Pneumothorax with line diagrams
Reading File
Finding Sources
Searching the Web
pneumothorax types classification mechanism line diagram medical
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Generating Image
Here is a complete, well-structured overview of pneumothorax with line diagrams.
Pneumothorax
Definition: A collection of air in the pleural space (between the visceral and parietal pleura), causing the lung to collapse partially or completely by disrupting the normally negative intrapleural pressure. - Murray & Nadel's Textbook of Respiratory Medicine
Classification - Line Diagram
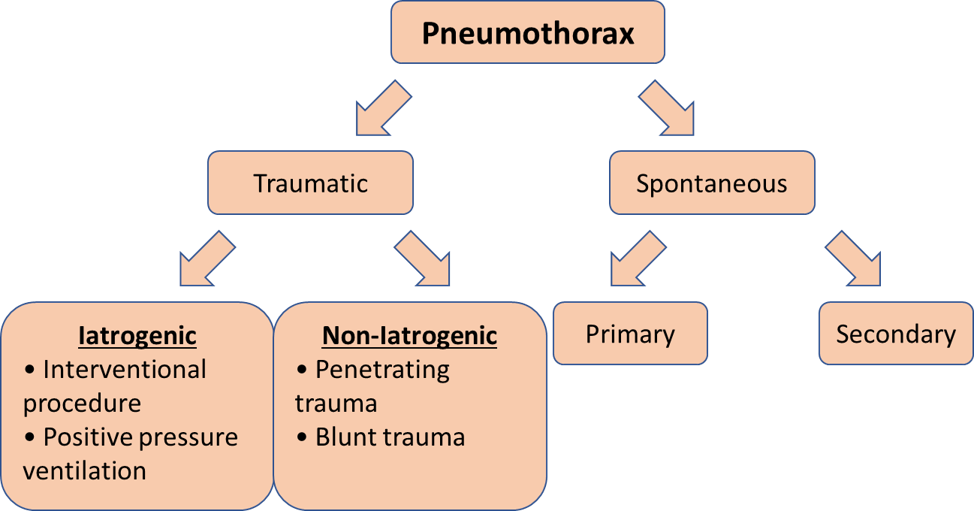
Types of Pneumothorax - Mechanisms (Line Diagram)

1. Primary Spontaneous Pneumothorax (PSP)
Definition: Occurs without a precipitating event or underlying pulmonary disease.
Mechanism:
- Air leaks from subpleural blebs or bullae (usually at the apex) into the pleural space
- Blebs form due to faster lung tissue growth than vasculature, thinning the lung at zones of highest oxygen tension
- Microscopic "pleural porosity" - large pores (10-20 μm) in mesothelial cells allow air leaks
- The result: visceral and parietal pleurae separate; lung recoils inward; chest wall expands outward
Who gets it:
- Tall, thin males aged 15-30 years
- Strong association with cigarette/marijuana smoking
- 3-7x more common in men
- Bimodal age distribution: first peak 15-34 years; rising incidence again after age 60
Features:
- Usually limited air accumulation (no valve mechanism - it is a simple/closed pneumothorax)
- Recurrence ~13% after first episode; rises to ~50% after second episode
2. Secondary Spontaneous Pneumothorax (SSP)
Definition: Pneumothorax occurring as a complication of underlying lung disease.
