Infective endocarditis in detail
Reading File
Finding Sources
Searching PubMed
"infective endocarditis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the full detailed answer on infective endocarditis.
Infective Endocarditis - A Comprehensive Overview
Definition
Infective endocarditis (IE) is a microbial infection - predominantly bacterial - of the endocardial surface of the heart, most commonly affecting the cardiac valves. It results in the formation of vegetations composed of thrombotic debris, fibrin, inflammatory cells, and organisms, often associated with destruction of underlying cardiac tissue. The aorta, aneurysms, other blood vessels, prosthetic devices, and cardiovascular implantable electronic devices (CIEDs) may also be infected.
- Robbins & Kumar Pathologic Basis of Disease
- Goldman-Cecil Medicine
Classification
IE is classically divided by clinical tempo and microbial virulence:
| Feature | Acute IE | Subacute IE |
|---|---|---|
| Onset | Days | Weeks to months |
| Virulence | High (e.g., S. aureus) | Low (e.g., viridans streptococci) |
| Valve involved | Previously normal or abnormal | Previously abnormal (e.g., rheumatic) |
| Destruction | Severe, rapid | Less destructive |
| Cure | Often requires surgery | Often cured with antibiotics alone |
| Mortality | High | Lower |
Modern classification is based on the causative organism, involved valve, and pace of disease rather than strict acute/subacute dichotomy.
Epidemiology
-
Incidence: approximately 13.8 per 100,000 (range 5.7-35.8 per 100,000)
-
In the United States: 10,000-20,000 new cases per year; approximately 1 case per 1,000 hospital admissions
-
In-hospital mortality: up to 22%; 5-year mortality: up to 40%
-
Deaths due to IE have increased 131% since 1990 (an estimated 66,322 deaths globally as of 2019)
-
The opioid epidemic has dramatically increased IV drug-associated IE, particularly S. aureus right-sided disease
-
Contemporary IE is most often an acute disease caused by S. aureus, involving the mitral valve (41.1%) and aortic valve (37.6%)
-
Common complications: stroke (16.9%), embolization (22.6%), heart failure (32.3%), intracardiac abscess (14.4%); 48.2% require surgery
-
Fuster and Hurst's The Heart, 15th Edition
-
Braunwald's Heart Disease
Predisposing Conditions
More common:
- Mitral valve prolapse (especially with regurgitation)
- Degenerative valvular disease / myxomatous degeneration
- Injection drug use
- Congenital heart disease (e.g., VSD, bicuspid aortic valve)
- Previous IE
- Prosthetic heart valves
- Chronic hemodialysis / intravascular devices
Less common:
-
Rheumatic heart disease (historically the most common, now declining in developed countries)
-
Idiopathic hypertrophic subaortic stenosis
-
Coarctation of the aorta
-
Goldman-Cecil Medicine
Microbiology
| Organism | Context / Notes |
|---|---|
| Viridans group streptococci | 50-60% of native abnormal valve IE; oral flora; dental procedures |
| Staphylococcus aureus | Most common overall; infects normal or abnormal valves; IV drug use, nosocomial; worst prognosis |
| Enterococci | ~10% of cases; often GI/GU source; E. faecalis |
| HACEK group (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella) | 5-10% community-acquired; fastidious gram-negatives; oral flora |
| Coagulase-negative staphylococci (S. epidermidis) | Early prosthetic valve IE (within 1-2 months of surgery); skin flora |
| *Streptococcus gallolyticus (formerly S. bovis) | Associated with colorectal polyps/cancer - warrants colonoscopy |
| Fungi (Candida, Aspergillus) | Rare; immunocompromised, prosthetic valves, IV drug users; very poor prognosis |
| Culture-negative IE | ~10% of cases; reasons: prior antibiotics, Coxiella burnetii (Q fever), Bartonella, Brucella, HACEK |
- Robbins & Kumar
- Washington Manual of Medical Therapeutics
Pathogenesis
The sequence of IE development:
- Endothelial damage - turbulent blood flow (from valvular abnormalities, jets of regurgitation, congenital defects) disrupts the endothelium
- Non-bacterial thrombotic endocarditis (NBTE) - sterile platelet-fibrin thrombus forms on damaged endothelium
- Bacteremia - organisms enter the bloodstream (dental procedures, skin breaks, IV drug use, GI/GU procedures, gut/oral/skin epithelial barriers)
- Colonization - organisms adhere to NBTE via surface adhesins (e.g., fibronectin-binding proteins in S. aureus)
- Vegetation formation - organisms proliferate, recruit more fibrin and platelets, and embed deeply in a protected nidus inaccessible to host defenses and poorly penetrated by antibiotics
- Local destruction and embolization - vegetations erode valve leaflets, chordae, annulus; fragments embolize systemically
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Morphology / Pathology
Vegetations are the hallmark: friable, bulky, irregular masses containing fibrin, inflammatory cells, and organisms.
