fibrous dysplasia of maxilla
Reading File
Finding Sources
Searching PubMed
"fibrous dysplasia" AND maxilla
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive summary of fibrous dysplasia of the maxilla drawn from multiple authoritative textbooks:
Fibrous Dysplasia of the Maxilla
Definition and Background
Fibrous dysplasia (FD) is a benign, slowly progressive developmental anomaly of bone-forming mesenchyme - not a true neoplasm - in which normal cancellous bone is replaced by a fibrous stroma containing immature woven bone. It results from a defect in osteoblastic differentiation and maturation. The maxilla is one of the most frequently involved bones in the craniofacial skeleton.
- Cummings Otolaryngology; Scott-Brown's Otorhinolaryngology
Molecular Pathogenesis
All forms arise from somatic gain-of-function mutations in GNAS1 (chromosome 20q13), which encodes the alpha subunit of the stimulatory G-protein (Gs-alpha). The constitutively active Gs-protein elevates intracellular cAMP, promoting cellular proliferation while disrupting osteoblast differentiation. The phenotype depends on when in embryogenesis the mutation is acquired and what proportion of mesenchymal cells carry it.
- Robbins & Kumar Basic Pathology
Classification
| Form | Frequency | Craniofacial Involvement |
|---|---|---|
| Monostotic | ~80% | Maxilla and mandible most commonly affected (up to 25% of cases) |
| Polyostotic | ~20% | Craniofacial involvement in 40-50% of cases |
| McCune-Albright syndrome | ~5% | Polyostotic FD + café-au-lait spots + endocrine hyperfunction |
| Mazabraud syndrome | Rare | FD + soft tissue myxoma |
The maxilla is the most commonly affected craniofacial bone in monostotic disease. Importantly, unlike FD in long bones (which does not cross joint lines), craniofacial FD can cross bony sutures - involvement of multiple facial bones is still classified as monostotic craniofacial fibrous dysplasia, not polyostotic.
- Scott-Brown's Otorhinolaryngology; Harrison's Principles of Internal Medicine 22E
Clinical Features
- Age of onset: First two decades; monostotic form may become quiescent at puberty, polyostotic form can progress into adulthood (and with pregnancy or estrogen therapy)
- Sex: Equal frequency in monostotic form; McCune-Albright is 10:1 female predominance
- Presentation in the maxilla:
- Painless facial swelling and asymmetry
- Expansion causing nasal obstruction, altered dentition
- Interference with maxillary sinus drainage - pressure/pain
- Aesthetic deformity ("leontiasis ossea" in severe polyostotic involvement)
- Rarely: cranial nerve compression (optic nerve, trigeminal branches)
- Monostotic cases are often incidentally discovered; polyostotic forms present earlier with bone pain and deformity
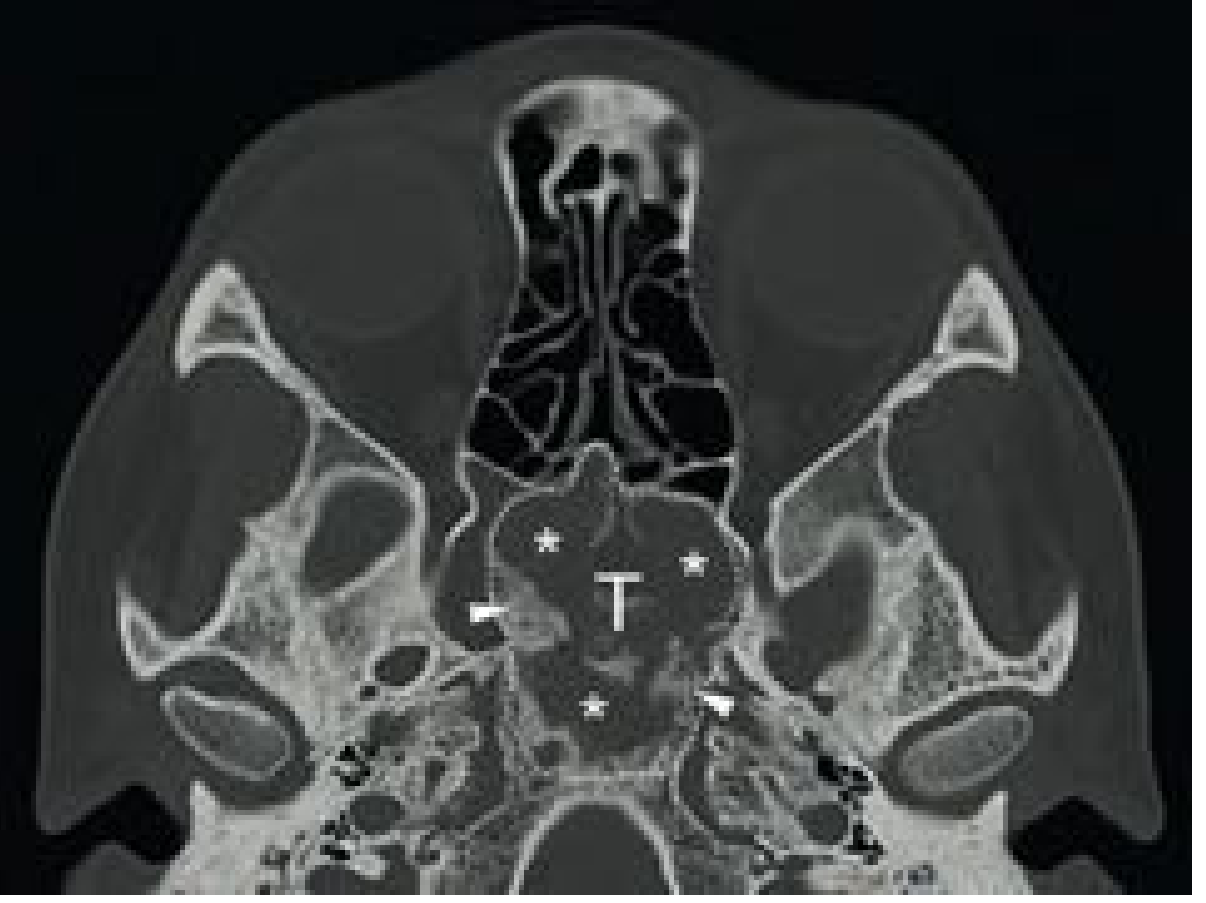
Radiology
Plain X-ray / CT (hallmark): The appearance depends on the degree of mineralization:
- Early phase (high fibrous density): Radiolucent/lytic appearance
- Mixed phase: Classic "ground-glass" appearance - hazy, homogeneous density from irregularly arranged woven bone spicules (most typical)
- Late/sclerotic phase: Dense "cotton-wool" areas
On CT: expansile lesion with intact cortex, well-defined margins, no periosteal reaction.
