Thyrotoxicosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"thyrotoxicosis" AND "management"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the information needed to write a comprehensive answer. Let me compile it.
Thyrotoxicosis
Definition and Distinction from Hyperthyroidism
Thyrotoxicosis is a physiologic process manifesting as hypermetabolism and hyperactivity caused by high serum concentrations of T4, T3, or both. It is not necessarily caused by excess hormone production - it can occur with normal or even reduced thyroid synthetic activity (e.g., thyroiditis leaking preformed hormone). Hyperthyroidism, in contrast, specifically refers to increased thyroid hormone biosynthesis and secretion. This distinction is clinically important - Scott-Brown's classifies causes into "thyrotoxicosis with hyperthyroidism" and "thyrotoxicosis without hyperthyroidism."
- Textbook of Family Medicine 9e, p. 1021
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Causes and Classification
| Thyrotoxicosis WITH Hyperthyroidism | Thyrotoxicosis WITHOUT Hyperthyroidism | |
|---|---|---|
| Common | Graves' disease, Toxic multinodular goitre, Solitary toxic adenoma | Silent (painless) thyroiditis, Postpartum thyroiditis, Subacute thyroiditis, Exogenous thyroid hormone |
| Uncommon | TSH-secreting pituitary adenoma, Iodine-containing drugs (amiodarone), Pituitary resistance to thyroid hormone, Neonatal Graves' disease, Hyperemesis gravidarum, Struma ovarii, Metastatic follicular thyroid carcinoma | Drug-induced thyroiditis (amiodarone, lithium, interferon-α), Acute infectious thyroiditis, Radiation thyroiditis, 'Hamburger' thyrotoxicosis |
Graves' disease accounts for 60-90% of all cases. Autonomous functioning nodules have a much higher incidence in iodine-deficient areas, accounting for approximately 60% of cases in those regions.
Epidemiology
- More common in females and in persons of northern European extraction; rare in Black populations.
- Graves' disease most commonly affects women aged 30-60, but can occur in children and men.
- Autonomous functioning nodules show higher incidence in iodine-deficient regions.
- Atrial fibrillation occurs more often in older individuals (5-15%).
Pathophysiology
In Graves' disease, TSH-receptor stimulating antibodies (TSH-RS Abs / TSI) bind to TSH receptors on the thyroid, mimicking TSH and stimulating T4 production and release. This suppresses the pituitary feedback loop, driving sTSH to levels significantly below 0.01 mIU/L.
Circulating T4 and T3 enter cells, where T4 is converted to the active T3. T3 passes into the nucleus, binds thyroid hormone receptors, and induces gene activation and transcription, producing tissue-specific effects. In the pituitary, thyroid hormones exert negative regulation (TSH suppression). Many symptoms arise from adrenergic hyperactivity - increased sensitivity to catecholamines.
Of all clinical manifestations, cardiovascular complications represent the highest potential for morbidity and mortality (Tietz Laboratory Medicine).
Clinical Features
Symptoms
- Weight loss (with paradoxically increased appetite - due to elevated BMR)
- Anxiety, agitation, irritability, insomnia
- Palpitations, tachycardia, dyspnea
- Heat intolerance, sweating
- Diarrhea (increased stool frequency; frank diarrhoea is rare)
- Menstrual irregularity, oligomenorrhoea
- Fatigue and proximal muscle weakness
- Hair loss, brittle nails
Signs
- Sinus tachycardia, wide pulse pressure
- Atrial fibrillation (especially in elderly >60 years)
- Fine tremor
- Warm, moist skin; palmar erythema
- Onycholysis
- Proximal myopathy, muscle wasting
- High-output heart failure
- Thyroid bruit (Graves' disease)
- Goitre (>90% in Graves' disease)
- Ophthalmopathy (exophthalmos/proptosis - Graves' specific)
Special Presentations
- Apathetic thyrotoxicosis: Occurs in the elderly; presents with apathy, lethargy, pseudodementia, weight loss, depression - without the classic hyperadrenergic symptoms. Easy to miss; a screening sTSH should be included in every dementia/depression workup.