Common causes:
| Disease | Mechanism |
|---|---|
| COPD (most common) | Centri-acinar emphysema, rupture of emphysematous bullae |
| Asthma | Air trapping, alveolar overdistension |
| Tuberculosis | Cavitation, bronchopleural fistula |
| Pneumocystis pneumonia (PCP) | Pneumatocele formation |
| Marfan syndrome | Connective tissue defects |
| Cystic fibrosis | Chronic infection, cyst formation |
Key distinction from PSP: Patients are older (>55 years), have higher morbidity and mortality, and leaks are less likely to resolve with conservative measures. - Fischer's Mastery of Surgery
3. Traumatic Pneumothorax
A. Closed Traumatic
- Blunt chest trauma (rib fractures puncturing lung) or deceleration injury
- No communication with external environment
- Air leak is self-limiting once pressure equilibrates
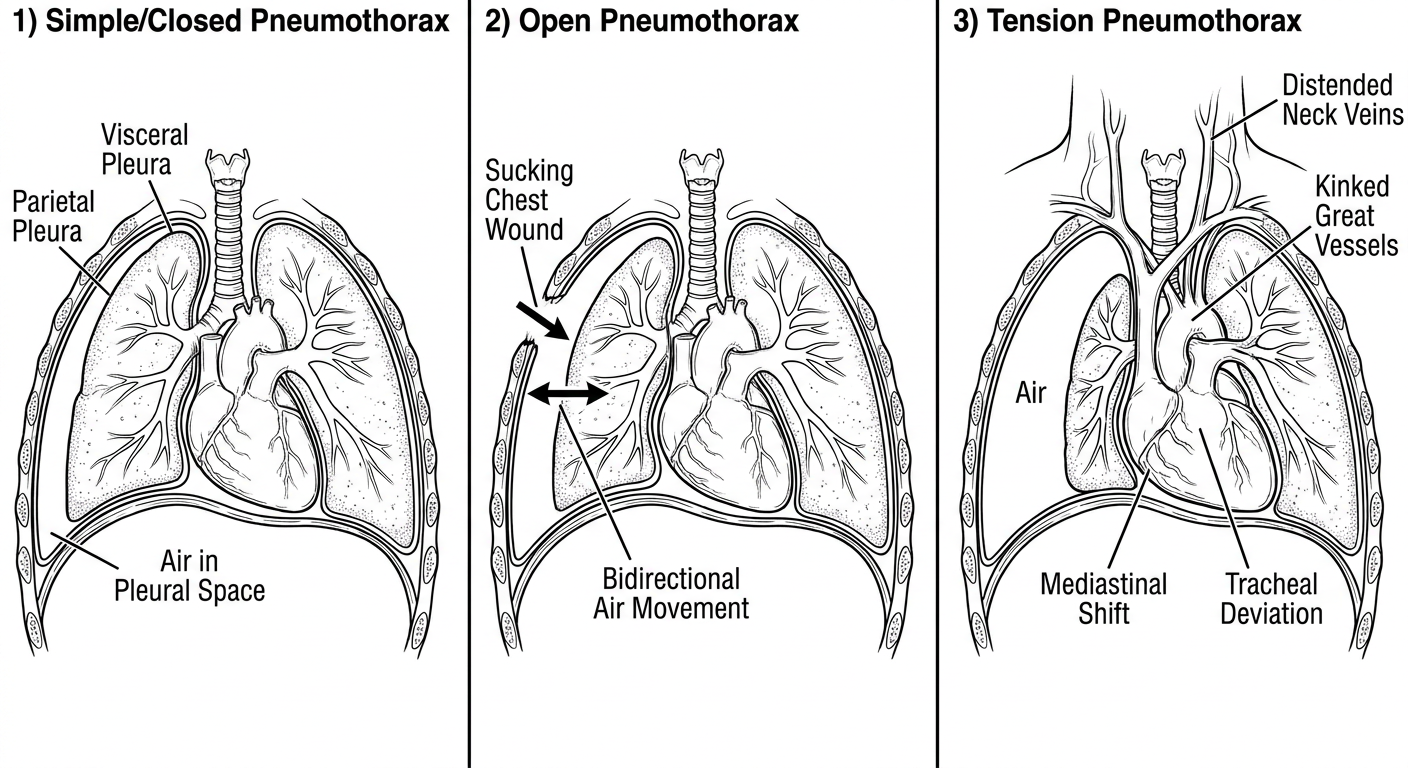
B. Open Pneumothorax ("Sucking Chest Wound")
- Large chest wall defect allows direct communication between pleural space and atmosphere
- Air flows in and out with breathing (bidirectional) - the "sucking" sound
- Lung collapses as intrapleural pressure equilibrates with atmospheric pressure
- Management: 3-sided occlusive dressing (acts as a one-way valve) + urgent chest tube
C. Iatrogenic Pneumothorax
- Complication of procedures: central line insertion, thoracentesis, lung biopsy, pacemaker insertion, positive pressure ventilation (barotrauma)
- Patients on mechanical ventilation (PPV) are at high risk of progression to tension pneumothorax
4. Tension Pneumothorax (Life-threatening)
Mechanism - One-Way Valve:
Inspiration → Air enters pleural space through defect
Expiration → Defect closes (valve), air CANNOT escape
↓
Progressive accumulation of air under pressure
↓
Ipsilateral lung: complete collapse
Mediastinum: shifts AWAY from affected side
↓
Tracheal deviation (away from lesion)
Kinking of superior/inferior vena cava
↓ venous return → ↓ cardiac output → SHOCK
Clinical Signs (The 5 T's):
- Tachycardia
- Tracheal deviation (away from affected side)
- Tension (raised JVP / distended neck veins)
- Tympanic (hyperresonance on percussion)
- Total absence of breath sounds (ipsilateral)
-
- Hypotension, elevated peak airway pressure if ventilated
This is a clinical diagnosis - do NOT wait for CXR. Treat immediately with needle decompression (2nd ICS, mid-clavicular line) followed by chest tube.