MRI:
- T1: intermediate signal (hypointense where sclerotic)
- T2: hypointense (distinguishes it from other lesions like bone cysts)
- May show non-homogeneous enhancement with gadolinium
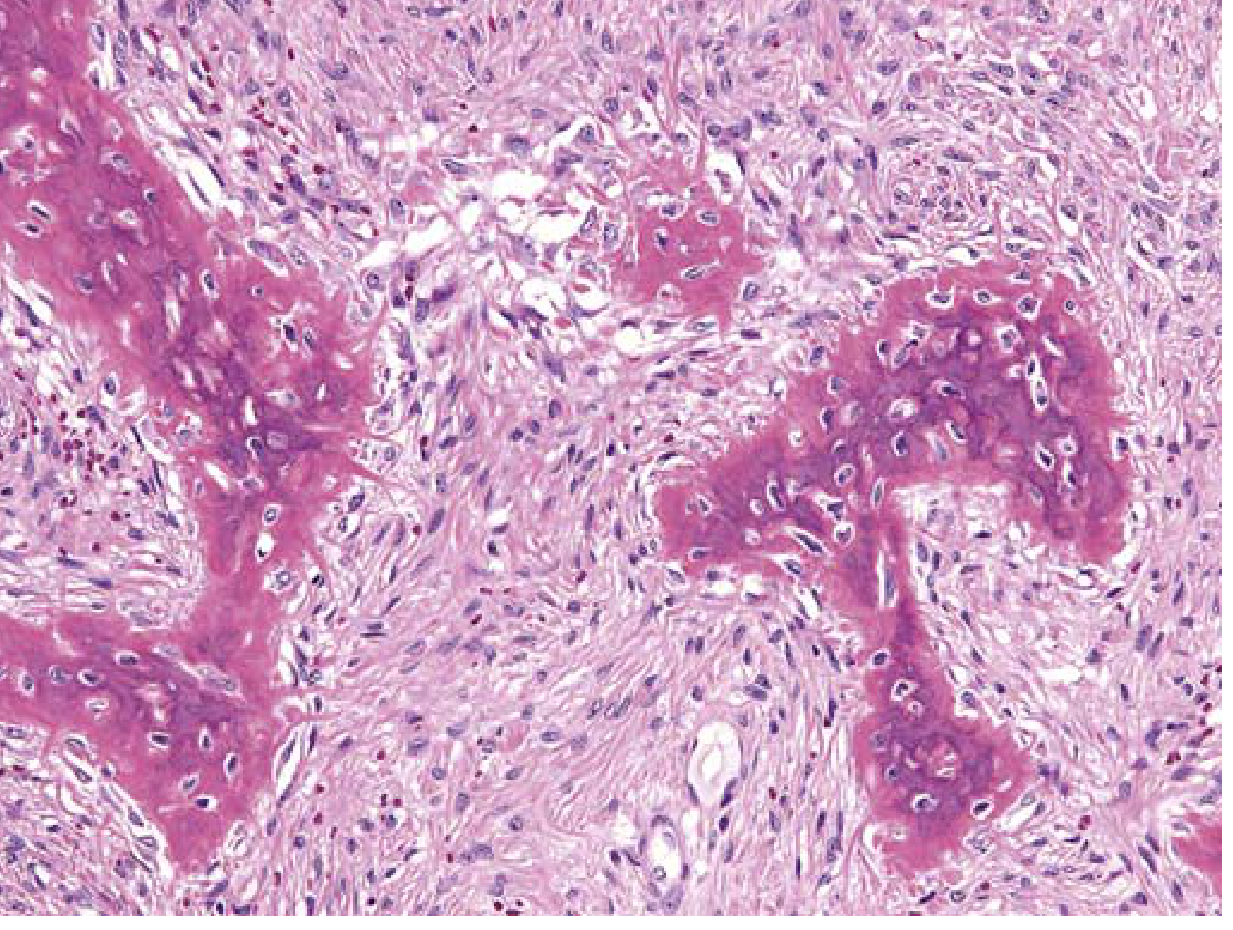
Histopathology
The classic microscopic picture (H&E):
- Intramedullary lesion with no capsule
- Curvilinear/Chinese-letter trabeculae of woven bone (immature, irregular, no lamellar pattern)
- Critically: no osteoblastic rimming of the bony trabeculae (this distinguishes FD from ossifying fibroma)
- Background of moderately cellular fibroblastic stroma in a whorled pattern
- Cystic degeneration, hemorrhage, and foamy macrophages may be present
FD vs. Ossifying Fibroma (Key Distinction)
| Feature | Fibrous Dysplasia | Ossifying Fibroma |
|---|---|---|
| Nature | Developmental/genetic anomaly | True benign neoplasm |
| Capsule | Absent | Present |
| Bone trabeculae | Woven, no osteoblastic rimming | More mature, osteoblastic rimming |
| CT | Ground-glass, no eggshell rim | Well-defined multiloculated, peripheral eggshell rim |
| MRI T2 | Hypointense | Hyperintense |
| Malignant transformation | Rare (0.5% polyostotic) | None reported |
| Recurrence after surgery | Less (if quiescent) | High, especially ethmoid |
- Cummings Otolaryngology
Laboratory Findings
- Serum alkaline phosphatase (ALP): elevated in ~30% of polyostotic cases
- Serum calcium and phosphorus: usually normal
- In extensive polyostotic disease: hypophosphatemia and hyperphosphaturia due to excess FGF-23 production by abnormal fibrous tissue (may cause rickets/osteomalacia)
- Bone turnover markers may be elevated
Complications
- Pathological fracture (more common in long bones)
- Cranial nerve compression - optic nerve at highest risk in craniofacial involvement
- Sinus obstruction and mucocele (frontal > maxillary)
- Sarcomatous transformation - rare but documented:
- 0.5% in polyostotic forms
- Up to 4% in McCune-Albright syndrome
- Radiation therapy increases this risk significantly
Treatment
Conservative (Preferred)
- Asymptomatic lesions should be observed with periodic clinical and radiological follow-up
- Lesions typically stabilize after skeletal maturation - surgery should be deferred in young patients when possible
Medical
- Bisphosphonates (e.g., IV pamidronate): inhibit osteoclastic activity; reduce bone pain and can partially resolve lesions; particularly useful for extensive disease with pain/disfigurement
- Denosumab: effective in reducing bone turnover markers; occasional hypercalcemia on discontinuation
Surgical
Indications:
- Optic nerve compression - most urgent; decompression now often achievable endoscopically (endonasal or transorbital)
- Severe aesthetic deformity - local controlled resection and recontouring
- Sinus obstruction - endoscopic sinus surgery for drainage
- Any rapidly growing or painful lesion (raises suspicion for sarcomatous change)
Radiotherapy is contraindicated - increases risk of malignant transformation (to osteosarcoma) and impairs facial growth in children.
- Cummings Otolaryngology; Scott-Brown's Otorhinolaryngology; Harrison's Principles of Internal Medicine 22E
Summary Points
- Caused by GNAS1 gain-of-function somatic mutation -> excess cAMP -> impaired osteoblast differentiation
- Maxilla is the most common craniofacial site in monostotic FD
- Classic CT finding: expansile lesion with ground-glass appearance
- Histology: woven bone trabeculae without osteoblastic rimming in fibrous stroma - no capsule
- Distinguish from ossifying fibroma: FD has no capsule, no osteoblastic rimming, CT shows no eggshell rim
- Surgery only for symptoms (optic nerve compression, deformity, sinus obstruction); defer in young patients
- Radiotherapy is absolutely contraindicated
- Malignant transformation (<1%) to osteosarcoma is a rare but recognized complication
Vocal cord fixity in laryngeal carcinoma is due to
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent - the textbooks have given a very detailed, sourced answer. Here is the complete breakdown:
Vocal Cord Fixity in Laryngeal Carcinoma
Vocal cord fixity (immobility) is a clinically significant finding that upgrades glottic carcinoma to T3 (or T4 if there is cartilage destruction). The causes depend on the site of the primary tumor.
Primary Cause: Invasion of the Thyroarytenoid (Vocalis) Muscle
The most common cause of a fixed vocal cord in glottic carcinoma is extensive invasion of the thyroarytenoid muscle (the intrinsic muscle that forms the bulk of the vocal cord itself).
Hirano and colleagues studied whole-organ sections and confirmed that:
- Impaired cord mobility = superficial thyroarytenoid invasion (or bulk/mass effect of an exophytic lesion on the cord surface)
- Fixed cord = deeper, more extensive invasion into the thyroarytenoid musculature
This is the single most important and most frequently cited mechanism.
- Cummings Otolaryngology Head and Neck Surgery
All Mechanisms of Vocal Cord Fixity
| Mechanism | Primary Site / Context |
|---|---|
| Thyroarytenoid (vocalis) muscle invasion | Glottic carcinoma - most common cause overall |
| Cricoarytenoid joint invasion | Glottic, subglottic, postcricoid, pyriform apex tumors |
| Lateral cricoarytenoid muscle invasion | Subglottic extension or deep glottic tumors |
| Deep arytenoid cartilage invasion | Supraglottic carcinoma (most common cause at this level) |
| Paraglottic space invasion | Transglottic, pyriform apex tumors - cord fixity by mass effect and muscle invasion |
| Posterior cricoarytenoid (PCA) muscle invasion | Postcricoid carcinoma - also causes aspiration |
| Recurrent laryngeal nerve invasion | Rare; extrinsic/advanced tumors |
Detail by Tumor Site
Glottic Carcinoma
- Fixity = almost always due to thyroarytenoid muscle invasion (deep muscle involvement)
- Subglottic extension can additionally fix the cord to the cricoid, and lateral extension can involve the lateral cricoarytenoid muscle and cricoarytenoid joint
Supraglottic Carcinoma
- Cord fixation here is less often due to thyroarytenoid invasion (as the tumor is above the glottis)
- Most common mechanism: deep arytenoid cartilage invasion superiorly
- An important distinction: "pseudofixation" (apparent impaired movement due to the weight/bulk of tumor pressing on the arytenoid from above) vs. true fixation (from actual malignant involvement of the cricoarytenoid joint or intrinsic muscles)
Pyriform Sinus (Hypopharyngeal) Carcinoma
- Tumors of the pyriform apex spread superiorly into the paraglottic space, causing cord fixity via:
- Mass effect impeding cord movement
- Invasion of intrinsic laryngeal muscles
- Also close proximity to the cricoarytenoid joint and recurrent laryngeal nerve
Postcricoid Carcinoma
- Invades the posterior cricoarytenoid muscle and cricoarytenoid joint, causing cord fixity and aspiration
TNM Staging Significance
| Cord Mobility | T Stage (Glottis) | Structural Correlate |
|---|---|---|
| Normal mobility | T1 | No significant deep invasion |
| Impaired mobility | T2 | Thyroarytenoid or lateral cricoarytenoid muscle infiltrated but not fully transgressed; no paraglottic fat involvement |
| Fixed cord | T3 | Extensive thyroarytenoid invasion; OR cricoarytenoid joint involved; OR paraglottic fat space invaded |
- Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Key Exam Point
The most common cause of vocal cord fixity in laryngeal carcinoma is invasion of the thyroarytenoid (vocalis) muscle. In glottic tumors this is the dominant mechanism. At the supraglottic level, arytenoid cartilage invasion takes over as the primary cause. Involvement of the cricoarytenoid joint (by glottic, subglottic, or postcricoid tumors) and paraglottic space invasion are additional important mechanisms.