- Elderly: Age-related desensitization of β-adrenergic receptors blunts classic symptoms; cardiovascular dysfunction, dyspnea, and proximal weakness predominate.
Diagnosis
Key labs:
- sTSH: suppressed (<0.1 mIU/L for hyperthyroidism; typically <0.01 mIU/L in Graves')
- Elevated FT4 and FT3
- TSH-RS Abs (TSI): positive in Graves'
Diagnosis pearls:
- sTSH >0.05 mIU/L makes Graves' suspect
- Graves' without goitre and without ophthalmopathy should raise suspicion
- If FT4 and FT3 are elevated but sTSH is also elevated: consider TSH-secreting pituitary adenoma or thyroid hormone resistance syndrome
Imaging:
- Radioactive iodine uptake (RAIU) scan with ¹²³I: differentiates Graves' (diffuse uptake) from toxic nodule/TMNG (focal/patchy uptake) vs. thyroiditis (low uptake)
- Factitious thyrotoxicosis: markedly suppressed uptake
Treatment
Three Main Objectives:
- Ameliorate acute symptoms
- Suppress synthesis and secretion of thyroid hormones
- Treat the primary cause to prevent recurrence
1. Symptomatic Control (All Causes)
- Beta-blockers (propranolol, metoprolol, atenolol): first-line for controlling sympathetically mediated symptoms - tachycardia, hypertension, tremor, anxiety. Continue until FT4 normalises.
- Calcium channel blockers: alternative for patients who cannot tolerate beta-blockers.
2. Antithyroid Drugs (ATDs)
| Drug | Mechanism | Key Notes |
|---|---|---|
| Methimazole (MMI) | Blocks thyroid peroxidase; inhibits hormone synthesis | Preferred drug in most patients; euthyroid state in 3-8 weeks |
| Propylthiouracil (PTU) | Inhibits synthesis + inhibits peripheral T4→T3 conversion | Preferred in first trimester of pregnancy (MMI teratogenic); used in thyroid storm; risk of serious hepatotoxicity |
- PTU is generally avoided in non-pregnant adults except in thyroid storm or first trimester pregnancy due to serious liver injury risk.
- Graves' disease may go into remission after 12-18 months of ATDs in some patients.
3. Radioactive Iodine (¹³¹I)
- Treatment of choice for toxic multinodular goitre and toxic adenoma.
- Option for Graves' disease in appropriate patients.
- Absolutely contraindicated in pregnancy or when pregnancy is possible.
- May take several months to destroy overactive tissue.
- Risk of post-treatment hypothyroidism requiring monitoring of sTSH.
- Caution: Thyroid storm may paradoxically occur following RAI if ATDs were withdrawn beforehand.
4. Surgery (Thyroidectomy)
- For large goitres requiring cosmetic improvement.
- Severe hyperthyroidism requiring more immediate effect.
- Patients who fail/cannot tolerate ATDs or RAI.
- Requires pre-operative euthyroid state; iodide given pre-operatively to reduce thyroid vascularity.
Thyroid Storm (Thyrotoxic Crisis)
Thyroid storm is a life-threatening exacerbation of thyrotoxicosis. Mortality is 10-75%.
