Chemoreceptors of digestive system and it’s stimulus
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have solid information from multiple textbooks. Let me compile a comprehensive answer.
Chemoreceptors of the Digestive System and Their Stimuli
Chemoreceptors in the digestive system are specialized sensory structures that detect the chemical composition of luminal contents and trigger appropriate secretory, motor, and absorptive responses. They operate at three levels: mucosal enteroendocrine cells, intrinsic primary afferent neurons (IPANs), and extrinsic afferent neurons (vagal and spinal).
1. Enteroendocrine (EE) Cells - The Primary Chemoreceptors
These scattered epithelial cells in the GI mucosa act as chemosensors. They detect luminal chemicals and respond by secreting hormones/paracrine agents. There are over 17 types identified by TEM, classified by secretory vesicle morphology and immunochemical staining.
| Cell Type | Location | Hormone Secreted | Chemical Stimuli |
|---|---|---|---|
| G cells | Stomach antrum, duodenum | Gastrin | Proteins/amino acids, distension, vagal (ACh), gastrin-releasing peptide (GRP/bombesin) |
| ECL cells | Gastric fundus mucosa | Histamine | Gastrin, ACh (paracrine - stimulates parietal cells for acid secretion) |
| S cells | Duodenum and jejunum | Secretin | Acid (pH <4.5), fatty acids (C10+ chain), alcohol (indirectly via acid) |
| I cells | Duodenum and proximal jejunum | Cholecystokinin (CCK) | Fat (fatty acids), proteins (amino acids), HCl in duodenum |
| K cells | Duodenum and jejunum | Gastric Inhibitory Peptide (GIP) | Fat, glucose, amino acids |
| L cells | Ileum and colon | GLP-1, GLP-2, Peptide YY (PYY) | Fat, glucose, protein in ileum/colon |
| D cells | Throughout GI mucosa + pancreas | Somatostatin | Fat, proteins, acid, glucose, amino acids, CCK (acts as paracrine inhibitor of other cells) |
| EC (Enterochromaffin) cells | Throughout GI mucosa | Serotonin (5-HT) | Mechanical distension, acid, alkaline pH, nutrients |
| X/A cells | Gastric fundus | Ghrelin | Fasting state (empty stomach), decreased glucose |
| M cells (Mo) | Small intestine | Motilin | Fasting, alkaline pH in duodenum |
| PP cells | Pancreatic islets | Pancreatic Polypeptide | Protein (most potent), fat, glucose |
| N cells | Ileum | Neurotensin | Fat (especially long-chain fatty acids) |
(Sources: Histology: A Text and Atlas, Tietz Textbook of Laboratory Medicine, Guyton & Hall Textbook of Medical Physiology, Schwartz's Principles of Surgery)
2. Key Chemical Stimuli and Their Receptors
Acid (H+)
- Detected primarily by S cells in the duodenum when pH drops below 4.5-5.0
- Triggers secretin release → pancreatic bicarbonate secretion to neutralize the acid
- Secretin release is proportional to acid load below pH 4.5; the major physiologic inhibitor is somatostatin
Fats (Lipids)
- Fatty acids (C10+ chain) stimulate S cells (secretin) and I cells (CCK)
- Undigested fat does NOT stimulate these cells - enzymatic breakdown to fatty acids is required
- CCK release from I cells → gallbladder contraction, pancreatic enzyme secretion, sphincter of Oddi relaxation
- Long-chain fatty acids also stimulate N cells (neurotensin) in the ileum
Proteins and Amino Acids
- Stimulate G cells (gastrin) and I cells (CCK) in the stomach/duodenum
- Protein is the most potent enteral stimulator of Pancreatic Polypeptide (PP) release
- Somatostatin release also triggered by amino acids
Glucose
- Stimulates K cells (GIP release) → insulin secretion (incretin effect)
- Also stimulates L cells (GLP-1 release) → enhances insulin secretion, reduces gastric emptying
- In the gut lumen, glucose causes release of GLP-2 which then activates submucosal neurons to upregulate SGLT1 glucose transporters
3. Intrinsic Primary Afferent Neurons (IPANs) as Chemoreceptors
IPANs (Dogiel type II / AH neurons) are the intrinsic chemosensory neurons of the enteric nervous system. They have processes that project into the mucosa and directly respond to luminal chemicals.