Unilateral and bilateral vocal cord paralysis
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive, textbook-sourced account of unilateral and bilateral vocal cord paralysis:
Vocal Cord Paralysis (VCP)
Anatomy of the Nerve Supply
The vocal cords are innervated by the vagus nerve (CN X) via its branch, the recurrent laryngeal nerve (RLN):
-
Left RLN: loops under the aortic arch, then ascends in the tracheo-oesophageal groove - making it vulnerable to thoracic pathology
-
Right RLN: loops under the right subclavian artery, shorter course - less commonly affected by mediastinal lesions
-
~90% of paralyses result from peripheral nerve (RLN/vagus) lesions; only ~10% are central in origin
-
~75% of VCP cases are unilateral
-
Cummings Otolaryngology Head and Neck Surgery
Semon's Law
Injury to the RLN paralyzes the abductor (posterior cricoarytenoid, PCA) before the adductors. During recovery, the adductors recover first, before the abductor.
This explains the characteristic cord positions seen with incomplete vs. complete paralysis:
-
Partial/early RLN injury: cord sits in paramedian position (adductors still partially active, abductor lost)
-
Complete RLN paralysis: cord settles in the intermediate (cadaveric) position
-
Complete vagal (high) injury (above superior laryngeal nerve takeoff): cord assumes a more lateral/abducted position
-
KJ Lee's Essential Otolaryngology
Causes of Vocal Cord Paralysis
| Category | Specific Causes |
|---|---|
| Neoplastic (most common overall, ~36%) | Lung/bronchial tumors (left RLN), thyroid cancer, oesophageal cancer, laryngeal carcinoma, glomus jugulare, neck/mediastinal lymph nodes |
| Iatrogenic/Surgical (~25%) | Thyroidectomy (most common cause of unilateral VCP in adults), parathyroid surgery, carotid artery surgery, anterior cervical spine surgery, cardiac surgery (ligation of PDA - left RLN), oesophageal surgery |
| Inflammatory/Infectious (~13%) | Viral neuritis (idiopathic), syphilis, tuberculosis, Lyme disease |
| Idiopathic | Presumed viral; significant proportion, especially unilateral |
| Neurological | CVA/stroke, Arnold-Chiari malformation + hydrocephalus (bilateral, especially in children), ALS, multiple sclerosis, Wallenberg syndrome, poliomyelitis, pseudobulbar palsy |
| Trauma | Birth trauma, clothesline injury, penetrating neck injury, blunt cervical trauma |
- Textbook of Family Medicine 9e; Cummings Otolaryngology
Unilateral Vocal Cord Paralysis (UVCP)
Clinical Features
- Hoarseness - the dominant complaint; often breathy or weak voice
- Voice may normalize over time as the contralateral mobile cord compensates ("glottic competence")
- Aspiration - particularly with liquids; due to incomplete glottic closure
- Weak cough - inability to build up subglottic pressure (impaired Valsalva)
- Mild or no stridor - airway is usually adequate
- Dysphagia - especially with high vagal lesions
The paralyzed cord typically rests in the paramedian position.
Imaging Signs (CT/MRI)
- Paramedian position of the cord
- Anteromedial displacement of the arytenoid
- Ipsilateral piriform sinus dilatation
- Tilting of the thyroid cartilage
- Prominent laryngeal ventricle
Imaging should cover the entire course of the vagus nerve from skull base to pulmonary hila (CT neck/chest; MRI for skull base).
Prognosis
- ~70% of idiopathic unilateral VCP resolves spontaneously, most within the first 6 months
- Wait 12 months before proceeding to permanent surgical intervention in idiopathic cases
Management - Unilateral VCP
1. Observation + voice therapy - in early/mild cases; contralateral cord compensation often occurs
2. Injection laryngoplasty (temporary/permanent)
- Medialization of the paralyzed cord by injection of autologous fat, calcium hydroxyapatite, or other materials
- Can be done early (within waiting period) to improve voice and reduce aspiration risk
3. Medialization thyroplasty (Isshiki Type I)
- Permanent procedure for persisting unilateral VCP
- A silastic/Gore-Tex implant is placed through a cartilage window in the thyroid ala, medializing the vocal cord
- Performed under local anaesthesia so voice can be monitored intraoperatively
- Wait 12 months after idiopathic onset before performing this
4. Arytenoid adduction
- Added when there is a large posterior glottic gap or the paralyzed cord is on a different vertical plane than the contralateral cord
- Simulates contraction of the lateral cricoarytenoid muscle
5. Laryngeal reinnervation (ansa cervicalis to RLN)
-
Restores laryngeal tone; limited success in restoring voluntary movement
-
Scott-Brown's Otorhinolaryngology; Cummings Otolaryngology
Bilateral Vocal Cord Paralysis (BVCP)
Clinical Features
This is the more dangerous condition. Both cords rest near the paramedian position (adductors unopposed, abductors lost on both sides):
- Stridor - typically inspiratory, can be biphasic; the dominant and life-threatening symptom
- Voice may be near-normal - because the cords are close together, phonation is actually reasonable
- Airway compromise - may be severe, requiring emergency intubation or tracheostomy
- Aspiration - less prominent than in unilateral VCP
The classical paradox: in BVCP, the voice is preserved but the airway is at risk; in UVCP, the airway is preserved but the voice is affected.
Causes (Adult)
- Bilateral thyroid/parathyroid surgery (most common iatrogenic cause)
- CNS disorders: stroke, Arnold-Chiari malformation with hydrocephalus (brainstem herniation stretches both vagus nerves)
- Anterior cervical spine surgery
Management - Bilateral VCP
Emergency:
- Immediate intubation or tracheostomy if airway is compromised
Temporizing (while awaiting spontaneous recovery):
- Tracheostomy (required in ~50-73% of cases)
- Endoscopic anterior + posterior cricoid split (avoids tracheostomy in ~74%)
- Endoscopic percutaneous vocal fold lateralization
Definitive (if no spontaneous recovery after 2-3 years):
Goal: widen the posterior glottic aperture for breathing while preserving anterior glottis for voice
| Procedure | Details |
|---|---|
| Endoscopic CO2 laser posterior cordotomy | Resection of posterior true cord ± conus elasticus; widens glottis |
| Endoscopic laser arytenoidectomy (partial or total) | Removes arytenoid to lateralize cord; irreversible |
| External arytenoidectomy (Woodman procedure) | Open approach; older technique |
| Arytenoidopexy | Laterocervical fixation of arytenoid in an abducted position |
| Posterior costal cartilage graft laryngotracheoplasty | For associated subglottic stenosis |
| Permanent tracheostomy | Last resort |
All glottic widening procedures involve a trade-off: better airway at the cost of worse voice and potential aspiration.