Precipitants
- Infection, trauma, general surgery
- Myocardial infarction, pulmonary embolism, CVA
- DKA, hyperosmolar coma
- Radioactive iodine therapy, withdrawal of antithyroid medication
- Iodine administration, ingestion of thyroid hormone
- Labor and delivery, eclampsia
- Unknown in up to 25% of cases
Clinical Features of Thyroid Storm
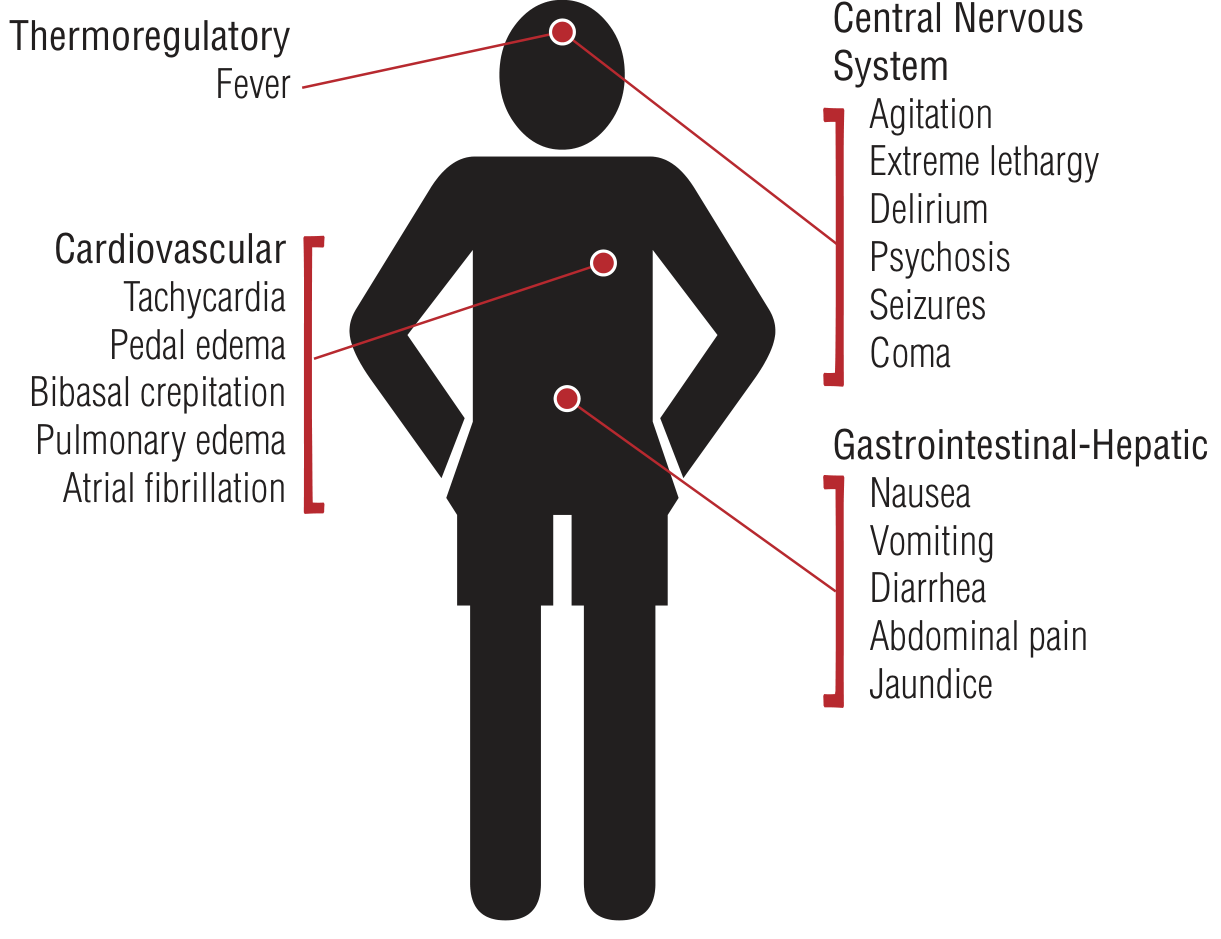
Key additional features beyond uncomplicated hyperthyroidism:
- Fever (may herald onset; key distinguishing feature)
- CNS: agitation → delirium/psychosis → seizures/coma
- Cardiovascular: AF in 10-35%, high-output cardiac failure, widened pulse pressure
- GI-Hepatic: nausea, vomiting, diarrhea, abdominal pain, jaundice
- Sinus tachycardia in ~40% of cases
Burch-Wartofsky Point Scale (BWPS)
Score ≥45 = thyroid storm likely; 25-44 = impending storm. Based on:
- Thermoregulatory dysfunction (temp 37.2°C = 5 pts → ≥40°C = 30 pts)
- CNS effects (absent=0, mild agitation=10, delirium/psychosis=20, seizures/coma=30)
- GI-hepatic dysfunction (0-20 pts)
- Cardiovascular (heart rate, heart failure, AF)
- Precipitating event (present = 10 pts)
Treat upon clinical suspicion - do not wait for lab confirmation.