- Myenteric IPANs: Respond to luminal chemistry via mucosal processes and to distortion of external muscle layers
- Submucosal IPANs: Detect mechanical distortion of mucosa AND luminal chemistry
- These are the only intrinsic neurons with villus projections and are the sole mediators of mucosally derived reflexes
- Activated by serotonin (5-HT) released from EC cells in response to chemicals - this is the key transduction step between luminal content and neural activation
- Cell bodies of chemoreceptor IPANs are in submucosal ganglia; stretch-responsive IPANs are in myenteric ganglia
(Source: Yamada's Textbook of Gastroenterology, 7th ed., p. 279-280)
4. Extrinsic Chemoreceptive Pathways
| Pathway | Cell Bodies | Function |
|---|---|---|
| Vagal afferents | Nodose (vagal) ganglia | Physiological state monitoring - nutrient sensing, satiety signals (CCK acts on vagal terminals) |
| Spinal afferents | Dorsal root ganglia | Pain/discomfort conduction; collaterals in prevertebral sympathetic ganglia |
| Intestinofugal neurons | Gut wall | Second-order neurons in pathways to prevertebral ganglia |
5. Paracrine/Neurocrine Chemoreceptor Mediators
Beyond classic endocrine hormones, the mucosa uses local signaling:
| Mediator | Source | Stimulus | Action |
|---|---|---|---|
| Somatostatin | D cells (diffuse) | Fat, protein, acid, glucose, CCK | Inhibits gastrin, acid secretion, other GI hormones |
| Histamine | ECL cells / mast cells | Gastrin, ACh | Stimulates gastric acid via H2 receptors |
| Bombesin/GRP | Gastric nerve endings | Vagal stimulation | Stimulates gastrin release from G cells |
| 5-HT (serotonin) | EC cells | Mechanical + chemical stimuli | Activates IPANs and vagal afferents - key transducer |
Summary: Stimulus-Response Map
Acid (pH <4.5) → S cells → Secretin → Pancreatic HCO3⁻
Fat/Amino acids → I cells → CCK → Gallbladder contraction + Pancreatic enzymes
Glucose/Fat → K cells → GIP → Insulin (incretin)
Glucose/Fat/Protein → L cells → GLP-1/PYY → Satiety + ↓ gastric emptying
Protein/distension → G cells → Gastrin → Gastric acid
Fasting/empty stomach → X cells → Ghrelin → Hunger/GH release
Fat/Protein/Acid/Glucose → D cells → Somatostatin → Inhibits all GI secretion
Luminal chemicals → EC cells → 5-HT → Activates IPAN/vagal chemoreceptors
- Guyton and Hall Textbook of Medical Physiology, p. 807
- Tietz Textbook of Laboratory Medicine, 7th ed., p. 2067
- Yamada's Textbook of Gastroenterology, 7th ed., p. 279-280
- Histology: A Text and Atlas, p. 1552-1554
- Schwartz's Principles of Surgery, 11th ed.
Menstrual cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have excellent textbook content and two high-quality diagrams. Let me compose the full answer.
The Menstrual Cycle
The menstrual cycle is a series of coordinated, cyclic hormonal and structural changes in the female reproductive system designed to prepare the uterus for potential implantation of an embryo. The average cycle is 28 days (normal range: 21-35 days), with 2-6 days of flow and average blood loss of 20-60 mL.
The cycle involves four anatomical levels operating in concert: the hypothalamus, anterior pituitary, ovary, and uterus (endometrium).