Key Comparison Summary
| Feature | Unilateral VCP | Bilateral VCP |
|---|---|---|
| Cord position | Paramedian (one side) | Both paramedian |
| Primary symptom | Hoarseness, aspiration | Stridor, airway obstruction |
| Voice | Breathy/dysphonic | Relatively preserved |
| Airway | Safe | Endangered |
| Cough | Weak | Relatively intact |
| Emergency risk | Low | High - may need tracheostomy |
| Common causes | Thyroid surgery, lung cancer, idiopathic | Bilateral thyroid surgery, Arnold-Chiari |
| Main treatment | Medialization (injection or thyroplasty) | Glottic widening (cordotomy, arytenoidectomy) |
| Spontaneous recovery | ~70% idiopathic | Up to 65% (pediatric), less in adults |
- Cummings Otolaryngology; Scott-Brown's Otorhinolaryngology; Textbook of Family Medicine 9e; KJ Lee's Essential Otolaryngology
Recurrent laryngeal nerve paralysis
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive material from multiple authoritative sources. Here is the complete, detailed answer:
Recurrent Laryngeal Nerve (RLN) Paralysis
Anatomy and Embryological Basis for the Asymmetry
The RLN is the nerve of the 6th branchial arch. The asymmetry between left and right is rooted in embryology:
- The artery of the 6th arch becomes the ductus arteriosus, which:
- Obliterates on the right - so the right RLN "rises up" and only hooks around the right subclavian artery
- Descends into the thorax on the left - dragging the left RLN down to loop around the aortic arch (ligamentum arteriosum)
| Feature | Left RLN | Right RLN |
|---|---|---|
| Loops around | Aortic arch / ligamentum arteriosum | Right subclavian artery |
| Intrathoracic course | Long - through the chest | Short - only in the root of the neck |
| Vulnerability | Greater - to mediastinal/thoracic pathology | Less - limited to neck/root of neck |
| Ascent | In the left tracheo-oesophageal groove | In the right tracheo-oesophageal groove |
This explains why left RLN paralysis is more common in chest/mediastinal disease (aortic aneurysm, lung cancer, lymph node metastases, mitral stenosis), while right RLN paralysis is more often cervical in origin.
The nerve provides motor innervation to all intrinsic laryngeal muscles except the cricothyroid (supplied by the external branch of the SLN) and sensory innervation to the laryngeal mucosa below the vocal folds.
- Scott-Brown's Otorhinolaryngology; KJ Lee's Essential Otolaryngology
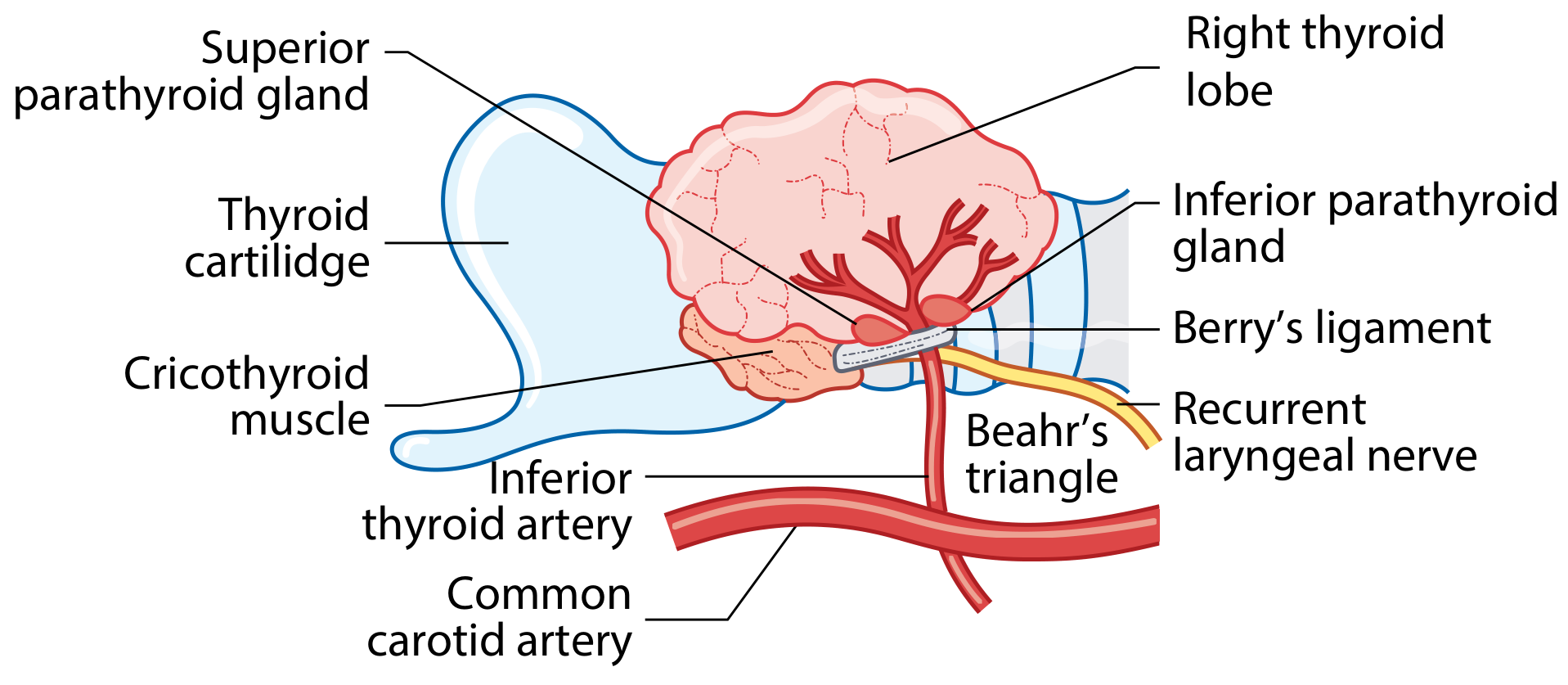
Relationship to the Inferior Thyroid Artery
The relationship of the RLN to the inferior thyroid artery is variable and surgically critical:
- The nerve may run deep to, superficial to, or between branches of the inferior thyroid artery
- The RLN passes in the vicinity of Berry's ligament (the posterior suspensory ligament of the thyroid), where it is at greatest risk during thyroidectomy
- A reliable surgical landmark is Beahr's triangle: formed by the common carotid artery laterally, inferior thyroid artery superiorly, and the trachea medially
Non-Recurrent Laryngeal Nerve (NRLN)
- Occurs in ~1% of individuals, almost always on the right side
- Associated with an aberrant retrooesophageal right subclavian artery (arteria lusoria): the right subclavian arises directly from the aorta instead of the innominate artery, so the right RLN has no vessel to hook around and travels directly from the vagus to the larynx
- A carotid artery originating directly from the aortic arch on preoperative imaging should alert the surgeon to a possible NRLN
- A left NRLN is extremely rare and implies situs inversus
- Failure to recognise a NRLN during thyroid surgery = high risk of transection
Causes of RLN Paralysis
Organized by anatomical segment of the nerve:
Central (10% of cases) - brainstem/before jugular foramen
- Stroke / CVA
- Arnold-Chiari malformation + hydrocephalus (bilateral - brainstem herniation)
- Multiple sclerosis
- Amyotrophic lateral sclerosis (ALS)
- Poliomyelitis, encephalitis
- Pseudobulbar/bulbar palsy
Central lesions virtually always affect other cranial nerves too - isolated central VCP is rare
Skull Base / Jugular Foramen
- Glomus jugulare tumour
- Nasopharyngeal carcinoma (base of skull extension)
- Meningioma, acoustic neuroma (rarely)
Cervical (neck)
| Cause | Notes |
|---|---|
| Thyroid surgery (most common cause overall) | ~1-2% permanent, 2-5% temporary; higher in revision surgery, cancer, substernal goiter |
| Thyroid malignancy (direct invasion) | Papillary/anaplastic carcinoma |
| Thyroid goiter (compression/stretch) | Especially substernal |
| Neck dissection | Central compartment clearance |
| Parathyroid surgery | Especially revision surgery |
| Carotid artery surgery (endarterectomy) | Stretch or clamp injury |
| Anterior cervical spine surgery | Particularly C3-C7 approach; right RLN at higher risk |
| Blunt neck trauma / penetrating injury | |
| Cervical lymphadenopathy (TB, metastases) | |
| Inflammatory: viral neuritis, sarcoidosis, Lyme disease, syphilis |
Thoracic / Mediastinal (particularly LEFT RLN)
| Cause | Notes |
|---|---|
| Lung carcinoma (most common malignant cause of left RLN palsy) | Left upper lobe / aortopulmonary window involvement; apex of right lung for right RLN |
| Aortic aneurysm (thoracic) | Ortner syndrome (see below) |
| Mitral stenosis - enlarged left atrium | Cardiovocal / Ortner syndrome |
| Mediastinal lymphadenopathy (lymphoma, TB, sarcoid, metastases) | |
| Oesophageal carcinoma | |
| Thymoma | |
| Cardiac surgery | Ligation of PDA (left RLN); valve surgery |
| Pneumonectomy | Scar, traction |
| Aortic surgery |
Ortner's Syndrome (Cardiovocal Syndrome)
Hoarseness due to left RLN compression by cardiovascular structures in the chest.