- Current Surgical Therapy 14e, Roberts & Hedges' Clinical Procedures in Emergency Medicine
5. Catamenial Pneumothorax (Special Type)
- Recurrent pneumothorax in women of reproductive age (30-35 years)
- Occurs within 72 hours before/after menstruation
- Usually right-sided
- Caused by pleural/diaphragmatic endometriosis
- Air enters through diaphragmatic fenestrations from the peritoneum
Summary Comparison Table
| Feature | PSP | SSP | Open | Tension |
|---|---|---|---|---|
| Age | 15-30 yr | >55 yr | Any | Any |
| Sex | M >> F | M > F | Any | Any |
| Cause | Blebs | Lung disease | Trauma | Valve mechanism |
| Lung collapse | Partial | Variable | Partial | Complete |
| Mediastinal shift | No | No | No | Yes |
| Immediate threat | Low | Moderate | Moderate | High |
| Treatment | Observation/drain | Drain | 3-side dressing + drain | Needle decompression |
Management Overview
Small, asymptomatic PSP (<2 cm on CXR)
→ Observe, repeat CXR at 4-6 hours, supplemental O₂
Larger or symptomatic pneumothorax
→ Simple aspiration OR small-bore chest drain (24 Fr)
→ Connect to water-seal drainage ± suction (-20 cmH₂O)
Recurrent PSP / SSP with ongoing leak
→ Video-Assisted Thoracoscopic Surgery (VATS)
→ Blebectomy + parietal pleurectomy + mechanical/chemical pleurodesis
Tension pneumothorax
→ IMMEDIATE needle decompression (14-16G cannula, 2nd ICS MCL)
→ Then chest drain
Open pneumothorax
→ 3-sided occlusive dressing → chest drain (away from wound)
- Fischer's Mastery of Surgery, Current Surgical Therapy 14e, Roberts & Hedges' Clinical Procedures in Emergency Medicine
CN u make one closed tension pneumothorax diagrams for exam clearly showing difference
