Write a short note on upper lip bite test for my MD Anaesthesiology exam notes
Reading File
Finding Sources
Searching the Web
upper lip bite test airway assessment anaesthesia classification
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have everything needed for a thorough, exam-ready note. Here it is:
Upper Lip Bite Test (ULBT)
Definition and Background
The Upper Lip Bite Test (ULBT) is a simple bedside preoperative airway assessment tool introduced by Khan et al. (2003). It evaluates anterior mandibular mobility (jaw subluxation) by assessing the ability of the lower incisors to cover the upper lip. It is considered a more practical and arguably more accurate alternative to the modified Mallampati classification (MMC) for predicting difficult laryngoscopy and intubation.
How to Perform
The patient is asked to protrude the lower jaw and bite the upper lip with the lower incisors as far as possible. The patient sits upright; no special positioning is required. The result is graded based on how far the lower incisors can reach.
Classification
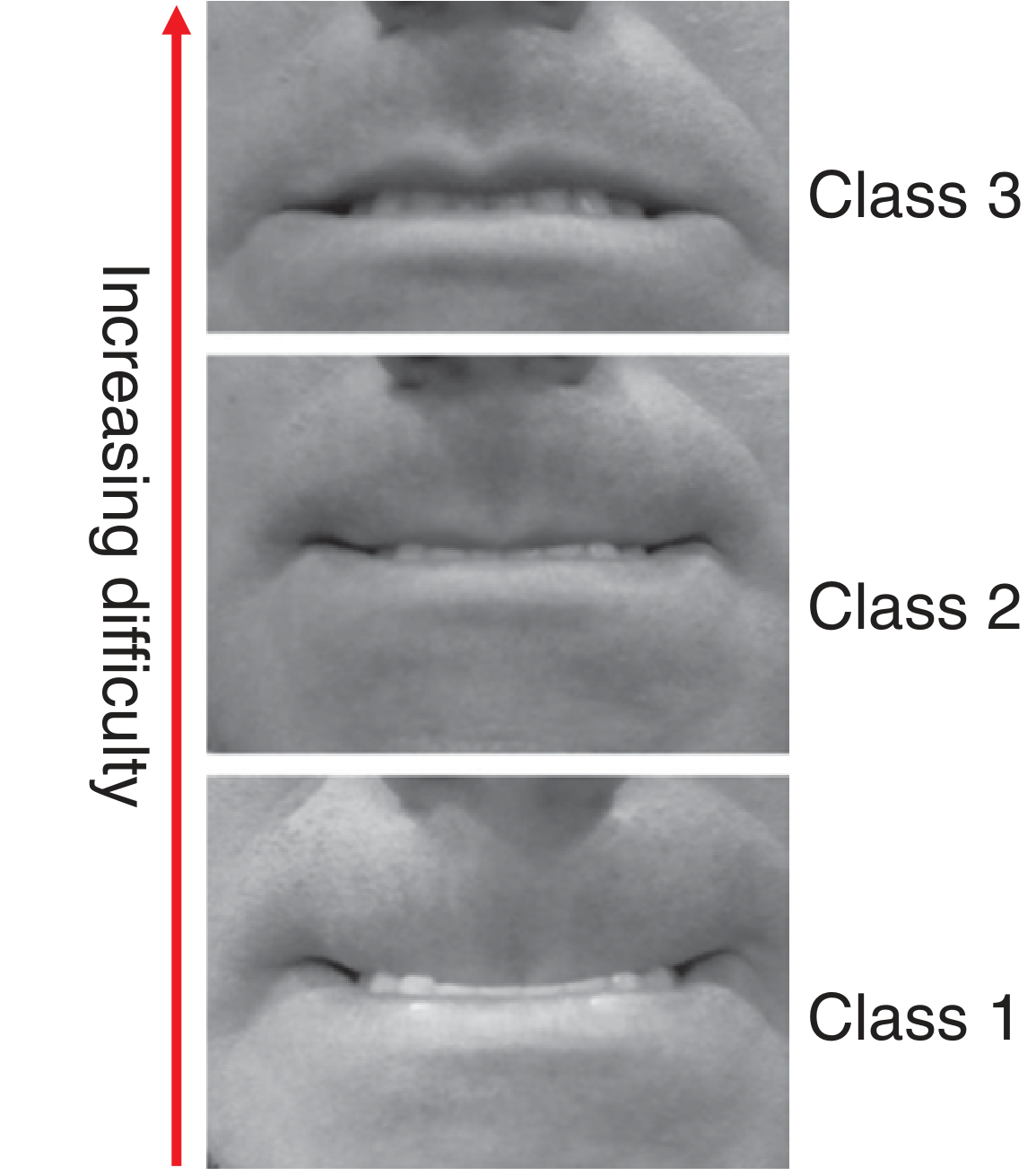
Figure: Upper Lip Bite Test classes showing increasing difficulty from Class 1 (bottom) to Class 3 (top). - Fishman's Pulmonary Diseases and Disorders, Fig. 145-4
| Class | Finding | Implication |
|---|---|---|
| Class I | Lower incisors can bite above the vermilion border of the upper lip (mucosa covered) | Normal jaw protrusion - easy intubation likely |
| Class II | Lower incisors can bite only at the vermilion border (partial coverage) | Intermediate - mild concern |
| Class III | Lower incisors cannot bite the upper lip at all | Poor jaw protrusion - difficult intubation predicted |
Classes II and III are considered predictors of a difficult airway.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 571
- Fishman's Pulmonary Diseases and Disorders, p. 2576-2577
What It Assesses
The ULBT is fundamentally a test of:
- Temporomandibular joint mobility
- Anterior mandibular protrusion (jaw subluxation ability)
- Adequacy of the lower jaw to facilitate laryngoscopy
It correlates with the ability to align the oral and pharyngeal axes during laryngoscopy. Poor protrusion means the lower jaw cannot move forward to create the space needed for laryngoscope blade insertion.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 114
Diagnostic Performance
From pooled data (Barash Clinical Anesthesia, 9e, Table 28-6):
| Test | Sensitivity (%) | Specificity (%) |
|---|---|---|
| Mouth opening | 22 | 94 |
| Mallampati classification | 53 | 80 |
| Thyromental distance | 37 | 89 |