Originally described with mitral stenosis causing a massive dilated left atrium compressing the left RLN between the aorta and pulmonary artery. Now applied to any cardiovascular cause:
-
Mitral stenosis (classic - most common cardiac cause)
-
Thoracic aortic aneurysm / expanding proximal descending aorta
-
Patent ductus arteriosus (PDA)
-
Pulmonary artery hypertension with dilated pulmonary trunk
-
Harrison's Principles; Goldman-Cecil Medicine; KJ Lee's Essential Otolaryngology; Sabiston Textbook of Surgery
Clinical Features
Unilateral RLN Paralysis
- Hoarseness - breathy, weak voice; easily fatigued
- Diplophonia (two-pitch sound from unequal cord tension)
- Aspiration - especially liquids; weak cough
- Inability to sustain Valsalva (important in straining/heavy lifting)
- Cord position: paramedian
- Airway: usually adequate (no stridor in most cases)
- Combined SLN + RLN injury: cord lies more laterally, voice worse, aspiration greater
Bilateral RLN Paralysis
- Inspiratory stridor + respiratory distress (may be life-threatening)
- Voice relatively preserved (cords close together enable phonation)
- Less aspiration than unilateral
- Both cords in paramedian position - acute airway emergency possible
- May be missed initially if cords adapt; deteriorates over time as cords migrate to midline
Vocal Cord Position after RLN Injury
| Injury Level | Cord Position | Explanation |
|---|---|---|
| Complete RLN section | Intermediate (cadaveric) position | Loss of all intrinsic laryngeal muscles |
| Partial RLN injury | Paramedian position | Residual adductor tone (Semon's Law - abductors more sensitive) |
| High vagal lesion (above SLN takeoff) | Lateral/abducted position | Loss of all laryngeal muscle tone including SLN-supplied cricothyroid |
Semon's Law: Abductor fibers (to PCA muscle) are more susceptible to injury than adductor fibers. Hence in incomplete paralysis, abduction is lost first. During recovery, adductors recover first.
Investigations
- Flexible nasolaryngoscopy - gold standard; shows cord mobility, position, arytenoid movement
- CT neck + chest (skull base to pulmonary hilum) - evaluates entire RLN course
- MRI skull base - for central lesions, jugular foramen tumours
- Laryngeal EMG (electromyography) - distinguishes paralysis from mechanical fixation; predicts recovery potential; synkinetic activity or absent activity = poor prognosis
- Barium swallow, oesophagoscopy if oesophageal cause suspected
- Laryngoscopy palpation of arytenoid - distinguishes cricoarytenoid joint fixation from paralysis
Management
Of the Underlying Cause
- Always treat the primary cause first (e.g., thyroid cancer surgery, aortic repair)
- In Arnold-Chiari: shunting for hydrocephalus often restores cord function
Unilateral RLN Paralysis - Voice Rehabilitation
| Step | Treatment |
|---|---|
| Observation + voice therapy | Wait up to 12 months for spontaneous recovery (~70% idiopathic cases recover) |
| Injection laryngoplasty (temporary) | Carboxymethylcellulose (2-3 months), hyaluronic acid, calcium hydroxyapatite (~18 months), autologous fat - bridges the waiting period |
| Medialization thyroplasty (Isshiki Type I) | Permanent implant (Gore-Tex/silastic) via thyroid cartilage window; done under local anaesthesia; gold standard for permanent unilateral paralysis |
| Arytenoid adduction | Added when large posterior glottic gap or height mismatch between cords |
| Laryngeal reinnervation (ansa cervicalis to RLN) | Restores tone, prevents atrophy; does not restore voluntary motion but may improve outcome |
Bilateral RLN Paralysis - Airway Management
- Emergency intubation or tracheostomy if acute airway compromise
- Wait for spontaneous recovery (2-3 years; earlier if iatrogenic/pressure injury)
- Glottic widening procedures (permanent - trade-off voice for airway):
- Endoscopic CO2 laser posterior cordotomy (divide posterior cord + conus elasticus)
- Laser arytenoidectomy (partial or total) - most commonly used
- External arytenoidectomy (Woodman approach)
- Posterior costal cartilage graft laryngotracheoplasty - for associated subglottic stenosis
- Botulinum toxin to thyroarytenoid/lateral cricoarytenoid - temporary, palliative
- Permanent tracheostomy - last resort
If RLN Transected During Surgery (e.g., Thyroidectomy)
- Immediate microsurgical reanastomosis of proximal to distal nerve ends
- If not possible: ansa cervicalis to distal RLN anastomosis
- Goal: restore laryngeal muscle tone and prevent cord atrophy, even if voluntary motion does not return
Key Summary Points
- The left RLN loops under the aortic arch - vulnerable to thoracic/mediastinal disease
- The right RLN loops around the right subclavian - shorter, vulnerable mainly in the neck
- Non-recurrent LN (~1%): almost always right side, associated with aberrant right subclavian (arteria lusoria)
- Most common cause overall: thyroid surgery (iatrogenic)
- Most common malignant cause of left RLN palsy: lung carcinoma (aortopulmonary window)
- Ortner's syndrome: cardiovocal syndrome - left RLN compression by cardiovascular structure (mitral stenosis most classic)
- Semon's Law: abductors (PCA) fail first; adductors recover first
- Unilateral: paramedian cord, hoarseness, aspiration - airway safe
- Bilateral: both cords paramedian, stridor/airway crisis - voice preserved
- Investigations must cover skull base to pulmonary hila (full course of vagus/RLN)
- EMG helps distinguish paralysis from fixation and predicts recovery
Superior laryngeal nerve palsy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Here is a complete, textbook-sourced account of superior laryngeal nerve palsy:
Superior Laryngeal Nerve (SLN) Palsy
Anatomy of the SLN
The SLN arises from the inferior (nodose) ganglion of the vagus nerve (CN X) and receives a branch from the superior cervical sympathetic ganglion. It descends lateral to the pharynx, behind the internal carotid artery, and at the level of the greater cornu of the hyoid bone divides into two branches:
Internal Branch (larger - primarily sensory)
- Pierces the thyrohyoid membrane alongside the superior laryngeal artery
- Provides sensory and secretomotor innervation to the supraglottic larynx:
- Lower pharynx, epiglottis, vallecula, vestibule of larynx
- Aryepiglottic folds, mucosa down to the level of the vocal folds
- Also carries afferent fibres from neuromuscular spindles and stretch receptors in the larynx
- Ends by piercing the inferior constrictor to join an ascending branch of the RLN = loop of Galen (Galen's anastomosis - purely sensory)
- In its course under the mucosa of the medial wall of the piriform fossa, it is accessible for nerve block injection
External Branch (smaller - motor)
- Descends on the lateral edge of the inferior pharyngeal constrictor
- Terminates by supplying the cricothyroid muscle - the only intrinsic laryngeal muscle NOT supplied by the RLN
- Also supplies the inferior pharyngeal constrictor muscle
The cricothyroid muscle lengthens, tenses, and adducts the vocal folds - it is the primary muscle controlling voice pitch (especially high frequencies). It tilts the cricoid posteriorly against the fixed thyroid cartilage, increasing the distance between the vocal processes and the anterior commissure, thus tensing the vocal ligament.
- Scott-Brown's Otorhinolaryngology; Fischer's Mastery of Surgery
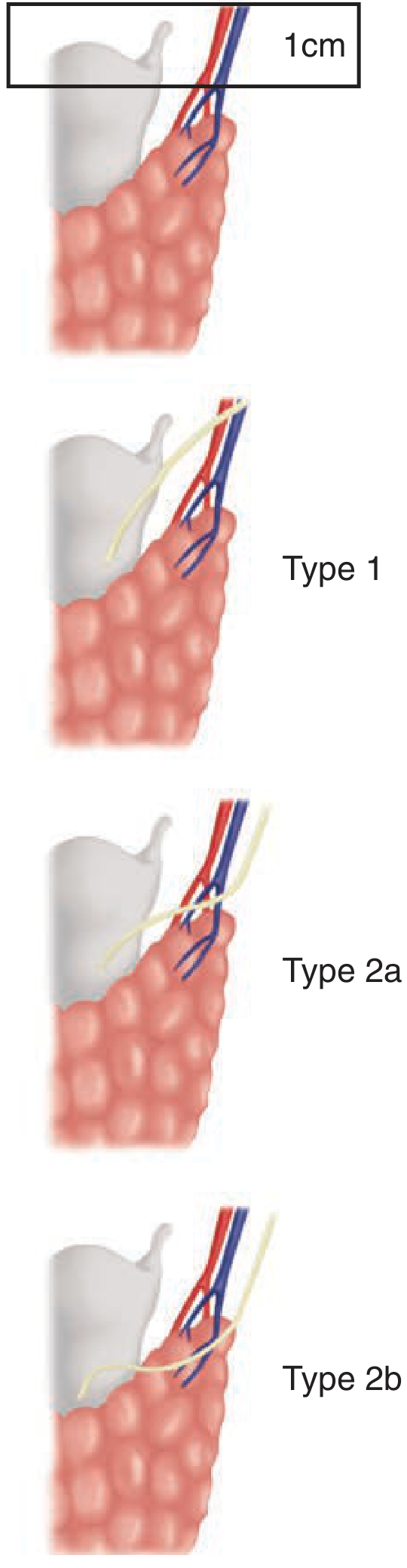
External Branch of SLN (EBSLN) - Cernea Classification
The EBSLN's relationship to the superior thyroid vessels is variable and surgically critical. Cernea classified this:
| Type | Description | Risk |
|---|---|---|
| Type 1 | Nerve crosses superior pole vessels ≥1 cm above the upper pole of the thyroid | Low risk |
| Type 2a | Nerve crosses within 1 cm of the upper border of the superior pole | Higher risk |
| Type 2b | Nerve crosses below the upper border of the superior pole | Highest risk - nerve lies within the surgical field during superior pole ligation |
- Type 2a occurs in ~20% of individuals - these nerves are subfacial and visually unidentifiable
- Up to 20% of EBSLN cannot be seen visually and require intraoperative nerve monitoring (IONM) for identification
The safe zone for EBSLN identification during thyroid surgery is Joll's (sternothyrolaryngeal) triangle, bounded by the superior thyroid pedicle and upper lobe of the thyroid, the cricothyroid muscle, and the lower edge of the thyroid cartilage.