Generating Image
Here are the key exam points to remember alongside the diagram:
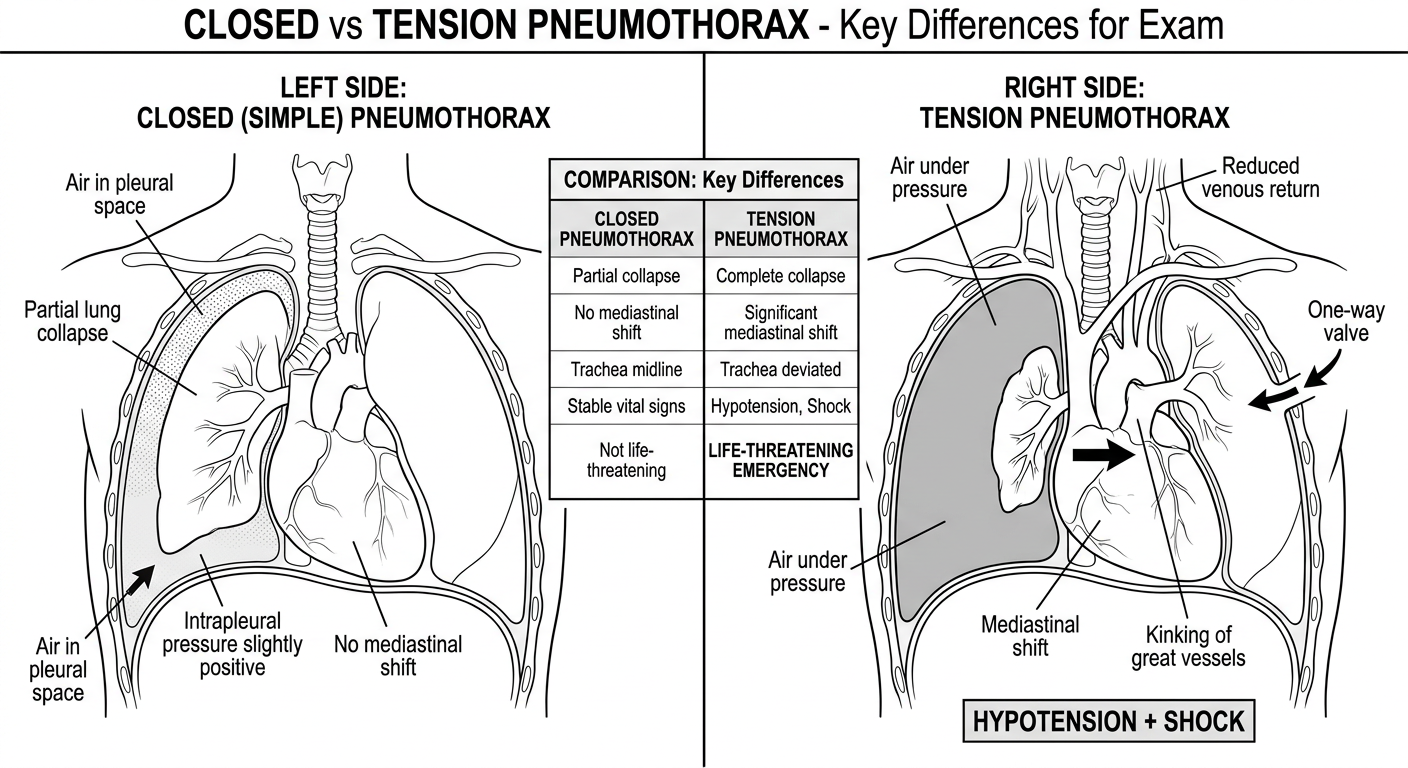
Closed vs Tension Pneumothorax - Exam Summary
| Feature | Closed (Simple) | Tension |
|---|---|---|
| Air entry | One-time leak, self-limiting | Continuous, one-way valve |
| Lung collapse | Partial | Complete |
| Mediastinal shift | None | Away from lesion |
| Tracheal deviation | None | Away from lesion |
| Intrapleural pressure | Slightly positive, then equalizes | Progressively increasing |
| JVP / neck veins | Normal | Distended |
| BP | Normal | Hypotension / Shock |
| Trachea | Midline | Deviated contralaterally |
| Breath sounds | Reduced ipsilaterally | Absent ipsilaterally |
| Emergency? | No | YES - immediate action |
| Treatment | Observation / chest drain | Needle decompression FIRST (2nd ICS, MCL) then chest tube |
The One-Way Valve - Key Concept for Exams
The single most important difference is the valve mechanism in tension pneumothorax:
- Inspiration → air is sucked INTO pleural space through the defect
- Expiration → defect closes like a flap valve → air CANNOT escape
- Each breath adds more air under pressure
- This progressively compresses the lung, shifts the mediastinum, kinks the SVC/IVC → preload drops → cardiac output falls → obstructive shock
Mnemonic for tension pneumothorax signs: "3 Aways"
- Trachea deviates away
- Mediastinum shifts away
- Treat it before it takes you away (i.e., it's immediately life-threatening - don't wait for CXR!)
This is a shared conversation. Sign in to Orris to start your own chat.