Blisters
Reading File
Asking for Preferences
Finding Sources
Searching the Web
skin blisters types causes management clinical overview
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive material. Let me now compose a thorough, well-organized overview of blisters.
Blisters - A Clinical Overview
Terminology
The terms for blisters depend on size:
- Vesicle - a circumscribed, fluid-filled elevation less than 1 cm in diameter. The apex may be rounded, pointed (acuminate), or umbilicated (as in eczema herpeticum). Vesicles may be discrete, grouped (herpes zoster), or linear (poison ivy contact dermatitis).
- Bulla - a rounded or irregularly shaped fluid-filled blister larger than 1 cm. Fluid is serous or serosanguineous.
Vesicles can coalesce or enlarge into bullae. Both can contain clear serous fluid, blood (hemorrhagic), or become secondarily infected (vesicopustule).
Andrews' Diseases of the Skin, p. 24-25
Where the Blister Forms (Level of Split)
The anatomical level of cleavage is diagnostically important:
| Level | Appearance | Examples |
|---|---|---|
| Intraepidermal (within epidermis) | Flaccid, thin-walled; ruptures easily; leaves moist erosion or thin crust | Pemphigus vulgaris, friction blisters, SSSS |
| Subepidermal (below epidermis/dermo-epidermal junction) | Tense, thick-walled; does NOT rupture easily; often present intact on examination | Bullous pemphigoid, dermatitis herpetiformis, burns |
Friction blisters specifically split just below the stratum granulosum - the blister roof consists of stratum corneum + stratum granulosum, while the floor is formed by pale, degenerated keratinocytes. Dermatology 2-Volume Set 5e, p. 679
Categories and Causes
1. Physical / Mechanical
- Friction blisters - the most common type. Rubbing of moist skin (new shoes, sports, military training) causes intraepidermal splitting. Common sites: soles, heels, palms, fingers. Risk factors: ill-fitting shoes, heat, sweating. Prevalence in military foot studies: ~33%.
- Fracture blisters - overlie closed fractures (especially ankle/lower leg); appear days to 3 weeks after injury from vascular compromise. Heal in 5-14 days but can complicate surgical planning. Blood-filled or diabetic-patient blisters carry higher infection risk.
- Coma/pressure blisters - form within 48-72 hours of prolonged immobilization or loss of consciousness. Associated historically with barbiturates but also opioids, benzodiazepines, CVA, hypoglycemia, viral encephalitis. Appear at pressure sites; heal over 1-2 weeks if patient survives. Characteristic histology: sweat gland necrosis.
2. Thermal / Environmental
- Burns (2nd and 3rd degree) - subepidermal blisters at burn sites
