Valsalva
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the Valsalva maneuver drawn from multiple authoritative textbooks.
The Valsalva Maneuver
Definition: Forced expiration against a closed glottis, generating an increase in intrathoracic pressure of ~30–40 mmHg for at least 10 seconds. It occurs physiologically during coughing, defecation, heavy lifting, vomiting, and childbirth.
How to Perform It
A simple bedside method: ask the patient to place their thumb in their mouth with closed lips and attempt to exhale without expelling air — or bear down as if to defecate. Alternatively, place the examiner's hand over the patient's abdomen and ask them to push against it. Standard strain is maintained for 10–20 seconds with the patient supine and legs passively raised (modified Valsalva).
The Four Phases
| Phase | Event | Hemodynamic Change |
|---|---|---|
| I — Onset of strain | Intrathoracic pressure transmitted to aorta | Transient ↑ BP |
| II — Sustained strain | ↓ Venous return → ↓ stroke volume, ↓ pulse pressure | ↓ BP + reflex tachycardia (sympathetic ↑, parasympathetic ↓) |
| III — Release | Initial drop as intrathoracic pressure normalizes | Brief further ↓ BP |
| IV — Recovery (overshoot) | Venous return restored into a vasoconstricted, sympathetically activated heart | BP overshoots above baseline → baroreceptor-mediated reflex bradycardia |
The most important heart rate changes: reflex tachycardia in Phase II and reflex bradycardia in Phase IV. If tachycardia is absent in Phase II, consider autonomic dysfunction, β-blocker use, or elevated left-sided filling pressures.
Cardiovascular Uses
1. SVT Termination
By increasing vagal tone, the Valsalva maneuver slows SA and AV node conduction. It produces the greatest mean vagal response of vagal maneuvers (greater than carotid sinus massage). The modified Valsalva (strain → immediate supine repositioning + 15-second passive leg raise) increases efficacy in converting SVT.
2. Dynamic Auscultation — Murmur Differentiation
During Phase II (reduced ventricular filling), most systolic murmurs decrease in intensity. Two critical exceptions:
| Condition | Effect on Murmur | Mechanism |
|---|---|---|
| HOCM (hypertrophic obstructive cardiomyopathy) | Louder | Smaller LV cavity → greater subaortic obstruction |
| MVP (mitral valve prolapse) | Louder + longer | Reduced LV size → earlier leaflet prolapse; click moves closer to S1 |
| Aortic stenosis | Softer | Fixed obstruction, reduced flow |
| Mitral regurgitation | Softer | Reduced flow |
During Phase IV, nearly all murmurs increase — except HOCM (increased ventricular filling reduces obstruction).
3. Autonomic Testing
The maneuver tests baroreceptor reflex integrity. Blowing into a closed system to 40 mmHg for 12 seconds while monitoring BP and HR allows assessment of sympathetic and parasympathetic function:
- In autonomic insufficiency: heart rate changes are absent
- In primary hyperaldosteronism: abnormal response that normalizes after tumor removal
- Intact vagi are needed for the HR changes; sympathetic function drives the BP overshoot in Phase IV
Other Clinical Contexts
- Laryngology: The larynx closes tightly with inflated lungs, stabilizing the thorax for muscular actions (lifting) and increasing intra-abdominal pressure for defecation/childbirth
- Ophthalmology (Valsalva retinopathy): Forceful Valsalva during coughing, vomiting, or straining can cause sudden ↑ intraocular venous pressure, rupturing superficial retinal capillaries
- Urology/pelvic floor: EMG activity should increase during Valsalva to maintain continence; absence suggests pelvic floor dysfunction
- GI radiology: Prolonged Valsalva during imaging can unmask small hernias or defects
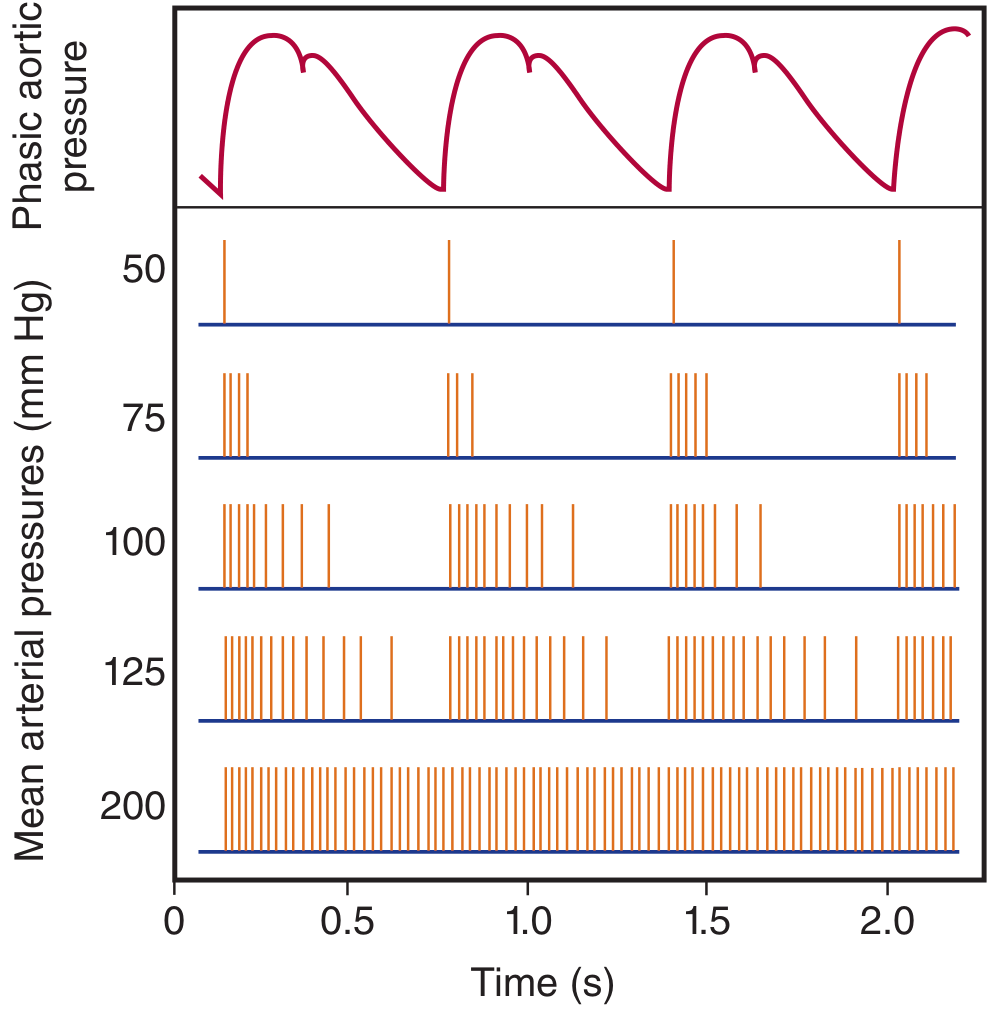
Baroreceptor Response (Graph)
The graph below (from Ganong's Review of Medical Physiology) shows baroreceptor discharge frequency at various mean arterial pressures alongside phasic aortic pressure — illustrating the sensitivity of the system to changes in pulse pressure that the Valsalva maneuver exploits:
Sources: Ganong's Review of Medical Physiology (26e) | Fuster and Hurst's The Heart (15e) | Harrison's Principles of Internal Medicine (22e) | Braunwald's Heart Disease | Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.