Arsenic poisoning
Reading File
Finding Sources
Searching PubMed
arsenic poisoning toxicology
Searching the Web
arsenic poisoning clinical features treatment 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
I now have all the material needed for a thorough, well-illustrated answer. Let me compile it.
Arsenic Poisoning
Arsenic is a naturally occurring metalloid that exists in inorganic and organic forms. Inorganic arsenic (especially trivalent arsenite, As³⁺) is far more toxic than organic forms. It is classified as a corrosive irritant poison.
Sources of Exposure
- Pesticides/insecticides: Paris green (copper arsenite), calcium arsenate, lead arsenate
- Contaminated groundwater (most common worldwide cause)
- Industrial exposure: smelting, semiconductor manufacturing, wood preservatives (CCA)
- Homicidal/suicidal ingestion: arsenic trioxide
- Medicinal: arsenic trioxide is used in acute promyelocytic leukemia (APL) treatment
- Arsine gas (AsH₃): occupational inhalation hazard
- Food: seafood contains organic arsenic (less toxic)
Permissible limit of arsenic in groundwater: 0.05 mg/liter.
Mechanism of Toxicity
Arsenic exerts toxicity through multiple mechanisms:
- Sulphydryl (SH) group binding - reversibly combines with SH groups in tissue proteins and enzymes, disrupting cellular metabolism
- Inhibition of pyruvate dehydrogenase and other enzymes essential for the Krebs cycle (arsenite binds lipoic acid)
- Arsenate uncoupling - pentavalent arsenate substitutes for phosphate in oxidative phosphorylation, uncoupling ATP synthesis
- Capillary toxin - dilates and damages capillaries, causing transudation of fluid, especially in the gut
- Direct organ damage: fatty degeneration of liver, renal tubular necrosis, peripheral axonal neuropathy with myelin fragmentation
Pharmacokinetics
- Absorption: oral (main route), dermal (arsenite), inhalation (arsine gas), rectal/vaginal
- Distribution: early - highest in liver, then kidneys and spleen. Arsenic has a high affinity for keratin, accumulating in hair and nails within hours. It replaces phosphorus in bone. Does NOT cross the blood-brain barrier easily but crosses the placenta.
- Elimination: mainly renal (as methylated arsenic - monomethylarsine, dimethylarsine), also in feces, bile, sweat, milk. Urinary excretion is continuous for ~10-12 days.
Acute Arsenic Poisoning
Fatal Dose and Period
- Fatal dose: ~180 mg of arsenic trioxide (range varies with compound and tolerance)
- Fatal period: 12-48 hours (can be fatal within 2-3 hours)
- Symptoms typically begin within 30 minutes of oral ingestion
Clinical Features
| Stage | Features |
|---|---|
| Early (minutes) | Metallic taste, garlicky odour on breath, xerostomia (dry mouth), dysphagia |
| GI (prominent) | Severe nausea, projectile vomiting (dark brown/yellow, contains blood and mucus), colicky abdominal pain, profuse diarrhoea - stools initially dark and bloody, later rice water (resembling cholera) |
| Systemic | Dehydration, cold clammy skin, pale anxious face, shrunken eyes, intense thirst, increased salivation |
| Cardiovascular | Hypotension, shock, ECG shows T-wave inversion and prolonged QT interval, congestive cardiomyopathy, ventricular arrhythmias |
| CNS | Restlessness, delirium, encephalopathy, convulsions, coma |
| Respiratory | Laboured breathing; if arsine gas inhaled: frothy sputum, pulmonary oedema, cyanosis, corneal ulcer, conjunctivitis |
Cramps in calf muscles are characteristic. Death from acute arsenic poisoning is usually caused by irreversible circulatory insufficiency.
Delayed Features (2-8 weeks post-acute)
- Hair loss (alopecia)
- Aldrich-Mees lines (white transverse striae on nail plates, 1-2 mm wide, appear ~5 weeks post-exposure)
- Sensorimotor peripheral neuropathy (ascending, glove-and-stocking distribution)
- Pancytopenia (within 1 week), basophilic stippling of erythrocytes
Differential Diagnosis: Arsenic vs. Cholera
| Feature | Arsenic Poisoning | Cholera |
|---|---|---|
| Pain in throat | Before vomiting | After vomiting |
| Purging | After vomiting | Before vomiting |
| Stools | Dark-colored/bloody, later rice-watery | Rice-watery, not bloody, continuous involuntary jet |
| Tenesmus | Present | Absent |
| Vomited matter | Contains mucus, bile, blood | Watery; without mucus, bile, blood |
| Voice | Not affected | Rough and whistling |
| Conjunctivae | Inflamed | Not inflamed |
From: The Essentials of Forensic Medicine and Toxicology, 36th ed.
Chronic Arsenic Poisoning
Chronic poisoning occurs from repeated small doses. Overt effects appear after chronic absorption of >0.01 mg/kg/day (~500-1000 mcg/day in adults).