- Sunburn (severe)
- Frostbite
- Chemical irritants / contact dermatitis
3. Infectious
| Organism | Disease | Blister Type |
|---|---|---|
| Staphylococcus aureus | Bullous impetigo; SSSS | Flaccid superficial |
| Herpes simplex virus 1/2 | Oral/genital herpes, cold sores | Grouped vesicles, weep clear fluid then crust |
| Varicella-zoster virus | Chickenpox; Shingles (herpes zoster) | Grouped dermatomal vesicles |
| Coxsackievirus | Hand, foot, and mouth disease | Oval vesicles on hands/feet/mouth |
4. Autoimmune Blistering Diseases
| Disease | Level of Split | Autoantibody Target | Key Feature |
|---|---|---|---|
| Pemphigus vulgaris | Intraepidermal (suprabasal) | Desmoglein 3 (+ desmoglein 1) | Positive Nikolsky sign; flaccid bullae; mucous membrane involvement |
| Bullous pemphigoid | Subepidermal | BP180, BP230 | Tense bullae; elderly; pruritic |
| Dermatitis herpetiformis | Subepidermal | Transglutaminase 3 | Intensely pruritic; associated with celiac disease |
| Epidermolysis bullosa acquisita (EBA) | Subepidermal | Collagen VII | Trauma-induced blisters; can mimic friction blisters |
| Linear IgA disease | Subepidermal | BP180 ectodomain | "Crown of thorns" pattern |
5. Metabolic / Systemic
- Edema blisters (hydrostatic bullae) - develop in patients with acute exacerbation of chronic edema or anasarca, particularly in elderly, immobile, or hospitalized patients. The tense bullae are non-inflammatory and surrounded by edematous skin. They resolve when the underlying edema resolves. Dermatology 2-Volume Set 5e, p. 683
- Bullosis diabeticorum - spontaneous blisters in diabetic patients, typically on the lower extremities
6. Drug-Induced
- Fixed drug eruption, Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), bullous drug reactions
Key Diagnostic Signs
| Sign | Technique | Positive Result | Significance |
|---|---|---|---|
| Nikolsky sign | Lateral pressure on uninvolved skin | Epithelium shears off | Intraepidermal split (pemphigus, SSSS, SJS/TEN) |
| Asboe-Hansen sign | Pressure on top of a blister | Blister extends into adjacent skin | Demonstrates sub-clinical vesiculation |
Both signs indicate that microscopic vesiculation extends beyond what is visible. Andrews' Diseases of the Skin, p. 25
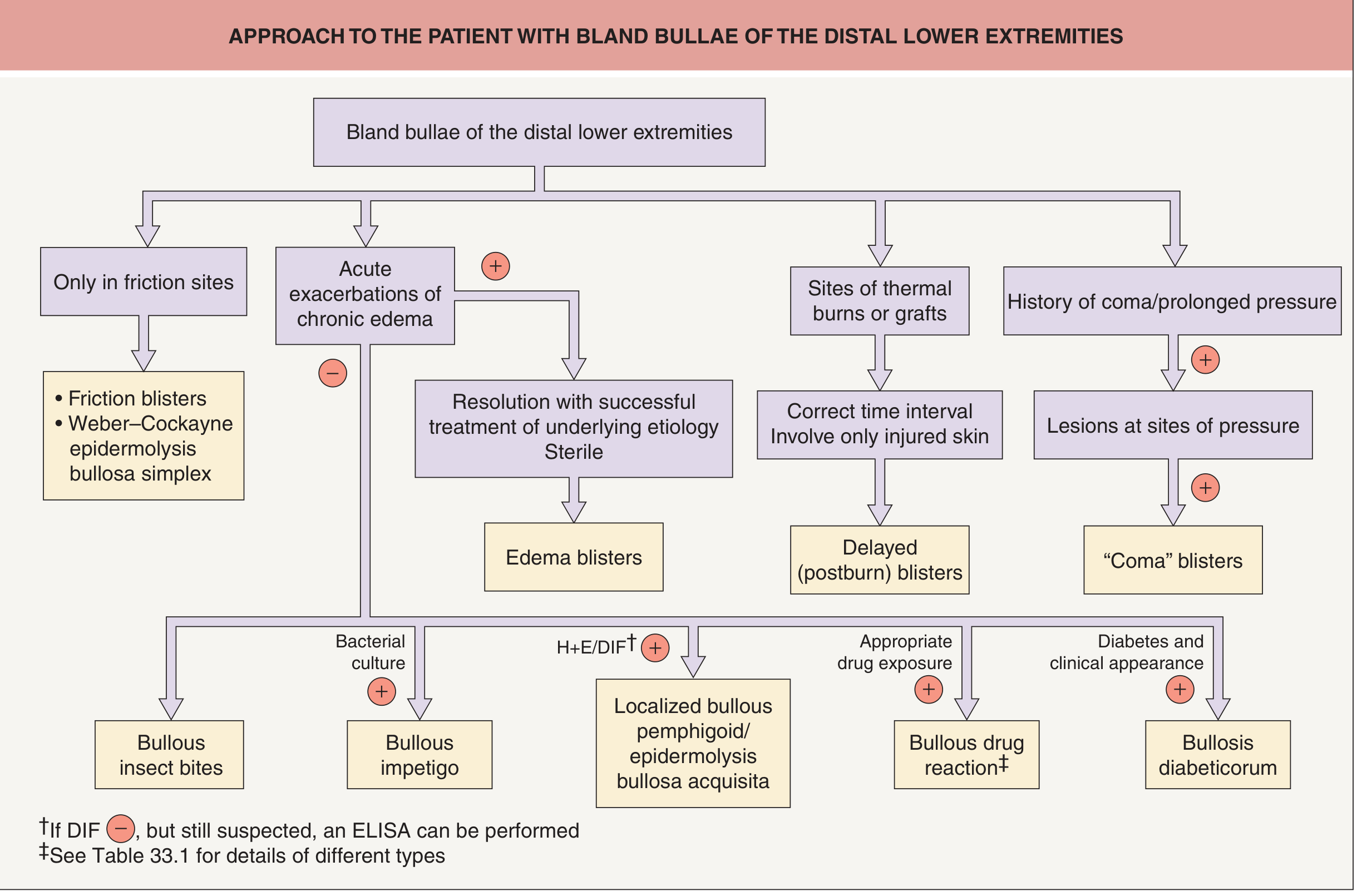
Diagnostic Approach
Here is a helpful flowchart for bland (non-inflammatory) bullae of the lower extremities, from Dermatology 2-Volume Set 5e:
For inflammatory or widespread blisters, further workup includes:
- Skin biopsy for H&E histology (level of split, inflammatory infiltrate)
- Direct immunofluorescence (DIF) - essential for autoimmune bullous diseases