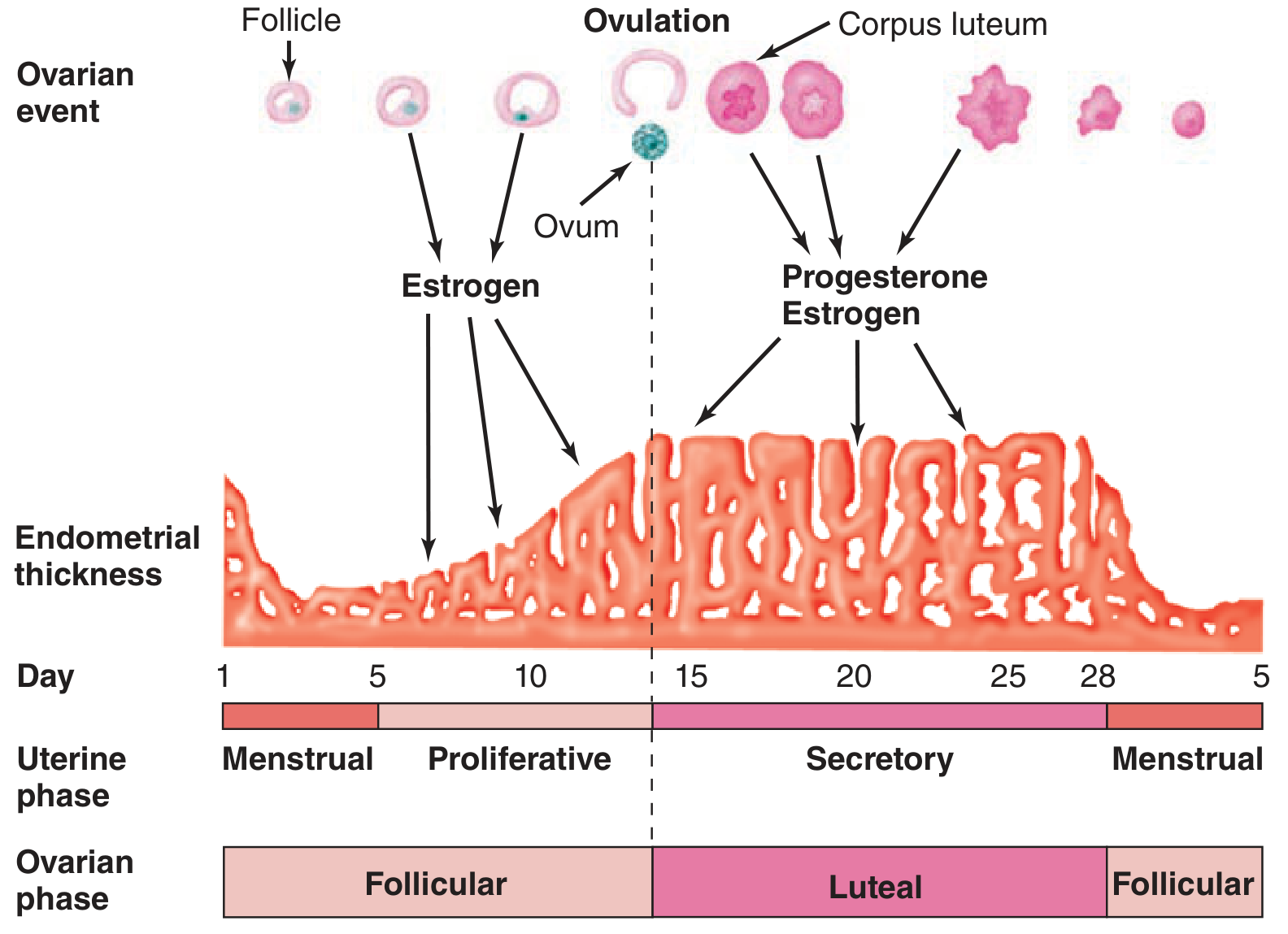
Overall Framework: Two Parallel Cycles
| Ovarian Cycle | Uterine Cycle | |
|---|---|---|
| Phase 1 | Follicular phase (Day 1-14) | Menstrual + Proliferative phase |
| Phase 2 | Luteal phase (Day 15-28) | Secretory phase |
Hormonal Control: The HPO Axis
The hypothalamic-pituitary-ovarian (HPO) axis drives the entire cycle.
