Bi Red2 lesions fbrodenptic change
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information to provide a thorough answer on BI-RADS 2 lesions and fibrocystic change.
BI-RADS 2 Lesions & Fibrocystic Change
BI-RADS (Breast Imaging Reporting and Data System)
The ACR BI-RADS system standardizes mammographic reporting and management recommendations. The full classification:
| Category | Definition | Management |
|---|---|---|
| 0 | Incomplete — needs additional imaging | Additional views / US / MRI |
| 1 | Negative (0% malignancy) | Annual screening |
| 2 | Benign finding (0% malignancy) | Annual screening |
| 3 | Probably benign (<2% malignancy) | Short-interval follow-up (6 months) |
| 4a | Suspicious (2–10% malignancy) | Biopsy |
| 4b | Suspicious (10–50% malignancy) | Biopsy |
| 4c | Suspicious (50–95% malignancy) | Biopsy |
| 5 | Highly suggestive of malignancy (>95%) | Biopsy |
| 6 | Known biopsy-proven malignancy | As indicated |
Source: ACR BI-RADS Atlas, 5th ed., adapted in Sabiston Textbook of Surgery
BI-RADS 2 — Key Points
- Assigned to definitively benign findings identified on mammography, ultrasound, or MRI
- 0% risk of malignancy — no further workup required
- Patient returns to routine annual screening
- Examples of BI-RADS 2 findings include:
- Simple cysts (completely anechoic on US)
- Intramammary lymph nodes
- Fat-containing lesions (lipoma, oil cyst, hamartoma)
- Calcified fibroadenoma
- Fibrocystic changes (when confidently benign in appearance)
- Stable calcifications on serial imaging
Fibrocystic Change (Nonproliferative Breast Changes)
Fibrocystic change is the most common benign breast condition, typically affecting women aged 30–50 years, peaking in the perimenopausal period.
Pathophysiology
An exaggerated stromal and epithelial response to circulating hormones (estrogen, progesterone) and growth factors drives the changes. The term "nonproliferative" historically implied no increased cancer risk, though some subtypes involve clonal proliferation.
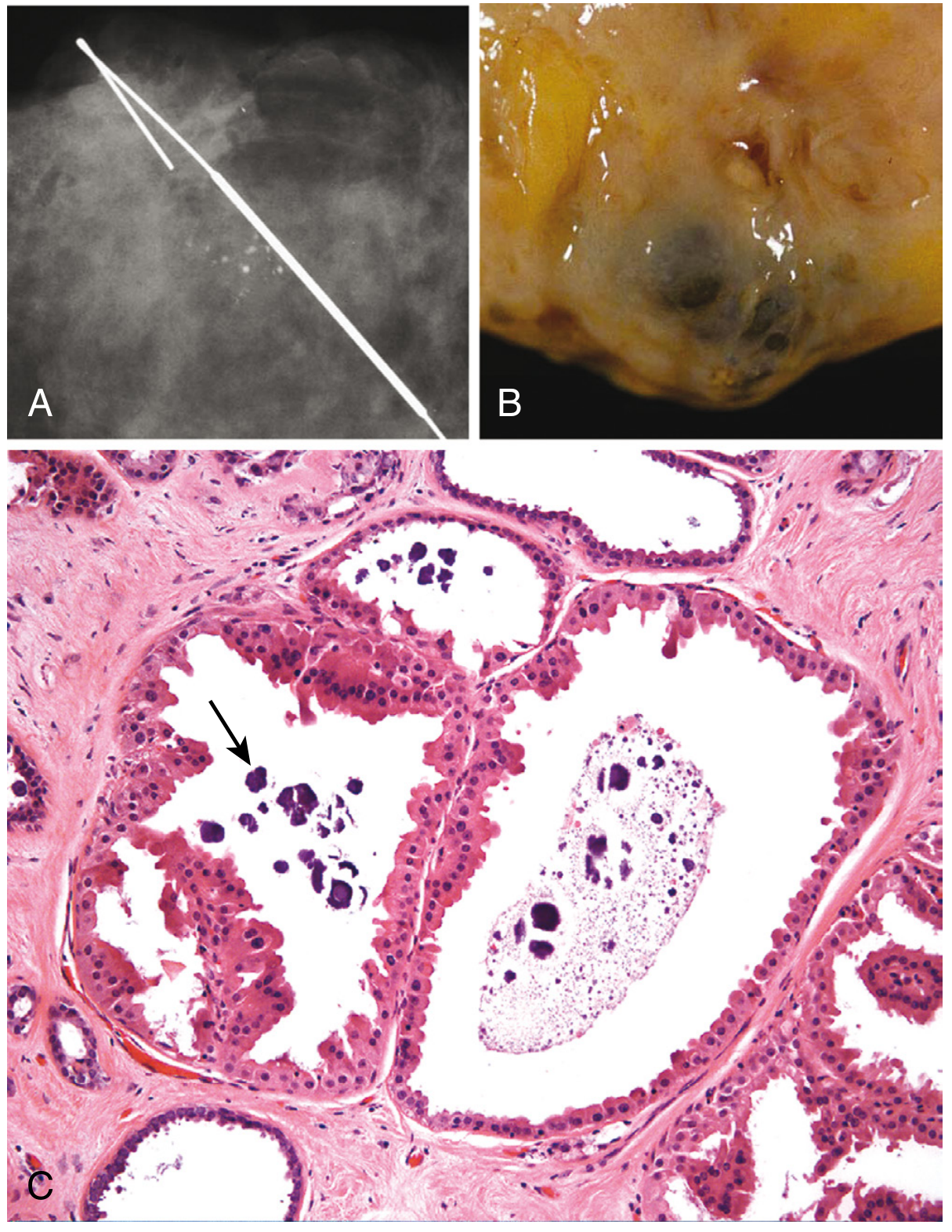
Three Principal Morphologic Features
-
Cystic change (with or without apocrine metaplasia)
- Small lobular cysts coalesce into larger macrocysts
- Classic "blue-dome cysts" — turbid, blue-brown fluid
- Lined by flattened or apocrine metaplastic epithelium
- Calcifications are common (clustered, rounded)
-
Fibrosis