- Indirect immunofluorescence (IIF)
- ELISA for specific autoantibodies (desmoglein 1 and 3, BP180, BP230, collagen VII)
- Bacterial culture if infection is suspected
- Tzanck smear (for herpetic infections - shows multinucleated giant cells)
Management
General Principles
Intact blisters:
- Intact blisters provide some pain relief and act as a physiologic dressing that rarely becomes infected
- Large blisters (painful, tense) can be drained by needle puncture at the edge, but the roof should be left in place - it acts as its own dressing and protects the raw floor
- Needle aspiration alone (without unroofing) is NOT recommended for burn blisters - it may increase infection risk without the debridement benefit
Ruptured blisters:
- Ruptured blisters should be debrided; once the blister roof is gone, the fluid becomes a culture medium
- Clean with antiseptic, apply a non-adherent dressing
- Anticipate pain on exposure to air - offer analgesia before debridement
Roberts and Hedges' Clinical Procedures in Emergency, p. 38.14
By Type
| Type | Specific Management |
|---|---|
| Friction blisters | Drain if symptomatic; keep roof intact; cushioning, acrylic-fiber socks for prevention; 20% aluminum chloride hexahydrate reduces recurrence in hikers/soldiers |
| Fracture blisters | Conservative - most heal in 5-14 days; blood-filled blisters and diabetic patients need close monitoring |
| Burn blisters | Controversial; intact blisters left in place vs. early debridement both acceptable; no aspiration; analgesia when debriding |
| Edema blisters | Treat underlying edema; blisters resolve with successful edema management |
| Coma blisters | Supportive; treat underlying cause; blisters heal in 1-2 weeks |
| Infectious blisters | Antivirals (acyclovir for HSV/VZV); topical/oral antibiotics for bullous impetigo |
| Autoimmune bullous diseases | Systemic corticosteroids; steroid-sparing agents (azathioprine, mycophenolate, dapsone, rituximab depending on type) |
Prevention
- Well-fitting footwear; moisture-wicking (acrylic fiber) socks
- Gradual conditioning (breaking in new shoes, building up calluses)
- Protective padding/gloves for repetitive activities
- Skin lubricants for at-risk areas (though they reduce efficacy of topical preventives)
Special Notes
- Hemorrhagic bullae are common in pemphigus, herpes zoster, severe drug reactions, and lichen sclerosus
- Cytology of blister fluid can help confirm pemphigus (acantholytic cells), herpes zoster, and herpes simplex
- Sucking blisters are a specific type seen in neonates from in-utero sucking activity - benign and self-resolving
This is a shared conversation. Sign in to Orris to start your own chat.