Hypothalamus - GnRH
- The arcuate nucleus of the hypothalamus secretes GnRH (gonadotropin-releasing hormone), a decapeptide, in a pulsatile fashion
- Pulsatile release is essential - continuous GnRH causes downregulation of pituitary GnRH receptors and suppresses gonadotropin secretion
- GnRH half-life is only 2-4 minutes (rapidly cleaved by proteolysis)
- Pulse frequency varies across the cycle:
- Follicular phase: frequent, small-amplitude pulses
- Late follicular phase: increased frequency and amplitude
- Luteal phase: progressive lengthening of pulse intervals; higher amplitude but declining
- Decreasing pulse frequency → preferentially increases FSH over LH (important for FSH availability in late luteal/early follicular transition)
Anterior Pituitary - FSH and LH
- GnRH stimulates secretion of both FSH (follicle-stimulating hormone) and LH (luteinizing hormone) from gonadotrophs
- Their relative secretion is determined by GnRH pulse frequency and feedback from ovarian steroids and peptides
Phase 1: Follicular Phase (Days 1-14)
Ovarian Events
Early follicular (Days 1-5):
- FSH rises (due to loss of negative feedback from the regressed corpus luteum)
- FSH recruits a cohort of antral follicles
- Each follicle develops: granulosa cells (FSH-responsive) + theca interna cells (LH-responsive)
Follicle development stages:
| Stage | Size | Key Feature |
|---|---|---|
| Primordial | 0.03-0.05 mm | Primary oocyte + one layer of flattened granulosa cells |
| Primary | ~0.1 mm | Cuboidal granulosa cells; zona pellucida forms; FSH receptors develop |
| Secondary | ~0.2 mm | Multiple layers of granulosa; theca cells form with LH receptors; vascularized |
| Tertiary (antral) | 0.2-20 mm | Antrum forms; theca interna/externa differentiation; gonadotropin-dependent |
| Preovulatory (Graafian) | >20 mm | Final maturation; meiosis I completed → secondary oocyte arrested at meiosis II |
Two-cell, two-gonadotropin model:
- Theca cells (LH) → produce androgens (androstenedione, testosterone)
- Granulosa cells (FSH) → aromatize androgens → estradiol (E2)
Dominant follicle selection (around Day 6):
- One follicle outgrows the rest, probably because of superior ability to produce intrafollicular estrogen
- Non-dominant follicles undergo atresia (apoptosis)
- The dominant follicle produces increasing amounts of estradiol
Late follicular (Days 10-13):
