Management of angina
Reading File
Finding Sources
Searching PubMed
"stable angina" AND management
Finding Sources
Reading Article
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive content from multiple authoritative textbooks plus the management flowcharts. Here is the full synthesized response:
Management of Angina
Angina is chest pain or discomfort caused by myocardial ischemia - an imbalance between oxygen supply and demand. Management differs by type (stable, unstable, vasospastic), but for stable angina the goals are: (1) relieve symptoms and improve quality of life, and (2) reduce disease progression, MI, and death. Absolute risk reduction in MI/cardiac death is achieved primarily through medical therapy, not revascularization.
1. Lifestyle Modification
The foundation of all angina management:
- Smoking cessation - most impactful single intervention
- Regular aerobic exercise (intensity guided by stress testing)
- Weight loss and low-fat, low-cholesterol diet
- Cardiac rehabilitation programs for diet, exercise, and risk factor education
- Control of hypertension, diabetes (target HbA1c ≤7%), and dyslipidemia
2. Medical Therapy
Anti-ischemic / Antianginal Agents
Beta-Blockers (First-line)
Beta-blockers prevent catecholamine binding to beta-adrenergic receptors, reducing heart rate, myocardial contractility, and therefore myocardial oxygen demand. They raise the ischemic threshold and delay the onset of exertional angina.
- Titrate dose to a resting heart rate of 50-60 bpm
- All beta-blockers are roughly equally effective in stable angina
- Avoid agents with intrinsic sympathomimetic activity (ISA)
- Post-MI: reduce secondary events and sudden cardiac death
- Goldman-Cecil Medicine, p. 633
Calcium Channel Blockers (CCBs)
CCBs reduce afterload via peripheral vasodilation, lower myocardial oxygen demand, reduce coronary vascular resistance, and inhibit coronary vasospasm.
- Non-dihydropyridines (verapamil, diltiazem): also slow heart rate - preferred as monotherapy when beta-blockers are contraindicated; caution when combined with beta-blockers (risk of bradycardia)
- Dihydropyridines (amlodipine, nifedipine): greater vasodilation, better for hypertensive patients with angina; short-acting dihydropyridines can reflexly increase HR, so add a beta-blocker
- CCBs and beta-blockers are roughly equally effective in clinical trials for angina; CCBs have not been shown to reduce death or MI in stable IHD, so they serve as add-on or alternative therapy
- Vasospastic (Prinzmetal) angina: CCBs are first-line; higher doses often required
- Goldman-Cecil Medicine, p. 633
Dosing reference:
| Drug | Dose |
|---|---|
| Nifedipine LA | 30-180 mg daily |
| Amlodipine | 5-10 mg daily |
| Diltiazem SR | 120-360 mg daily |
| Verapamil SR | 120-480 mg daily |
Nitrates
Nitrates are metabolized to nitric oxide in vascular smooth muscle, causing vasodilation of coronary arteries and veins:
- Venodilation reduces preload (LV end-diastolic pressure and wall tension), decreasing subendocardial oxygen demand
- Coronary vasodilation improves blood flow
Important clinical points:
- Sublingual nitroglycerin (0.3-0.6 mg) terminates an acute attack within 2-5 min; can also be used prophylactically before exertion
- Long-acting nitrates (isosorbide di/mononitrate, transdermal patches) prevent angina and improve exercise tolerance
- A nitrate-free interval of 8-12 hours daily is mandatory to prevent tolerance/tachyphylaxis
- Absolute contraindication: concurrent use of PDE-5 inhibitors (sildenafil, tadalafil, vardenafil) - marked and prolonged hypotension
- Long-acting nitrates are typically used as a second or third agent alongside beta-blockers/CCBs
- Goldman-Cecil Medicine, p. 634
Nitrate preparations:
| Preparation | Dose | Onset | Duration |
|---|---|---|---|
| Sublingual NTG | 0.3-0.6 mg PRN | 2-5 min | 10-30 min |
| Aerosol NTG | 0.4 mg PRN | 2-5 min | 10-30 min |
| Isosorbide dinitrate | 5-40 mg tid | 30-60 min | 4-6 h |
| Isosorbide mononitrate | 10-20 mg bid | 30-60 min | 6-8 h |
| Isosorbide mononitrate SR | 30-120 mg daily | 30-60 min | 12-18 h |
| Transdermal NTG patch | 5-15 mg daily | >60 min | 12 h |
| IV nitroglycerin | 10-200 mcg/min | <2 min | During infusion |
Ranolazine
Inhibits the late inward sodium current, reducing intracellular calcium overload. It decreases angina and improves exercise tolerance without lowering blood pressure or heart rate - making it useful when hemodynamics limit uptitration of other agents. Used in combination with a beta-blocker for refractory symptoms.