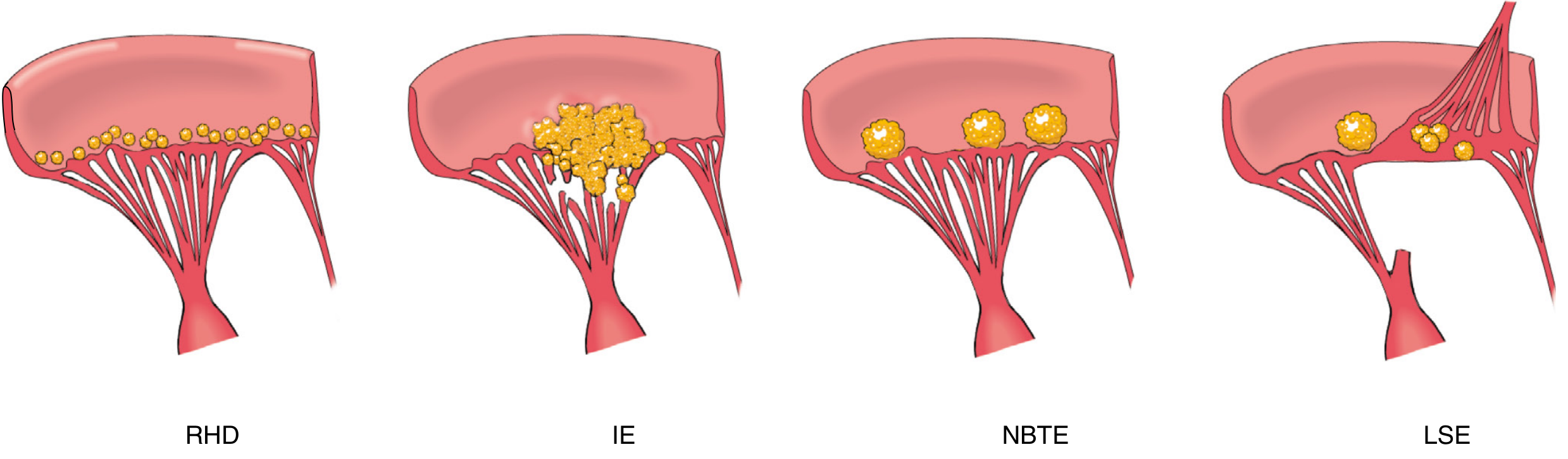
Comparison of RHD, IE, NBTE, and Libman-Sacks endocarditis vegetations. IE shows the largest, most destructive vegetations extending onto chordae. (Robbins & Kumar)
- Most common sites: aortic and mitral valves (left-sided); right-sided (tricuspid, pulmonic) in IV drug users
- Vegetations can be single or multiple; may involve more than one valve
- Can erode into the myocardium causing ring abscess (perivalvular abscess)
- Embolization of infected fragments causes septic infarcts or mycotic aneurysms
- Subacute IE: less valvular destruction; granulation tissue may form
- Acute IE: neutrophilic infiltration, necrosis, greater destruction
Clinical Features
Symptoms
- Fever (most common, >90%) - may be absent in elderly, immunocompromised, or with prior antibiotics
- Constitutional: fatigue, malaise, night sweats, weight loss, arthralgias
- Symptoms of heart failure (dyspnea, orthopnea) if significant valve destruction
- Back/musculoskeletal pain
- Neurologic symptoms (stroke, confusion, seizures)
Signs
Cardiac:
- New or changing heart murmur (new regurgitant murmur in most cases of left-sided IE)
- Signs of heart failure
Peripheral / Embolic / Immune ("peripheral stigmata"):
These occur in <15% of cases (often not present unless infection is advanced):
| Sign | Description | Mechanism |
|---|---|---|
| Janeway lesions | Painless, erythematous/hemorrhagic flat macules on palms and soles | Septic microemboli |
| Osler nodes | Painful, tender, red nodules on fingertip pulp (lasting days-weeks) | Immune complex deposition + microemboli; involves glomus bodies |
| Splinter hemorrhages | Linear dark streaks under fingernails | Microemboli |
| Roth spots | Oval retinal hemorrhages with a pale center | Microemboli (retinal); immune complex |
| Petechiae | Conjunctivae, palate, skin | Microemboli |
| Clubbing | In chronic/subacute IE | |
| Splenomegaly | Especially subacute IE |

Splinter hemorrhages in a patient with infective endocarditis. (Fitzpatrick's Dermatology)
In IV drug users (right-sided IE):
-
Fever, cough, pleuritic chest pain, hemoptysis
-
Multiple pulmonary opacities (septic pulmonary emboli) on CXR/CT
-
Right-sided murmur varying with respiration
-
Pyuria (22%) and hematuria (35%) from immune complex glomerulonephritis
-
Tintinalli's Emergency Medicine
-
Fitzpatrick's Dermatology
Complications
| Complication | Notes |
|---|---|
| Cardiac | Valve destruction, acute regurgitation, HF, perivalvular abscess (ring abscess), conduction abnormalities (new heart block from septal involvement), fistula formation, pericarditis |
| Embolic | Stroke (16.9%), peripheral arterial embolism, splenic/renal infarction, mesenteric ischemia, limb ischemia |
| Neurologic | Ischemic stroke, intracranial hemorrhage, mycotic aneurysm, cerebral abscess, meningitis, encephalopathy (22-40%) |
| Renal | Immune complex glomerulonephritis, embolic renal infarction, acute kidney injury (also from antibiotics) |
