Treatment of SVT
Reading File
Finding Sources
Searching PubMed
"supraventricular tachycardia" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer. Let me synthesize it.
Treatment of Supraventricular Tachycardia (SVT)
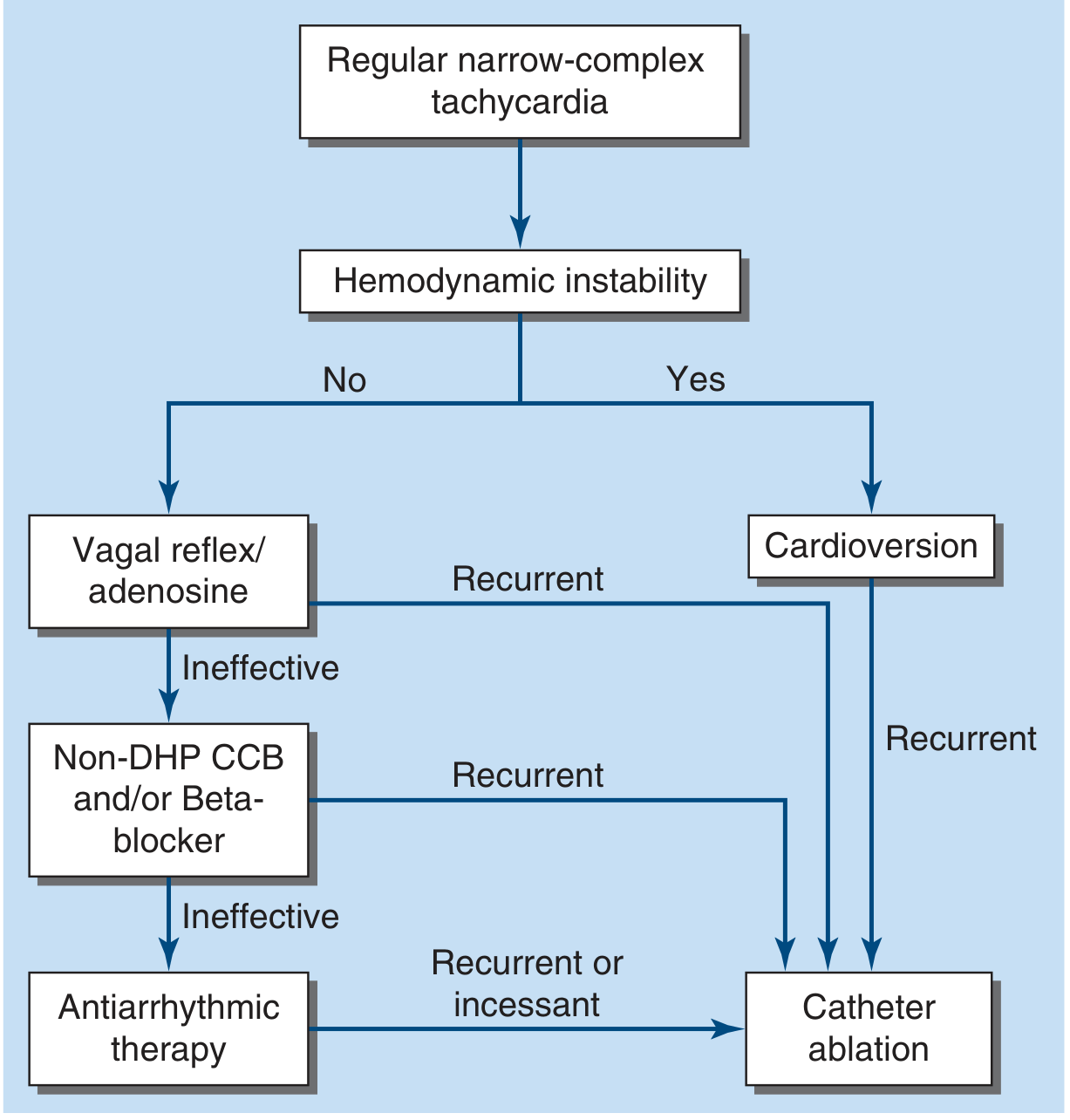
SVT encompasses several distinct arrhythmias — most commonly AVNRT (AV nodal reentrant tachycardia), AVRT (AV reentrant tachycardia, including WPW), and focal atrial tachycardia — all arising above or within the AV node. Treatment is stratified by hemodynamic stability and the underlying mechanism.