Treatment of Thyroid Storm (in order)
| Step | Goal | Agent |
|---|---|---|
| 1 | Supportive care | IV fluids (isotonic saline ± dextrose), cooling |
| 2 | Inhibit peripheral adrenergic effects | Beta-blockers (propranolol IV/PO; metoprolol/atenolol) |
| 3 | Inhibit NEW thyroid hormone synthesis | Thionamide FIRST (PTU preferred in storm due to T4→T3 block; high doses) |
| 4 | Inhibit thyroid hormone release | Iodide (Wolff-Chaikoff) - given AFTER thionamide (1+ hour delay to prevent iodine substrate for new synthesis) |
| 5 | Block peripheral T4→T3 conversion | PTU, corticosteroids (hydrocortisone/dexamethasone), propranolol |
| 6 | Reduce free hormone reabsorption | Cholestyramine (interrupts enterohepatic recirculation) |
| 7 | Treat the precipitant | Antibiotics, surgery, etc. |
| 8 | Definitive care | Plan RAI or surgery once stable |
Critical order rule: Always give thionamide BEFORE iodide. Giving iodide first provides substrate for new hormone synthesis and can worsen storm.
Corticosteroids serve a dual purpose: reduce T4→T3 conversion AND cover for possible coincidental adrenal insufficiency (low cortisol in thyroid storm should raise suspicion for this).
Special Populations
Pregnancy
- Preferred ATD: PTU in first trimester (methimazole is teratogenic - associated with aplasia cutis and choanal/oesophageal atresia)
- Switch to MMI after first trimester (PTU hepatotoxicity risk)
- ¹³¹I: absolutely contraindicated
- Thyroid storm in pregnancy: manage same drugs (beta-blockers, PTU, iodide, corticosteroids); avoid aspirin (displaces T4 from binding proteins, worsening thyrotoxicosis)
- High TSI titers in Graves' disease are associated with fetal/neonatal hyperthyroidism
Elderly
- Blunted adrenergic symptoms; cardiovascular and weakness predominate
- Higher risk of AF
- "Apathetic hyperthyroidism" more common
Cardiovascular Complications
- Mild hypercalcaemia (<12 mg/dL) frequently accompanies thyrotoxicosis due to increased bone turnover; responds rapidly to beta-blockers, resolves with euthyroid state
- High-output heart failure: increased cardiac output, stroke volume, contractility; decreased peripheral resistance
- AF: 10-35% in thyroid storm; up to 15% in elderly with uncomplicated disease
- Increased risk of ischemic CHF in patients with pre-existing CAD
Recent Evidence (2024-2026)
A 2024 systematic review on perioperative thyrotoxicosis management (PMID 39722810) addresses approaches when standard therapy is contraindicated or fails - relevant for surgical patients. A 2026 systematic review noted autoimmune thyroid diseases after COVID-19 infection (PMID 42354220), including new-onset thyrotoxicosis/Graves' disease as a post-COVID sequela.
Sources:
- Textbook of Family Medicine 9e (pp. 1019-1022)
- Tintinalli's Emergency Medicine - Comprehensive Study (Ch. 229)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Ch. 61)
- Tietz Textbook of Laboratory Medicine, 7th Ed.
- Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.