| Metastatic infection | Septic emboli to lung (right-sided), joints (septic arthritis), vertebral osteomyelitis, psoas abscess |
| Mycotic aneurysms | Infected emboli seed arterial walls; intracranial aneurysms risk rupture and hemorrhage |
Diagnosis
Modified Duke Criteria (Updated 2023 - Duke-ISCVID)
Definite IE = 2 Major, OR 1 Major + 3 Minor, OR 5 Minor criteria
Possible IE = 1 Major + 1 Minor, OR 3 Minor criteria
Rejected = Firm alternative diagnosis, resolution with antibiotics ≤4 days, or surgery/autopsy after ≤4 days shows no IE
Possible IE = 1 Major + 1 Minor, OR 3 Minor criteria
Rejected = Firm alternative diagnosis, resolution with antibiotics ≤4 days, or surgery/autopsy after ≤4 days shows no IE
Major Criteria
1. Microbiologic:
- ≥2 separate blood culture sets positive for typical organisms: S. aureus, S. lugdunensis, E. faecalis, all streptococcal species (except S. pneumoniae and S. pyogenes), Granulicatella, Abiotrophia, Gemella, HACEK organisms
- ≥2 blood cultures drawn >12 hours apart, OR ≥3 of ≥4 separate cultures (first and last drawn ≥1 hour apart)
- Single positive blood culture for Coxiella burnetii (Q fever) OR anti-phase I IgG titer ≥1:800
2. Evidence of endocardial involvement:
- Echocardiographic: oscillating intracardiac mass on valve or supporting structure in path of regurgitant jet, OR abscess, OR new partial dehiscence of prosthetic valve
- New valvular regurgitation (change in pre-existing murmur is NOT sufficient)
- FDG-PET/CT or radiolabeled leukocyte SPECT/CT - equivalent to echo (new in 2023)
Minor Criteria
- Predisposing heart condition or IV drug use
- Fever ≥38°C
- Vascular phenomena: arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial/conjunctival hemorrhage, Janeway lesions
- Immunologic phenomena: glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Microbiologic evidence: positive blood culture not meeting major criteria OR serologic evidence of active infection with organism consistent with IE
- Braunwald's Heart Disease
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
Blood Cultures
- Collect 3 sets from separate venipuncture sites, ideally before antibiotics
- Each set: paired aerobic and anaerobic bottles (10 mL per bottle)
- At least 1 hour between first and last collection
- If negative at 48-72 hours, obtain 2-3 more sets and consult microbiology for special culture techniques (PCR, serology for Coxiella, Bartonella)
- Prior antibiotics are the #1 cause of culture-negative endocarditis
Echocardiography
| Modality | Use |
|---|---|
| TTE (Transthoracic Echo) | First-line in most patients; sensitivity ~60-70% for vegetations |
| TEE (Transesophageal Echo) | Preferred when: TTE is inadequate/negative with high suspicion; prosthetic valves; complicated IE (abscess suspected); S. aureus bacteremia; aortic IE |
TEE has sensitivity >90% for vegetations, perivalvular abscesses, and fistulae.