Step 1: Assess Hemodynamic Stability
| Status | Action |
|---|---|
| Unstable (hypotension, altered consciousness, respiratory distress) | Immediate synchronized DC cardioversion |
| Stable | Sequential pharmacologic approach below |
Step 2: Stable Patient — Acute Termination
1. Vagal Maneuvers (first-line)
Most PSVTs depend on AV nodal conduction and respond to vagotonic stimulation.
- Modified Valsalva (preferred): Patient semi-recumbent at 45°, exhales against closed glottis for 10–15 s, then immediately repositioned supine with passive leg raise at 45° for 15 s. Higher success rate than standard Valsalva.
- Standard Valsalva: Supine, forced exhalation against closed glottis for 10–15 s.
- Carotid sinus massage: Steady pressure for 5–10 s at one carotid sinus; avoid in patients with prior stroke (within 3 months), carotid stenosis/bruit, or history of ventricular arrhythmia.
- Cold stimulus (especially in children/infants): Ice pack/ice-water washcloth to forehead or bridge of nose for ≤30 s.
2. Adenosine (first-line if vagal maneuvers fail)
"Intravenous adenosine will terminate the vast majority of PSVT episodes by transiently blocking conduction in the AV node." — Harrison's Principles of Internal Medicine, 22e
- Dose: 6 mg IV rapid bolus with rapid NS flush → if no conversion, 12 mg IV; may repeat 12 mg once
- Mechanism: Slows AV nodal conduction; interrupts reentry pathways
- Side effects: Transient chest pain, dyspnea, anxiety, flushing; may precipitate AF in up to 15%
- Contraindications/Cautions:
- Contraindicated in prior cardiac transplantation (hypersensitivity due to surgical sympathetic denervation)
- Use cautiously in WPW (adenosine-induced AF can cause hemodynamic instability)
- Caution in asthma (can aggravate bronchospasm)
If adenosine converts the rhythm → probable re-entry SVT. Observe for recurrence.
3. If Adenosine Ineffective: Non-DHP CCB or Beta-Blocker
IV verapamil, diltiazem, or esmolol are second-line options — effective but carry a risk of hypotension and have longer duration of action. These can also be given orally for outpatient "pill-in-pocket" use (patient takes at onset of episode, combined with Valsalva).
4. If No Conversion (atrial flutter, ectopic AT, junctional tachycardia suspected)
- Rate control: calcium channel blockers or beta-blockers (use beta-blockers cautiously in pulmonary disease or CHF)
- Treat underlying cause
- Consider expert consultation
SVT Subtypes and Special Situations
AVNRT (most common in adults)
Treated with vagal maneuvers → adenosine → CCB/beta-blocker. Patients with frequent recurrences are candidates for prophylaxis (beta-blocker or CCB) or catheter ablation.
AVRT / WPW Syndrome
- Orthodromic AVRT (narrow complex): Treated the same as AVNRT — vagal maneuvers → adenosine → CCB/beta-blocker.
- Antidromic AVRT (wide complex): Wide QRS, potentially very rapid (≥200 bpm). Treat as VT unless diagnosis is certain.
- Pre-excited AF + WPW: Avoid AV nodal blockers (adenosine, digoxin, verapamil) — they can precipitate lethal arrhythmias by accelerating conduction through the accessory pathway. Use cardioversion or IV procainamide/ibutilide.
- Definitive treatment: Radiofrequency catheter ablation (~95% efficacy).
Wide-Complex SVT (SVT with Aberrancy)
- Treat as VT until proven otherwise.
- If the rhythm is regular and the patient is stable, a trial of IV adenosine is reasonable.
- Very irregular wide-complex tachycardia = likely preexcited AF → cardioversion or IV procainamide/ibutilide.
Junctional Tachycardia
- Address underlying cause (structural heart disease, metabolic disturbance, drug toxicity).
- Trial of nodal blockade (CCB or beta-blocker) if rate is deleterious.
Pediatric SVT
- Vagal maneuvers first (e.g., ice to face, blowing into a syringe)
- Adenosine 6 mg IV → 12 mg IV if no conversion
- If unstable: synchronized cardioversion 0.5 J/kg (up to 1 J/kg)
- Always consult Cardiology
Long-Term / Recurrence Management
| Option | Indication |
|---|---|
| Beta-blocker or non-DHP CCB (daily or "pill-in-pocket") | Frequent, symptomatic recurrences |
| Flecainide, propafenone | Refractory cases without structural heart disease (avoid in WPW) |
| Catheter ablation | Recurrent PSVT; drug-intolerant; desired by patient; WPW with high-risk pathway. Success ~95% |
Key Drug Contraindications Summary
| Drug | Avoid in |
|---|---|
| Verapamil, Digoxin | WPW with pre-excitation / antidromic AVRT |
| Flecainide | WPW syndrome |
| Adenosine | Cardiac transplant; caution in asthma, WPW |
| Beta-blockers | Severe asthma, decompensated HF (relative) |
Sources: Harrison's Principles of Internal Medicine 22e; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Washington Manual of Medical Therapeutics; Harriet Lane Handbook 23e.