Causes of SLN Palsy
External Branch (EBSLN)
- Thyroid surgery - most common cause; incidence of EBSLN injury up to 25% in thyroid surgery (many cases subclinical)
- Superior pole ligation en masse rather than on the thyroid capsule
- Neck dissection
- Trauma to the anterior neck
- Laryngeal/hypopharyngeal tumours
- Anterior cervical spine surgery
Internal Branch
- Thyroid surgery (rare - it is higher and more medial)
- Skull base tumours
- Trauma
- Viral/inflammatory neuritis
Both Branches (complete SLN palsy)
- High vagal lesions (above the SLN takeoff from the vagus)
- Jugular foramen tumours (glomus jugulare, paraganglioma)
- Skull base fractures
Clinical Features
EBSLN Injury (most clinically relevant)
The cricothyroid muscle is paralyzed on the affected side. Effects:
- Loss of high-pitched voice - inability to "hit high notes" or project the voice
- Voice fatigue during prolonged speech
- Reduction in vocal range - particularly high frequencies
- Diplophonia - two-pitch voice from unequal tension between the two cords
- Voice weakness and reduced projection - inability to shout
- Singers and vocal performers are disproportionately affected - this is why Semon called the EBSLN "the nerve of the singing voice"
- Symptoms may be subtle and unrecognised by the patient if they are not a voice professional
Bilateral EBSLN injury may produce hoarseness or easy voice tiring, but airway control is not jeopardised.
IBSLN Injury (internal branch)
The sensory supply to the supraglottic larynx is lost:
- Loss of laryngeal protective reflexes above the vocal folds
- Silent aspiration - material enters the larynx without triggering cough (very dangerous)
- Loss of cough reflex (supraglottic/reflex cough driven by laryngeal mucosa sensation)
- Recurrent aspiration pneumonia
- Combined SLN + RLN injury: cord lies more laterally, aspiration is more severe
Complete SLN Palsy (both branches)
- All of the above: pitch loss + aspiration + voice weakness
- Asymmetric glottic appearance on laryngoscopy
Laryngoscopic / Videostroboscopic Findings (EBSLN palsy)
- Asymmetric glottic aperture - the affected cord appears shorter and sits at a different vertical level
- Rotation of the posterior glottis - posterior commissure rotates toward the affected side (arytenoid of the affected side tilts forward and down)
- Shortening/bowing of the ipsilateral vocal cord (loss of tension from cricothyroid)
- The affected cord vibrates at a lower frequency than the contralateral cord - hence diplophonia
Comparison: EBSLN vs RLN Injury
| Feature | EBSLN Injury | RLN Injury |
|---|---|---|
| Muscle affected | Cricothyroid (pitch/tension) | All intrinsic muscles except cricothyroid |
| Cord mobility | Preserved (cord still moves) | Lost (cord fixed) |
| Voice | Loss of high pitch, fatigue, reduced range | Hoarseness, breathiness, weak voice |
| Aspiration | Minimal (only if combined with IBSLN) | Present (glottic incompetence) |
| Airway | Safe | Safe (unilateral); Dangerous (bilateral) |
| Laryngoscopic appearance | Asymmetric glottis, cord shortened | Cord fixed paramedian |
| Frequency of recognition | Often unrecognised | Usually recognised |
| Incidence post-thyroidectomy | Up to 25% | 1-2% permanent |
- Cummings Otolaryngology; Localization in Clinical Neurology; Morgan and Mikhail's Clinical Anesthesiology
Diagnosis
- Careful post-operative voice assessment: pitch, strength, fatigue, projection - surgeon must specifically ask
- Videostroboscopy - gold standard; shows asymmetric cord tension, pitch asymmetry, abnormal mucosal wave
- Laryngeal EMG - confirms cricothyroid denervation
- Voice analysis (acoustic analysis) - documents reduced pitch range
- Imaging if non-iatrogenic cause suspected (CT neck/skull base)
Management
- Voice therapy - primary treatment; teaches compensatory techniques to improve pitch and projection
- Observation - many cases mild and partially recover
- No specific surgical intervention is routinely available for isolated EBSLN injury
- For internal branch injury (aspiration): dietary modification, upright feeding posture, speech-language therapy, rarely surgical airway protection measures
- Prevention is key:
- Identify and preserve the EBSLN during superior pole dissection (Joll's triangle)
- Ligate superior pole vessels individually on the thyroid capsule, not en masse
- Use intraoperative nerve monitoring (IONM) - especially for high-risk cases (revision surgery, Graves', large goitre)
Key Points Summary
- SLN = internal branch (sensory, supraglottis) + external branch (motor, cricothyroid only)
- EBSLN injury: preserved cord mobility but loss of pitch, projection, and high notes - "singer's nerve"
- IBSLN injury: silent aspiration without triggering cough reflex
- Most common cause: thyroid surgery - en masse superior pole ligation
- Cernea Type 2b: highest surgical risk (nerve below the superior pole)
- Up to 25% of thyroid operations injure the EBSLN - most are subclinical
- Combined RLN + SLN injury produces a more laterally positioned cord and worse voice/aspiration than RLN injury alone
- Diagnosis requires videostroboscopy - standard laryngoscopy is insufficient as cord movement is preserved
Superior laryngeal nerve palsy
I just covered this topic in detail in my previous response. Here is a concise structured summary for quick reference:
Superior Laryngeal Nerve (SLN) Palsy - Summary
The Two Branches
| Branch | Type | Supplies | Function |
|---|---|---|---|
| Internal branch (larger) | Sensory + secretomotor | Laryngeal mucosa above vocal folds, epiglottis, piriform fossa, stretch receptors | Laryngeal protective reflexes, cough reflex, sensation |
| External branch (smaller) | Motor | Cricothyroid muscle only (+ inferior constrictor) | Lengthens, tenses, adducts vocal folds - controls pitch |
Both branches divide at the level of the greater cornu of the hyoid bone.
Effects of Each Branch Injury
External Branch (EBSLN) Palsy
- Cricothyroid paralysis → cord cannot be properly tensed
- Loss of high-pitched voice - cannot hit high notes
- Reduced vocal range (especially upper frequencies)
- Voice fatigue and reduced projection
- Cannot shout
- Diplophonia (unequal cord tension → two simultaneous pitches)
- Cord mobility is preserved (cord still moves - abducts/adducts normally)
- Laryngoscopy: asymmetric glottis, ipsilateral cord shortened and lower, posterior commissure rotated toward affected side
- Airway: safe
Internal Branch Palsy
- Loss of supraglottic sensation
- Silent aspiration (no cough triggered when food/liquid enters larynx)
- Loss of protective cough reflex
- Recurrent aspiration pneumonia risk
- Airway: safe but aspiration risk
Combined SLN + RLN Injury (high vagal lesion)
- Cord lies more laterally (not just paramedian)
- Worse voice, worse aspiration, less glottic competence than RLN alone
Causes
| Cause | Branch most affected |
|---|---|
| Thyroid surgery (most common - up to 25%) | EBSLN |
| En masse superior pole ligation | EBSLN |
| Neck dissection | Either |
| Anterior cervical spine surgery | Either |
| Hypopharyngeal/laryngeal tumours | Either |
| Jugular foramen tumours (glomus) | Both (complete SLN) |
| Skull base fracture/tumours | Both |
| High vagal lesions | Both (+ RLN) |
| Viral neuritis | Either |
Cernea Classification (EBSLN vs. superior thyroid vessels)
| Type | Position of EBSLN | Risk during thyroidectomy |
|---|---|---|
| Type 1 | Crosses vessels ≥1 cm above upper pole | Low |
| Type 2a | Crosses vessels within 1 cm of upper pole | Moderate (~20% of people) |
| Type 2b | Crosses vessels below upper pole | Highest - lies in the surgical field |
Safe identification zone: Joll's triangle (superior thyroid pedicle + cricothyroid muscle + lower thyroid cartilage).