Skin Changes (most characteristic)
- Raindrop pigmentation: finely mottled brown hyperpigmentation on flexures, temples, eyelids, neck - persists for months
- Hyperkeratosis of palms and soles
- Dry, scaly desquamation with hyperpigmentation over trunk and extremities
Palmar keratosis in chronic arsenic poisoning:

Mees Lines (Aldrich-Mees Lines)
White transverse striations of the nails (striate leukonychia) appear 3-6 weeks after exposure. The distance of Mees lines from the nail base can be used to estimate the time of exposure (nails grow ~1 mm/week).

Mees Lines in Arsenic Neuropathy - from Bradley and Daroff's Neurology in Clinical Practice
System-by-System Chronic Effects
| System | Features |
|---|---|
| Nervous | Sensorimotor peripheral neuropathy (stocking-glove dysesthesia), encephalopathy, convulsions |
| Skin | Raindrop pigmentation, hyperkeratosis (palms/soles), Mees lines, hair/nail brittleness, alopecia |
| Eyes | Conjunctivitis, photophobia, watering |
| GI | Nausea, vomiting, abdominal cramps, diarrhoea, salivation |
| CVS/Renal | Chronic nephritis, cardiac failure, dependent oedema, peripheral vascular disease |
| Liver | Hepatomegaly, jaundice, cirrhosis, noncirrhotic portal hypertension |
| Haematologic | Bone marrow suppression, hypoplasia, anaemia, thrombocytopenia |
| Carcinogenic | Lung, skin, bladder, kidney, and liver cancer (years after exposure); tobacco smoking synergistically increases risk |
| Reproductive | Teratogenic; can cross placenta |
Diagnosis
- Urine arsenic (test of choice): Monomethylarsine and dimethylarsine appear in urine within 24 hours of ingestion
- Urinary arsenic >200 mcg/24 hr = indicative of toxic exposure
- Normal urine arsenic: <0.03 mcg/L
- Acute poisoning: 24-hr excretion >100 mcg
- Blood arsenic: only useful very early (arsenic disappears rapidly from blood); not recommended for diagnosis except in anuric patients
- Hair and nails: arsenic appears in hair and nails within hours; >3 ppm (100 mg per 100g specimen) is diagnostic of chronic arsenic ingestion. Enables timeline reconstruction.
- Liver arsenic at autopsy: >1 mg% is significant
- Methods: atomic absorption spectroscopy, neutron activation analysis, colorimetry, polarography
Treatment
Acute Poisoning
- Remove source of exposure immediately
- Gastric lavage (if within 1-2 hours of ingestion) with water or dilute sodium bicarbonate
- Activated charcoal (limited efficacy but can be administered)
- IV fluids (normal saline) for dehydration and shock correction
- Chelation therapy - the cornerstone of treatment:
- Unithiol (DMPS): 3-5 mg/kg IV every 4-6 hours (preferred)
- Dimercaprol (BAL): 3-5 mg/kg IM every 4-6 hours for 2 days, then 6-hourly for 1 day, then 12-hourly; total dose ~2.5-3 mg/kg body weight. Stop if side effects: nausea, vomiting, tachycardia, hypotension, throat constriction
- Succimer (DMSA): effective but only available orally in the US; avoid in initial acute phase due to poor GI absorption from splanchnic oedema
