blood contains ~15 g Hb; maximum O₂-carrying capacity ~20 mL/100 mL (20 vol%)
The steep portion of the sigmoid falls precisely in the range of tissue pO₂ values, so small drops in pO₂ trigger large release of O₂ - a feature a hyperbolic (myoglobin-like) curve could not provide.
Allosteric Effectors (Factors Shifting the Curve)
1. pH and CO₂ - the Bohr Effect
A fall in pH or a rise in pCO₂ shifts the curve right (decreases O₂ affinity, raises P50). This is the Bohr effect:
- Deoxyhemoglobin binds H⁺ more avidly than oxyhemoglobin via histidine side chains with a higher pKa in the deoxy state
- In active tissues, CO₂ is converted by carbonic anhydrase to H₂CO₃ → HCO₃⁻ + H⁺, lowering pH and favouring O₂ release
- Schematically: HbO₂ + H⁺ ⇌ HbH + O₂
2. 2,3-Bisphosphoglycerate (2,3-BPG)
2,3-BPG (also called 2,3-DPG) is the most abundant organic phosphate in RBCs. It:
- Binds in a positively charged pocket between the two β-globin chains of deoxyhemoglobin only
- Stabilises the T (deoxy) form, shifting the curve right
- Equation: HbO₂ + 2,3-BPG ⇌ Hb-2,3-BPG + O₂
Clinical relevance of 2,3-BPG:
- High altitude / chronic hypoxia / chronic anaemia: 2,3-BPG levels rise, shifting the curve right and enabling greater O₂ unloading in tissues
- Stored blood: 2,3-BPG is depleted in banked blood; transfused blood has abnormally high O₂ affinity and fails to deliver O₂ properly until 2,3-BPG is restored (6-24 hours). Large transfusions of stored blood can cause tissue hypoxia
- Thyroid hormones, growth hormone, androgens: raise 2,3-BPG → raise P50
- Acidosis: inhibits glycolysis → falls 2,3-BPG (partially offsetting the rightward Bohr shift)
3. Temperature
- Raised temperature (e.g. exercising muscle): curve shifts right → more O₂ released
- Lower temperature: curve shifts left → higher O₂ affinity
CO₂ Transport
Most CO₂ is carried as bicarbonate (after carbonic anhydrase reaction). A smaller fraction binds directly to terminal amino groups of haemoglobin forming carbaminohemoglobin, stabilising the T form and reducing O₂ affinity.
Carbon Monoxide (CO) Poisoning
- CO binds haemoglobin iron with 220× greater affinity than O₂
- CO binding shifts Hb into the R conformation, causing remaining heme sites to bind O₂ with high affinity → left shift of the dissociation curve → O₂ is not released to tissues
- Result: tissue hypoxia despite normal pO₂
- Treatment: 100% O₂ (or hyperbaric O₂) to competitively displace CO
Types of Haemoglobin
| Type | Chains | Where Found |
|---|---|---|
| Hb A | α₂β₂ | Normal adult (dominant) |
| Hb A₂ | α₂δ₂ | Normal adult (~2-3%) |
| Hb F (fetal) | α₂γ₂ | Fetus/newborn; higher O₂ affinity (binds 2,3-BPG poorly) |
| Hb S (sickle) | α₂β₂(Glu→Val) | Sickle cell disease |
| Hb C | α₂β₂(Glu→Lys) | Haemoglobin C disease |
| Methaemoglobin | Fe³⁺ (oxidised) | Cannot bind O₂; caused by oxidising drugs/toxins |
Fetal Hb has high O₂ affinity because its γ-chains bind 2,3-BPG poorly, keeping it in the R state - physiologically important for extracting O₂ from maternal blood across the placenta.
Normal Reference Values
| Measure | Normal Range |
|---|---|
| Haemoglobin (males) | 13.5-17.5 g/dL |
| Haemoglobin (females) | 12.0-16.0 g/dL |
| O₂-carrying capacity | ~20 mL O₂/100 mL blood |
| Arterial saturation (SaO₂) | ~97% |
| Venous saturation (SvO₂) | ~75% at rest |
| P50 | ~26 mm Hg |
Sources: Biochemistry, 8th ed. Lippincott Illustrated Reviews; Guyton and Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th ed.
This is a shared conversation. Sign in to Orris to start your own chat.