- Cyst rupture releases contents → chronic inflammation → stromal fibrosis
- Produces the palpable nodularity characteristic of the condition
-
Adenosis
- Increased number of acini per lobule
- Lined by columnar epithelial cells
- Occasional intraluminal calcifications
Clinical Presentation
- Cyclic mastalgia — premenstrual breast pain and tenderness (most common symptom)
- Diffuse or focal nodularity on exam
- Palpable mass possible (dominant cyst)
- Breast pain is not a typical breast cancer symptom — occurs in only ~7% of breast cancers
Imaging Appearance
- Mammography: diffuse or focal radiologic density
- Ultrasound: multiple small anechoic cysts; palpable cysts confirmed as simple cysts → BI-RADS 2
- Complex cysts (with solid intracystic components) require further evaluation (core needle biopsy)
Histologic Solid Elements
In addition to macro/microcysts, fibrocystic changes may include:
- Adenosis
- Sclerosis
- Apocrine metaplasia
- Stromal fibrosis
- Epithelial metaplasia and hyperplasia
Management
- Simple cyst confirmed by US: no further evaluation required if asymptomatic → BI-RADS 2, routine screening
- Symptomatic cysts: needle aspiration (if fluid non-bloody and cyst resolves, no cytology needed)
- Recurrent cysts (>2 aspirations): core needle biopsy to evaluate solid elements
- Mastalgia: Danazol, Lupron, or tamoxifen (significant side effects); nonsteroidal anti-inflammatory drugs; scapulothoracic bursa injection if pain is referred
- Women ≥30 with noncyclic mastalgia: mammography + US in addition to exam
Cancer Risk Stratification
Fibrocystic change spans a spectrum:
| Type | Relative Risk of Breast Cancer |
|---|---|
| Nonproliferative (cysts, apocrine metaplasia, adenosis, mild hyperplasia) | No increased risk |
| Proliferative without atypia (moderate/florid hyperplasia, sclerosing adenosis) | ~1.5–2× increased risk |
| Proliferative with atypia (ADH, ALH) | ~4–5× increased risk |
In summary: A BI-RADS 2 designation for fibrocystic change on imaging (simple cysts, benign calcifications, nodularity) means the finding is definitively benign, requires no biopsy or short-interval follow-up, and the patient returns to routine annual mammographic screening. — Sabiston Textbook of Surgery; Robbins, Cotran & Kumar Pathologic Basis of Disease; Current Surgical Therapy 14e
Danazol tab use in patient
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.