| Sternomental distance | 33 | 92 |
| Upper Lip Bite Test | 67 | 92 |
Key points:
- The ULBT has the highest sensitivity (67%) among common airway tests.
- Specificity is ~92-96% (relatively high - a positive test strongly suggests difficulty).
- In one prospective study, 60% of Class III patients had a difficult airway.
- Positive predictive value (PPV) remains low in isolation - most patients predicted difficult are in fact normal.
- The combination of abnormal ULBT + other abnormal tests greatly increases the probability of a truly difficult airway.
Advantages Over Mallampati
| Feature | ULBT | Mallampati |
|---|---|---|
| Patient cooperation | Minimal | Requires mouth opening + tongue protrusion |
| Observer variability | Less | More (lighting, phonation, etc.) |
| Sensitivity | Higher (67%) | Lower (53%) |
| Specificity | Higher (92%) | Lower (80%) |
| Assesses | Jaw mobility | Pharyngeal space |
| Edentulous patients | Not applicable | May be assessed |
Limitations
-
Cannot be used in edentulous patients (no lower incisors)
-
Cannot be assessed in patients with limited mouth opening from the start
-
Poor predictor as a single screening test - should always be combined with other assessments (Mallampati, thyromental distance, neck mobility, inter-incisor distance, sternomental distance)
-
Like all airway tests, no single test is 100% sensitive or specific - most difficult airways remain unanticipated
-
Limited utility in emergency settings where full cooperation may not be possible
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, p. prediction of difficulty section
Clinical Relevance for Anaesthesia
- Part of the standard preoperative airway assessment battery
- A Class III result should prompt:
- Senior anaesthetist involvement
- Awake fibreoptic intubation (AFOI) consideration
- Video laryngoscopy preparation
- Difficult airway trolley readiness
- Plan A/B/C airway strategy documentation
- Useful in patients where the Mallampati is difficult to elicit (reduced cooperation, limited neck extension)
- Often combined with Mallampati in a multivariate scoring system for better predictive accuracy
Summary Box (High-Yield for MCQ)
- Introduced by: Khan et al., 2003
- Tests: Anterior mandibular protrusion / TMJ mobility
- Class III = difficult intubation (cannot bite upper lip)
- Best sensitivity among common airway tests: 67%
- High specificity: ~92-96%
- Cannot use in edentulous patients
- Better than Mallampati in sensitivity and specificity
- Grades II and III = difficult airway predictors
This is a shared conversation. Sign in to Orris to start your own chat.