- Rising estradiol initially exerts negative feedback on FSH and LH
- As estradiol rises above ~200 pg/mL and is sustained for >36 hours, it switches to positive feedback - triggering the LH surge
- Estradiol also stimulates endometrial proliferation
The LH Surge and Ovulation (Day 14)
- Midcycle LH surge triggers ovulation approximately 9 hours after the LH peak
- The LH surge:
- Resumes meiosis I in the oocyte
- Causes follicular rupture
- Initiates luteinization of granulosa cells
- A smaller FSH surge occurs simultaneously (mechanism not fully clear)
- The extruded ovum is picked up by the fimbriated ends of the fallopian tube
- Minor peritoneal bleeding may cause "mittelschmerz" (midcycle pain)
Phase 2: Luteal Phase (Days 15-28)
Corpus Luteum Formation
- After rupture, the follicle fills with blood (corpus hemorrhagicum)
- Granulosa and theca cells rapidly proliferate, filling with lipid-rich material → corpus luteum (yellow body)
- VEGF (vascular endothelial growth factor) supports its vascular development
- Corpus luteum secretes progesterone (dominant) + estrogen
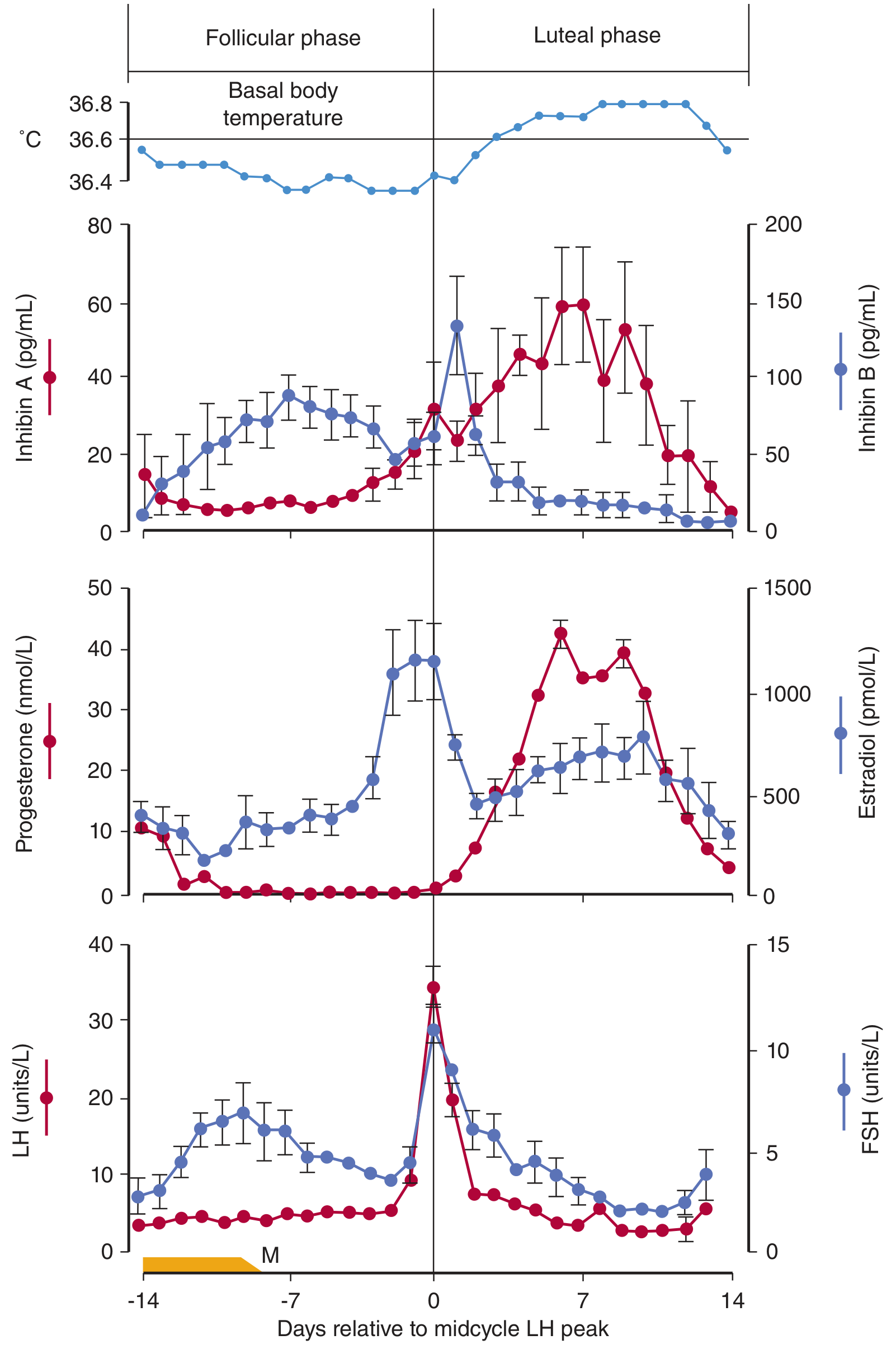
Hormone Changes
- Progesterone: rises sharply after ovulation, peaks mid-luteal phase (~Day 21)
- Estradiol: second smaller peak in mid-luteal phase
- Inhibin A: rises in luteal phase (from corpus luteum), suppresses FSH
- Inhibin B: high in follicular phase (from granulosa cells), falls after ovulation
Luteolysis (if no pregnancy)
- Without hCG from a conceptus, the corpus luteum regresses around Day 25-26
- Progesterone and estrogen fall sharply → loss of negative feedback → FSH begins to rise again, initiating the next cycle
- The regressed corpus luteum becomes the fibrous corpus albicans
Uterine (Endometrial) Cycle
The endometrium has two layers:
- Stratum functionale (superficial 2/3): shed at menstruation; supplied by spiral arteries
- Stratum basale (deep layer): not shed; regenerates the functionale; supplied by straight basilar arteries
Menstrual Phase (Days 1-4)
- Corpus luteum regresses → estrogen and progesterone fall
- Endometrium thins → spiral arteries become more coiled
- Foci of necrosis form and coalesce
- Vasospasm of spiral arteries (mediated by locally released prostaglandins, especially PGF2α) leads to ischemia, necrosis, and shedding
- Menstrual blood: ~75% arterial, ~25% venous; contains tissue debris, prostaglandins, and fibrinolysin (which prevents clotting of menstrual flow)