TEE is mandatory in prosthetic valve endocarditis and for detecting perivalvular complications.
- Braunwald's Heart Disease
Other Investigations
- CBC: leukocytosis (acute IE), normochromic normocytic anemia (subacute)
- Elevated ESR, CRP, rheumatoid factor, circulating immune complexes
- Urinalysis: hematuria, proteinuria, red cell casts (glomerulonephritis)
- Creatinine (renal involvement or antibiotic nephrotoxicity monitoring)
- ECG: new PR prolongation or heart block suggests perivalvular extension
- CXR / CT chest: septic emboli in right-sided IE
- Brain MRI: cerebral emboli, abscess, mycotic aneurysm
- CT angiography: mycotic aneurysm screening
Treatment
General Principles
- Bactericidal drugs are required (not bacteriostatic) - organisms are protected deep within vegetations with high bacterial burden (10⁸-10¹⁰ CFU/g)
- Prolonged parenteral courses needed (4-6 weeks for most; 2 weeks in selected uncomplicated cases)
- Multidisciplinary team: Infectious disease, cardiology, cardiac surgery (+ neurology if neurologic complications)
- All patients should be managed inpatient at a center with IE expertise
Antibiotic Regimens by Organism
Viridans Group Streptococci / S. gallolyticus (penicillin-susceptible, MIC ≤0.12 μg/mL)
- Penicillin G 12-18 million units/day IV × 4 weeks, OR
- Ceftriaxone 2g IV once daily × 4 weeks (equivalent; preferred for outpatient completion), OR
- Shortened 2-week regimen: Ceftriaxone + Gentamicin (for uncomplicated native valve IE in appropriate patients)
- Vancomycin × 4 weeks reserved for true penicillin allergy
Relatively resistant streptococci (MIC 0.12-0.5 μg/mL)
- Penicillin G 4 million units IV q4h × 4 weeks + Gentamicin × 2 weeks (synergy), OR
- Ceftriaxone + Gentamicin × 2 weeks
- Vancomycin for penicillin allergy
Staphylococcus aureus (native valve)
- MSSA: Nafcillin or oxacillin 2g IV q4h × 6 weeks (+ optional short-course gentamicin in first 3-5 days - no longer routinely recommended due to renal toxicity)
- MRSA or penicillin-allergic: Vancomycin 30-45 mg/kg/day IV in 2-3 divided doses × 6 weeks; OR Daptomycin 8-10 mg/kg/day IV (not for pulmonary involvement)
- TEE mandatory; early surgery evaluation
Staphylococcus aureus (prosthetic valve)
- MSSA: Nafcillin + Rifampin 300mg orally q8h × ≥6 weeks + Gentamicin × 2 weeks
- MRSA: Vancomycin + Rifampin × ≥6 weeks + Gentamicin × 2 weeks
Enterococci
- Ampicillin-sensitive: Ampicillin + Gentamicin × 4-6 weeks, OR Ampicillin + Ceftriaxone (double β-lactam synergy; preferred for aminoglycoside-resistant strains)
- Vancomycin-resistant enterococci (VRE): Linezolid or Daptomycin-based regimens
- Enterococci require synergistic combination therapy
HACEK organisms
- Ceftriaxone 2g IV once daily × 4 weeks (preferred)
- Ampicillin-sulbactam is an alternative
Culture-negative IE
-
Broad-spectrum: Ampicillin-sulbactam + Gentamicin, with coverage tailored based on clinical context and serology
-
Harrison's Principles of Internal Medicine 22e (2025)
-
Washington Manual of Medical Therapeutics
-
Jawetz, Melnick & Adelberg's Medical Microbiology
Prophylaxis (AHA 2021 Update)
Antibiotic prophylaxis (AP) before invasive dental procedures (those involving manipulation of gingival tissue, periapical region of teeth, or perforation of oral mucosa) is recommended ONLY for patients at highest risk:
- Prosthetic cardiac valve (including transcatheter-implanted)
- Previous IE
- Unrepaired cyanotic congenital heart disease
- Repaired congenital heart defect with prosthetic material (within 6 months)
- Repaired CHD with residual defect at or adjacent to prosthetic patch
- Cardiac transplant recipients with valvulopathy
- Ventricular assist devices and implantable hearts (NEW in 2021)
Regimen:
- Amoxicillin 2g orally 30-60 min before procedure (preferred)
- True penicillin allergy: Doxycycline 100mg orally (new 2021 addition; clindamycin REMOVED due to C. difficile risk)
- Cephalexin 2g, Azithromycin 500mg, or Clarithromycin 500mg are alternatives
AP is NOT recommended for GI/GU/respiratory procedures solely for IE prevention.