Diagnosis
- Videostroboscopy - gold standard; shows cord tension asymmetry, abnormal mucosal wave, asymmetric glottis
- Laryngeal EMG - confirms cricothyroid denervation
- Acoustic voice analysis - documents reduced pitch range
- Standard laryngoscopy alone is insufficient (cord still moves - easy to miss)
Management
- Voice therapy - primary treatment for EBSLN injury; compensatory technique training
- Observation (many cases mild, some recover spontaneously)
- Internal branch injury: dietary modification, safe swallowing techniques, aspiration precautions
- Prevention during thyroid surgery:
- Identify EBSLN in Joll's triangle before ligating superior pole
- Ligate superior pole vessels individually on the thyroid capsule (not en masse)
- Use intraoperative nerve monitoring (IONM) in high-risk cases
Key Exam Points
- EBSLN = "nerve of the singing voice" - loss of pitch, not cord movement
- IBSLN = loss of sensation → silent aspiration (most dangerous consequence)
- Most common cause = thyroid surgery (superior pole dissection)
- Cord is mobile on laryngoscopy despite EBSLN injury - easily missed clinically
- Cernea Type 2b = highest surgical risk
- Bilateral EBSLN injury = hoarseness/voice fatigue but airway is safe
Eustachian tube tests
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Excellent material gathered. Here is the comprehensive answer:
Eustachian Tube (ET) Tests
Background
The Eustachian tube has three key functions:
- Ventilation - equalizes middle ear pressure with ambient atmospheric pressure
- Drainage - clears secretions from the middle ear by mucociliary clearance and gravity
- Protection - prevents reflux of nasopharyngeal contents into the middle ear
ET dysfunction falls into two broad categories - obstructive (fails to open) and patulous (fails to close) - and the tests used differ for each. Importantly, no single test reliably diagnoses ET dysfunction, and tests often correlate poorly with clinical outcomes.
- Cummings Otolaryngology; Scott-Brown's Otorhinolaryngology
I. Clinical / Bedside Tests
1. Valsalva Maneuver
- How: Patient pinches both nostrils, closes mouth, and blows gently (raises intranasal pressure)
- What it tests: Whether positive pressure can be forced through the ET into the middle ear
- Normal result: Patient feels a "pop" in the ear; TM seen to move outward (lateralise) on otoscopy
- Limitation: Tests ET patency under forced conditions only - does not assess physiological (active, swallow-induced) function
- Sensation of equalization during Valsalva has 0% positive predictive value for predicting barotrauma risk
- Failure to equalize during diving = 91% chance of developing middle ear barotrauma
2. Toynbee Test
- How: Patient pinches both nostrils and swallows (raises nasopharyngeal pressure transiently, then creates negative pressure)
- What it tests: ET opening and closing during swallowing - more physiological than Valsalva
- Normal result: A pressure change is felt in the ear; TM moves inward (medialises) then returns to normal
- Positive predictive value for barotrauma: ~25%
- Combining the Toynbee test with the nine-step inflation-deflation test achieves 100% predictive accuracy for barotrauma risk
3. Politzerization (Politzer's Method)
- How: An olive-tipped bulb is placed in one nostril, the other nostril occluded; patient swallows or says "K" while the bulb is compressed - forces air into nasopharynx
- What it tests: Forced inflation of the ET and middle ear
- Normal result: Patient hears/feels a "pop"; TM seen to move outward
- Also used therapeutically (ET inflation for otitis media with effusion)
- Can be combined with auscultation tube (see below)
4. Catheterization of Eustachian Tube
- Historically used for both diagnosis and treatment (delivering air or fluid directly via catheter)
- A metal catheter is passed via the nose, rotated to engage the ET orifice, and air is insufflated
- Allows direct assessment of patency; combined with auscultation tube to hear air entering
- Largely abandoned due to difficulty and risk of serious complications
- Now replaced by nasal endoscopy-guided approaches
5. Auscultation of Eustachian Tube (Pertusson's Tube / Listening Tube)
- A rubber tube with olivary tips is placed in the examiner's ear and patient's ear simultaneously
- Air entry into the middle ear is heard during Valsalva/Politzer/catheterization
- A crackling or rushing sound = patent ET
- Largely historical
II. Objective Instrumental Tests
6. Tympanometry
The most practical and widely used indirect ET function test:
| Tympanogram Type | Interpretation |
|---|---|
| Type A (normal) | Normal ET function, normal middle ear pressure |
| Type As (shallow) | Reduced compliance - otosclerosis, tympanosclerosis |
| Type Ad (deep/flaccid) | Increased compliance - ossicular discontinuity |
| Type B (flat) | Middle ear effusion or TM perforation |
| Type C (negative peak pressure) | Negative middle ear pressure = ET obstruction/dysfunction |
- Type C tympanogram is the hallmark of obstructive ET dysfunction
- Used serially to monitor response to treatment
- In patulous ET: tympanometry in reflex decay mode during ipsilateral nasal breathing shows oscillating compliance changes synchronous with respiration - a sensitive diagnostic sign
7. Nine-Step Inflation-Deflation Tympanometric Test (Bluestone's Test)
- Specifically designed for patients with TM perforation or ventilation tubes (as the middle ear is accessible)
- How it works:
- Baseline tympanogram performed
- Positive pressure applied to the EAC (inflates middle ear)
- Patient swallows - ET opening recorded as pressure equalisation
- Negative pressure applied to EAC (deflates middle ear)
- Patient swallows again - ET opening and re-equilibration recorded
- Steps repeated - assessing active opening with swallowing in both directions
- 9 sequential pressure steps map ET ability to open against positive and negative pressures
- Positive predictive value for barotrauma: 25%; Negative predictive value: 75%
- Combined with Toynbee test: 100% predictive accuracy
- Used clinically before tympanoplasty in children to assess ET function
8. Forced Response Test
- Requires a TM perforation or patent ventilation tube
- A tympanometry probe + air pump is placed in the EAC
- Progressively increasing pressure is applied until the ET is forced open
- The opening pressure and resistance of the ET are measured
- Resistance can be measured during swallowing
- Used in research settings; limited widespread clinical use
9. Inflation-Deflation Test (simple)
- Uses a tympanometry probe in the EAC to record pressure changes while the patient swallows
- Does not require a TM perforation
- Less specific than the nine-step version
- Used to evaluate ET function before tympanoplasty
10. Tubomanometry
- A pressure probe is placed in the nasopharynx; tympanometry probe in EAC
- Increasing pressure applied at the nasopharynx while patient swallows with mouth closed
- The ET opening pressure = abrupt change in ear canal pressure
- Measures the nasopharyngeal pressure required to open the ET
- More physiological than forced response test
- Used mainly as a research tool; increasingly used clinically in Europe
11. Sonotubometry (Acoustic Reflectometry / Sonometry)
- A sound probe emits a tone inside the nasal cavity
- A microphone in the EAC detects changes in amplitude of the sound when the ET opens
- ET opening = increased sound transmission = detected as amplitude increase
- Non-invasive; does not require TM perforation
- Assesses physiological (swallow-induced) ET opening
- Can be combined with tubotympanometry
- Suggested as useful for predicting barotrauma risk
12. Pressure Chamber Test
- The patient is placed in a pressure chamber
- Controlled pressure changes simulate the conditions of flying or diving
- Tympanometry and symptoms are monitored before, during, and after pressure change
- Useful for aviation/diving medicine - predicts susceptibility to barotrauma
- Impractical as a routine clinical tool
III. Tests for Patulous Eustachian Tube
Patulous ET requires different diagnostic approach than obstructive ET:
| Test | Findings in Patulous ET |
|---|---|
| Otoscopy / Micro-otoscopy | TM excursions (in and out) synchronous with nasal breathing - visible best in upright position in the posterosuperior quadrant |
| Tympanometry (reflex decay mode) | Oscillating compliance changes synchronous with nasal breathing - more sensitive than visual observation alone |