Treatment
Asking for Preferences
The previous response already covers SVT treatment comprehensively. Here's a concise summary of what was covered:
SVT Treatment — Quick Reference
Unstable Patient
→ Immediate synchronized DC cardioversion
Stable Patient — Sequential Approach
Step 1 — Vagal maneuvers
- Modified Valsalva (best success rate)
- Standard Valsalva, carotid sinus massage, cold stimulus (face)
Step 2 — Adenosine IV (if vagal maneuvers fail)
- 6 mg rapid IV bolus → 12 mg → repeat 12 mg once
- Terminates the vast majority of PSVT
Step 3 — Non-DHP CCB or Beta-blocker (if adenosine fails)
- IV verapamil, diltiazem, or esmolol
Step 4 — Cardioversion (refractory or unstable)
Long-Term / Recurrence
- Beta-blocker or CCB — daily prophylaxis or pill-in-pocket
- Catheter ablation — first-line for recurrent/refractory SVT (~95% success)
Critical Caveats
- WPW + pre-excited AF: avoid adenosine, verapamil, digoxin → use cardioversion or IV procainamide
- Wide-complex tachycardia: treat as VT until proven otherwise
- Pediatric: vagal maneuvers → adenosine → cardioversion 0.5–1 J/kg
Is there a specific aspect of SVT treatment you'd like me to expand on (e.g., a specific drug, ablation, pediatric dosing, WPW management)?
Dose
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Here are the doses for all SVT drugs, organized by line of treatment:
Drug Doses for SVT Treatment
First-Line: Adenosine (IV)
| Step | Adult Dose | Pediatric Dose |
|---|---|---|
| Initial | 6 mg rapid IV bolus | 0.1 mg/kg (max 6 mg) |
| 2nd dose (if no conversion in 1–2 min) | 12 mg rapid IV bolus | 0.2 mg/kg (max 12 mg) |
| 3rd dose (repeat if needed) | 12 mg rapid IV bolus | — |
Administration: Rapid push over 1–2 seconds via peripheral IV, followed immediately by 20 mL NS flush. Patients typically experience transient asystole (<5 sec).
Dose adjustments:
- Reduce to 3 mg initial dose in: cardiac transplant patients, patients on dipyridamole or carbamazepine, central line administration
- Higher doses may be needed in patients on caffeine or theophylline
Second-Line: Non-DHP Calcium Channel Blockers (IV)
| Drug | Dose | Notes |
|---|---|---|
| Verapamil | Up to 10 mg IV over 1–2 min; may repeat equal dose in 30 min. Continuous infusion: 0.005 mg/kg/min | Monitor BP and rhythm. Terminates 60–90% of PSVT. Contraindicated in WPW + pre-excited AF |
| Diltiazem | 0.25 mg/kg IV bolus over 2 min; second dose in 15 min if needed | Generally better tolerated (less hypotension) than verapamil |
Oral (maintenance/prevention): Verapamil 240–480 mg/day in divided doses; Diltiazem 120–360 mg/day.
Second-Line: Beta-Blockers (IV)
| Drug | Dose | Notes |
|---|---|---|
| Esmolol | Loading: 500 mcg/kg IV over 1 min; Maintenance: 50–200 mcg/kg/min infusion | Short-acting (half-life ~9 min), titratable; preferred when transient effect is desired |
| Propranolol | 1–3 mg/dose IV slow push; may repeat every 2–5 min up to 5 mg total | Non-selective; avoid in asthma |
| Metoprolol | 2.5–5 mg IV bolus over 2 min; up to 3 doses | Cardioselective |
Unstable Patient: Synchronized Cardioversion
| Patient | Energy |
|---|---|
| Adult | 50–100 J (biphasic); escalate as needed |
| Pediatric | 0.5 J/kg (up to 1 J/kg) |
WPW + Pre-excited AF (AV nodal blockers contraindicated)
| Drug | Dose |
|---|---|
| Procainamide (preferred) | 15–18 mg/kg IV at 25–50 mg/min |
| Ibutilide | 1 mg IV over 10 min; may repeat once |
| Amiodarone | 150 mg IV over 10 min if unstable/polymorphic VT |
Sources: Tintinalli's Emergency Medicine; Braunwald's Heart Disease; Harrison's Principles of Internal Medicine 22e; Rosen's Emergency Medicine.
SVT ECG changes
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.