- D-Penicillamine: 100 mg/kg/day in 4 divided doses for 4-8 days, given after initial 12-48 hours of BAL therapy
- Chelation is most effective when given within minutes to hours of exposure; do not wait for lab confirmation if clinical suspicion is high
- Stop chelation when 24-hr urine arsenic falls below 50 mcg/24 hr
- Sodium thiosulphate 10% (7.5g IV) - of doubtful value
- Castor oil or magnesium sulphate to reduce intestinal absorption
- Morphine for pain relief
- Demulcents: ghee, barley water
- Monitor ECG for QTc prolongation and arrhythmias
Arsine Gas Poisoning
- Fresh air + oxygen inhalation
- Exchange transfusion
- Haemodialysis
- Alkaline drinks
- Note: BAL is NOT effective for arsine gas poisoning
Chronic Poisoning
- Remove from source of exposure
- BAL administration
- Supportive care
Autopsy Findings
External:
- Prolonged rigor mortis
- General shrunken appearance (dehydration)
- Shrunken eyeballs, cyanosis of hands and feet, jaundice
Internal:
- Stomach: mucous membrane inflamed and ulcerated; "red velvet appearance" with lines of redness along rugae; sticky mucus covers mucosa; arsenic particles may be visible
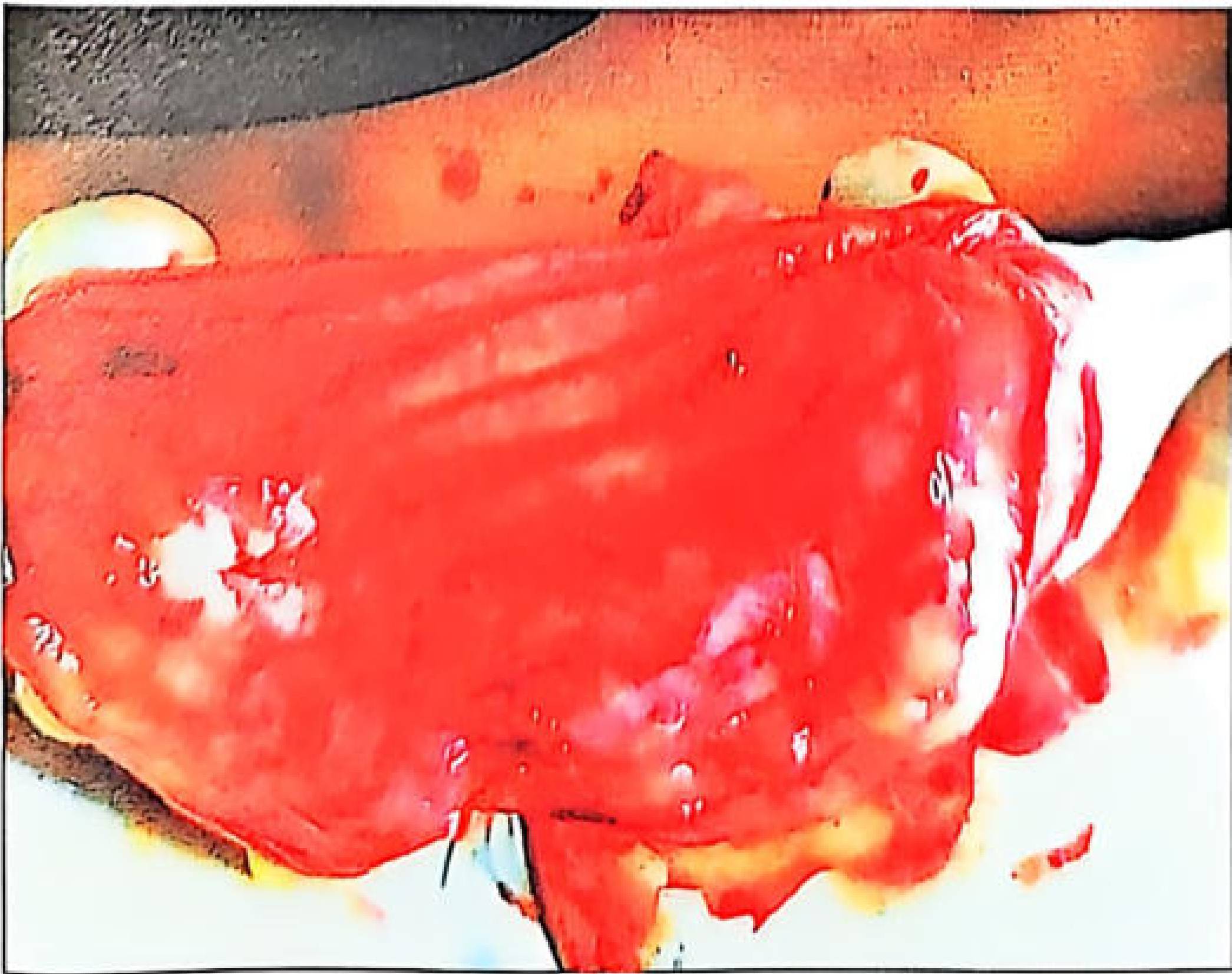
Stomach mucosa in arsenic poisoning - from The Essentials of Forensic Medicine, 36th ed.
- Intestine: flaccid, pale-violet mucosa, submucous hemorrhages along its length, large flakes of mucus
- Subendocardial petechial hemorrhages of the ventricle (characteristic and highly suggestive of arsenic poisoning)
- Liver: fatty degeneration, possibly necrosis
- Kidneys: acute tubular necrosis, glomerulonephritis
- Lungs: congestion, subpleural ecchymoses, pulmonary oedema
- Brain: oedema, patchy necrosis, hemorrhagic encephalitis; congested meninges
Medico-legal Aspects
- Arsenic poisoning is most commonly homicidal because arsenic is colourless, tasteless, and odourless when dissolved, making it easy to administer covertly
- Arsenic is also used for suicidal and accidental ingestion (pesticide workers)
- Hair and nail analysis is critical for timeline reconstruction in suspected homicide
- Segments of hair closest to the scalp represent the most recent exposure; distance of Mees lines from nail base helps estimate timing
- Arsenic is preserved in the body for years, including after putrefaction, making exhumation and toxicologic analysis valuable
Key Numbers Summary
| Parameter | Value |
|---|---|
| Fatal dose (As₂O₃) | ~180 mg |
| Fatal period | 12-48 hours |
| Symptom onset (oral) | Within 30 minutes |
| Urinary toxic threshold | >200 mcg/24 hr |
| Mees lines appearance | 3-6 weeks post-exposure |
| Hair diagnostic level | >3 ppm (100 mg/100g) |
| BAL chelation dose | 2.5-3 mg/kg body weight |
| Permissible As in water | 0.05 mg/L |
Sources: P.C. Dikshit Textbook of Forensic Medicine and Toxicology | The Essentials of Forensic Medicine and Toxicology, 36th ed. (2026) | Katzung's Basic and Clinical Pharmacology, 16th ed. | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.