| Nasopharyngoscopy | Longitudinal concave defect in the anterolateral wall of the ET lumen; tube visible as persistently open |
| Autophony test | Patient reports hearing own breathing/voice; TM excursions observed during forced nasal breathing (mouth and opposite nostril closed) |
- Diagnosis confirmed by observing TM excursions coincident with ipsilateral nasal breathing when autophony is active
- Patient examined sitting upright (lying supine causes venous congestion that may transiently close the patulous tube and mask findings)
- Sniffing temporarily relieves symptoms (negative pressure retracts TM) but can complicate diagnosis
Summary Comparison Table
| Test | Requires TM perforation? | Type of ET dysfunction assessed | Clinical use |
|---|---|---|---|
| Valsalva | No | Obstructive (forced) | Bedside; low sensitivity |
| Toynbee | No | Obstructive (physiological) | Bedside; PPV 25% |
| Politzerization | No | Obstructive (forced) | Bedside + therapeutic |
| Tympanometry (Type C) | No | Obstructive | Routine clinical |
| Nine-step tympanometric | Yes (perforation/tube) | Obstructive (quantitative) | Pre-tympanoplasty |
| Forced response test | Yes | Obstructive (opening pressure) | Research |
| Inflation-deflation | No | Obstructive | Pre-tympanoplasty |
| Tubomanometry | No | Obstructive (opening pressure) | Research + clinical |
| Sonotubometry | No | Obstructive (acoustic) | Research |
| Pressure chamber | No | Obstructive (barotrauma) | Aviation/diving |
| TM excursion + nasal breathing | No | Patulous | Bedside |
| Tympanometry (reflex decay) | No | Patulous | Clinical |
| Nasopharyngoscopy | No | Patulous | Clinical |
Key Exam Points
- No single test reliably diagnoses ET dysfunction - diagnosis relies on combined clinical + instrumental findings
- Valsalva + Toynbee = bedside tests for patency only; do not assess physiological function
- Nine-step test requires a TM perforation or grommet
- Toynbee + nine-step test combined = 100% accuracy for predicting barotrauma
- Type C tympanogram = negative middle ear pressure = obstructive ET dysfunction
- Patulous ET: TM moves with nasal breathing (not with swallowing) - confirmed by tympanometry on reflex decay mode
- Patulous ET: symptoms worse upright, better supine (opposite of obstructive ETD)
- Cummings Otolaryngology; Scott-Brown's Otorhinolaryngology; Shambaugh Surgery of the Ear
Frenzel manuvre
Finding Sources
Finding Sources
Reading File
Finding Sources
The textbooks address both usages of Frenzel. Here is the complete answer covering both meanings:
The Frenzel Maneuver - Two Distinct Meanings
The term "Frenzel maneuver" is used in two completely different clinical contexts in ENT and otology:
- Frenzel maneuver = an ear equalization technique (ET opening) used in diving
- Frenzel lenses/glasses = optical devices used in vestibular examination
1. Frenzel Maneuver - Eustachian Tube Equalization
What It Is
A technique for equalizing middle ear pressure, primarily used by divers and free-divers, that uses the tongue as a piston to compress air in the closed nasopharynx and push it through the Eustachian tube - without using lung pressure.
How to Perform It
- Pinch both nostrils shut (close off the nasal passage externally)
- Close the glottis (close the throat - unlike Valsalva where the glottis may be open)
- Place the tongue on the roof of the mouth, as far forward as possible
- Gently move the back of the tongue upward - as when beginning to swallow - compressing the air in the nasopharynx
- This compressed air is forced up the Eustachian tube into the middle ear
- Repeat as many times as necessary until equalization (the "pop") occurs
Key Mechanism
- The tongue acts as a piston/pump compressing the nasopharyngeal air column
- The glottis is closed throughout - no lung air is involved
- This is fundamentally different from Valsalva, which uses forced expiratory effort from the lungs
Comparison with Other Equalization Methods
| Method | Mechanism | Glottis | Pressure source | Force |
|---|---|---|---|---|
| Valsalva | Forced expiration against closed nostrils | Open | Lung/intrathoracic pressure | High - risk of barotrauma |
| Frenzel | Tongue piston compresses nasopharyngeal air | Closed | Nasopharyngeal air only | Gentle - preferred |
| Toynbee | Swallowing with nostrils pinched | Closed | Swallowing-created negative pressure | Passive |
| Edmonds | Jaw thrust + Frenzel | Closed | Tongue + jaw movement | Moderate |
Advantages of Frenzel over Valsalva
- Gentler - lower pressure generated, less risk of oval/round window rupture
- Can be performed hands-free (important during diving)
- Can be used at greater depths where lung volume is compressed and Valsalva becomes impossible (in free-diving)
- Does not raise intrathoracic pressure (no risk of air embolism from pulmonary barotrauma)
- Preferred technique for free-divers (breath-hold diving)
Clinical Relevance
-
Used therapeutically: after middle ear barotrauma with serous otitis, repeated Frenzel maneuvers help displace fluid through the Eustachian tube
-
Divers unable to equalize should not dive
-
Antihistamines should be avoided before diving (cause dry mouth and drowsiness)
-
Prophylactic nasal decongestants (pseudoephedrine 60 mg orally 30 min before, or oxymetazoline spray) may reduce middle ear barotrauma incidence
-
Rosen's Emergency Medicine
2. Frenzel Lenses / Frenzel Glasses - Vestibular Examination
What They Are
Frenzel lenses (also called Frenzel glasses) are high-powered magnifying lenses (+15 to +20 diopters) built into an illuminated frame, worn by the patient during vestibular testing.
Purpose
- Eliminate visual fixation - the thick lenses prevent the patient from focusing on any point, removing the ability to suppress nystagmus by fixation
- Illuminate and magnify the eyes so the examiner can clearly observe nystagmus
Why Fixation Suppression Matters
- Vestibular nystagmus (caused by asymmetric vestibular input) is suppressed by visual fixation via the cerebellum
- With fixation, peripheral vestibular nystagmus may not be visible even when present
- Frenzel lenses remove fixation, making peripheral vestibular nystagmus apparent
Clinical Applications
| Test | Why Frenzel Lenses Are Used |
|---|---|
| Spontaneous nystagmus assessment | Reveals low-amplitude nystagmus hidden by fixation suppression |
| Dix-Hallpike maneuver (BPPV) | Standard requirement - prevents fixation suppression of positional nystagmus |
| Head shake test | Patient shakes head rapidly 10-15 sec; Frenzel lenses reveal post-head-shake nystagmus indicating vestibular asymmetry |
| Positional tests (roll test, etc.) | All positional maneuvers benefit from Frenzel to unmask nystagmus |
| Pneumatic otoscopy / pressure tests | Observe pressure-induced nystagmus (Hennebert sign - superior canal dehiscence, perilymph fistula) |
| Caloric testing | Monitor caloric-induced nystagmus |
| Valsalva / straining nystagmus | Look for nystagmus in Arnold-Chiari, SSCD, perilymph fistula |
Key Properties
- +15 to +20 diopters: too thick for the patient to focus, but examiner can see eyes clearly through the illuminated frame
- Some modern equivalents use infrared video goggles (videonystagmography - VNG), which are more sensitive than Frenzel lenses and allow recording
- Frenzel lenses only eliminate fixation; they do not amplify to the degree of VNG
Frenzel vs. VNG Goggles
| Feature | Frenzel Lenses | VNG Goggles |
|---|---|---|
| Fixation removal | Yes | Yes |
| Recording capability | No | Yes |
| Nystagmus direction/velocity | Estimated | Quantified |
| Beat direction | Visible | Measured |
| Availability | Bedside (cheap) | Laboratory (expensive) |
| Portability | Excellent | Moderate |
Key Points Summary
Frenzel Maneuver (ET equalization):
- Tongue piston compresses nasopharyngeal air with glottis closed
- Gentler than Valsalva - preferred by divers, especially free-divers
- No lung pressure involved - safer for inner ear
- Used therapeutically after middle ear barotrauma
Frenzel Lenses (vestibular testing):
- High-power (+15-20 D) illuminated lenses that remove visual fixation
- Reveal peripheral vestibular nystagmus otherwise suppressed by fixation
- Essential for Dix-Hallpike, positional tests, and any nystagmus assessment
- Modern equivalent: VNG infrared goggles (recordable)
- Rosen's Emergency Medicine; Shambaugh Surgery of the Ear; Scott-Brown's Otorhinolaryngology; Localization in Clinical Neurology
This is a shared conversation. Sign in to Orris to start your own chat.