Proliferative Phase (Days 5-14) - driven by Estrogen
- Endometrium regenerates rapidly from stratum basale
- Thickness increases from Day 5 to 14
- Uterine glands elongate but remain straight and non-secretory
- Stroma is dense; spiral arteries lengthen
Secretory Phase (Days 15-28) - driven by Progesterone + Estrogen
- Endometrium becomes highly vascularized and edematous
- Glands become coiled, tortuous, and begin secreting clear glycogen-rich fluid ("subnuclear vacuoles" on histology - earliest sign)
- Progesterone's effects are antagonistic to estrogen - it limits further proliferation
- Ideal environment created for implantation (window of implantation: Days 20-24)
- Late secretory endometrium also produces prolactin (function unknown)
- If fertilization occurs → trophoblast produces hCG → rescues corpus luteum → cycle is interrupted
Key Feedback Mechanisms Summary
| Hormone | Source | Feedback Effect |
|---|---|---|
| Low Estradiol | Ovarian follicle | Negative feedback on FSH/LH |
| High Estradiol (>200 pg/mL, sustained) | Dominant follicle | Positive feedback → LH surge |
| Progesterone (luteal) | Corpus luteum | Negative feedback on LH/FSH |
| Inhibin A | Corpus luteum | Suppresses FSH (luteal phase) |
| Inhibin B | Granulosa cells | Suppresses FSH (follicular phase) |
| GnRH downregulation | Continuous exposure | Loss of LH/FSH secretion |
Indicators of Ovulation
- LH surge (urine/serum testing) - most reliable clinical marker
- Basal body temperature (BBT): rises 0.2-0.5°C starting 1-2 days after ovulation due to the thermogenic effect of progesterone; must be taken before rising in the morning
- Cervical mucus: changes from thick/tacky → thin, watery, "spinnbarkeit" (stretchy) at ovulation under estrogen influence
- Mittelschmerz: unilateral lower abdominal pain at time of follicular rupture
Fertile Window
- The ovum is fertilizable for a much shorter time than it survives (~72 h post-ovulation)
- Highest pregnancy rates come from intercourse in the 48 hours before ovulation
- Sperm can survive in the female genital tract for up to 120 hours before ovulation and still fertilize an egg
(Sources: Berek & Novak's Gynecology, p. 264-288; Ganong's Review of Medical Physiology, 26th ed., p. 404-408; Tietz Textbook of Laboratory Medicine, 7th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.