- Braunwald's Heart Disease
Surgical Treatment
Between 25-40% of patients with left-sided IE require cardiac surgery during active infection.
Indications (ACC/AHA 2021 Guidelines - Class I / Strong)
| Indication | Timing |
|---|---|
| Valve dysfunction resulting in heart failure | Early (during hospitalization, before completing antibiotics) |
| IE caused by S. aureus, fungi, or highly resistant organisms (left-sided) | Early |
| Heart block, annular or aortic abscess, or destructive penetrating lesions | Early |
| Persistent bacteremia or fever >5 days despite appropriate antimicrobials | Early |
| Definite IE + implanted cardiac electronic device (CIED) - complete system removal including all leads | Early |
| Prosthetic valve IE with relapsing infection | Recommended |
Class IIa / Reasonable
- Recurrent emboli + persistent vegetations despite antibiotics → Early surgery
Class IIb / May Consider
- Native left-sided IE with mobile vegetations >10 mm (with or without embolic phenomenon)
- IE with surgical indication + stroke (no intracranial hemorrhage, no severe neurological damage) → surgery without delay
- IE + major ischemic stroke + extensive damage or ICH + hemodynamically stable → delay surgery ≥4 weeks
Emergent surgery (same day)
-
Valve dysfunction with pulmonary edema or cardiogenic shock
-
Acute aortic regurgitation with pre-closure of mitral valve
-
Sinus of Valsalva abscess ruptured into right heart
-
Braunwald's Heart Disease
-
Harrison's Principles of Internal Medicine 22e (2025)
Special Scenarios
Prosthetic Valve Endocarditis (PVE)
- Early PVE (within 1-2 months of surgery): usually S. aureus, S. epidermidis, gram-negatives, fungi - from perioperative contamination
- Late PVE (>12 months): similar to native valve IE - streptococci, S. aureus, enterococci
- TEE is mandatory (TTE has poor sensitivity with prostheses)
- Requires longer antibiotic courses (≥6 weeks); rifampin added for staphylococcal PVE
- Higher surgical rates than native valve IE
IV Drug Users (IVDU)
- Predominantly right-sided (tricuspid valve 55-94% of cases)
- Organism: S. aureus in >50%
- Chest X-ray shows multiple bilateral pulmonary opacities (septic emboli)
- Tricuspid valve IE: often curable with antibiotics alone (right-sided good prognosis without surgery)
- Recurrence is common with continued drug use; addiction medicine consultation is required before repeat surgical intervention
CIED-IE (Cardiac Implantable Electronic Device)
- Pacemakers, ICDs
- Complete system removal (generator + all leads) is Class I indication
- Medical therapy alone rarely curative
Culture-Negative IE
- ~10% of cases
- Causes: prior antibiotics (most common), fastidious organisms (Coxiella, Bartonella, Brucella, Tropheryma whipplei, HACEK)
- Workup: extended cultures, Coxiella serology, Bartonella serology/PCR, excised valve tissue 16S rRNA PCR, FDG-PET/CT
Prognosis and Outcome
Predictors of poor prognosis:
- S. aureus infection
- Perivalvular abscess
- Prosthetic valve involvement
- Heart failure
- Neurologic complications
- Left-sided disease
- Fungal endocarditis
In-hospital mortality: ~15-25% overall; up to 50% for complicated or S. aureus PVE.
Valve surgery during index hospitalization (when indicated) conveys a 27-55% survival benefit, greatest among those with pressing indications.
- Fuster and Hurst's The Heart, 15th Edition
- Harrison's Principles of Internal Medicine 22e (2025)
Key References:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease
- Braunwald's Heart Disease, 2-Vol Set (Baddour, Anavekar et al.)
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Fuster and Hurst's The Heart, 15th Edition
- Goldman-Cecil Medicine
- Washington Manual of Medical Therapeutics
- AHA Scientific Statement 2021 (Prevention); AHA 2015 (Diagnosis and Management); ACC/AHA 2021 Valvular Heart Disease Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.