
Answer
Reading File
Finding Sources
Finding Sources
Searching Images
massive pleural effusion chest X-ray opacification
Finding Sources
Finding Sources
Reading File
Now I have enough information to give a thorough analysis.
Chest X-Ray Analysis — PA View
Patient: Opsing Kokani, 69Y | Civil Hospital, Nandurbar | Date: 10-Feb-25
Key Radiological Findings
1. Massive Left-Sided Pleural Effusion
The entire left lower hemithorax shows dense, near-homogeneous opacification obliterating:
- The left costophrenic angle
- The left hemidiaphragm
- The left cardiac border (silhouette sign)
The opacity has a concave superior meniscus, higher laterally — classic for free pleural fluid. Given the extent reaching well above the 4th anterior rib level, this is a massive effusion (>1000 mL).
2. Contralateral (Rightward) Mediastinal Shift
The cardiac silhouette is displaced to the right, with tracheal deviation right. This is the expected mass effect of a large free effusion pushing mediastinal contents away. — Grainger & Allison's Diagnostic Radiology
Clinical note: If mediastinal shift were absent despite this large an effusion, it would strongly raise concern for ipsilateral obstructive collapse or extensive pleural malignancy (mesothelioma/metastatic carcinoma).
3. Right Lung
Largely aerated with preserved lung markings. No gross opacities or pneumothorax on the right.
4. Upper Zones Bilaterally
Increased interstitial markings, possible cardiomegaly beneath the effusion — difficult to assess fully given the displacement.
5. Bony Structures
No obvious rib fractures visible.
Differential Diagnosis — Cause of Massive Pleural Effusion
In a 69-year-old, the leading causes include:
| Cause | Clues to look for |
|---|---|
| Malignancy (lung, breast, lymphoma, mesothelioma) | Most common at this age; exudate on thoracentesis |
| Congestive Heart Failure | Bilateral effusions typical; transudative; JVD, peripheral edema |
| Parapneumonic / Empyema | Fever, leukocytosis; exudate; loculations on US |
| Tuberculosis | Common in India; lymphocytic exudate; ADA elevated |
| Hepatic hydrothorax / Cirrhosis | Ascites, liver disease; transudate |
| Hemothorax | Trauma or iatrogenic history |
| Post-cardiac injury / Dressler's | History of MI or cardiac surgery |
Given the geographic context (Nandurbar, Maharashtra — a region with high TB burden), tuberculous pleural effusion is high on the differential in this patient.
Immediate Management
- Ultrasound-guided thoracentesis — both diagnostic and therapeutic
- Send fluid for: LDH, protein, glucose, cell count & differential, cytology, Gram stain, culture & sensitivity, ADA (for TB)
- Apply Light's criteria to classify transudate vs exudate
- CT chest — to assess underlying lung parenchyma (mass, collapse, lymphadenopathy) once some fluid is drained
- Blood tests — CBC, LFT, RFT, LDH, albumin, ESR, sputum AFB if TB suspected
- Large-volume therapeutic drainage if patient is dyspnoeic (up to 1–1.5 L at a time to avoid re-expansion pulmonary edema)
Reference Images for Comparison
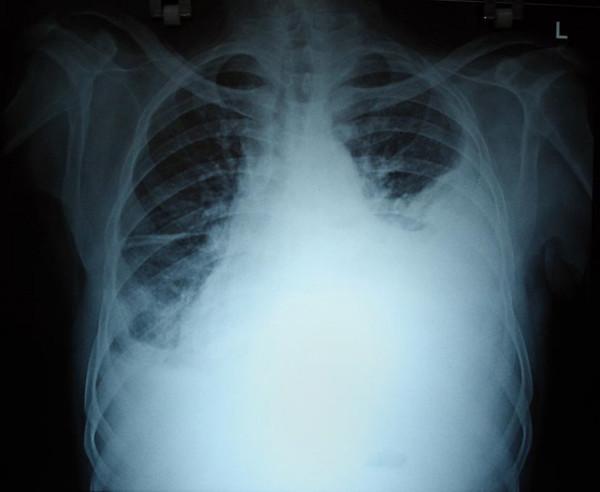
Reference: Massive left pleural effusion showing meniscus sign, obliteration of left hemidiaphragm and cardiac border, with rightward mediastinal shift — pattern identical to the presented film.
Summary: This 69-year-old patient has a massive left pleural effusion with contralateral mediastinal shift. Urgent ultrasound-guided thoracentesis is indicated for diagnosis and symptom relief. In this clinical setting, TB, malignancy, and cardiac failure are the top diagnostic considerations. — Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.