Disease-Modifying Agents (Reduce MI and Death)
| Agent | Indication / Role |
|---|---|
| Aspirin 81 mg daily | All patients with stable angina (absent contraindication); low-dose as effective as 325 mg with better adherence |
| Clopidogrel 75 mg | Alternative if aspirin intolerant; mandatory after PCI with stents |
| Low-dose rivaroxaban 2.5 mg bid + aspirin | Superior to aspirin alone for CV death/MI/stroke in stable CAD, but with more bleeding |
| High-intensity statin | All patients; reduces LDL and stabilizes plaque |
| ACE inhibitor / ARB | High-risk patients (diabetes, HF, LVEF <40%, vascular disease); reduces CV mortality and events |
| BP control | Target <130/80 mmHg |
| Glycemic control | HbA1c target ≤7%; refer to specialist if not achieved |
Goldman-Cecil Medicine, p. 632-633; Washington Manual, p. 125-126
3. Management Flowchart
Stable Angina - Evaluation and Treatment Strategy
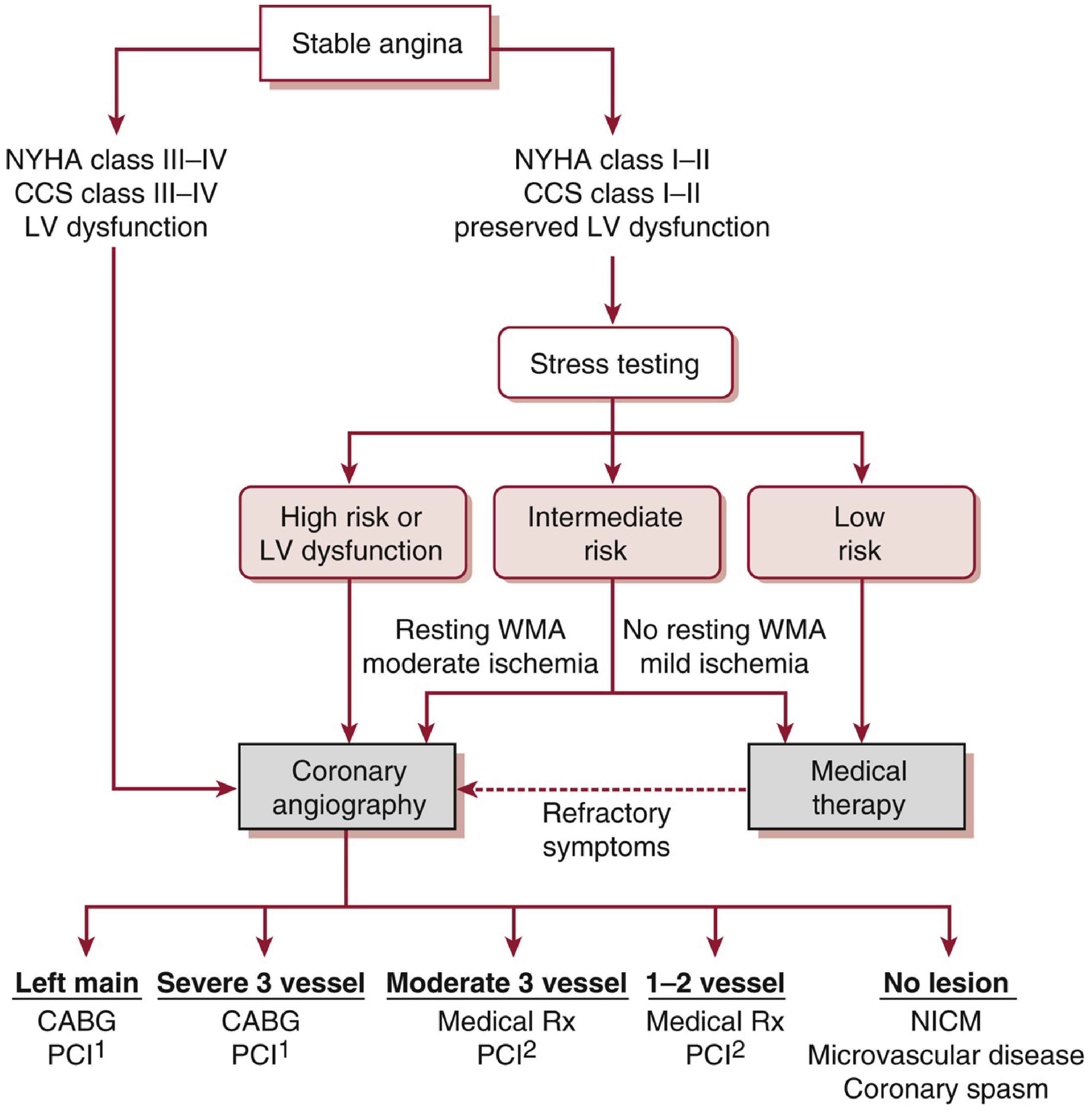
Figure: Approach to stable ischemic heart disease based on the ISCHEMIA trial. Patients with severe limiting angina, clinical HF, or LV dysfunction go directly to coronary angiography. Others undergo medical optimization with GDMT first. (Washington Manual of Medical Therapeutics)
Lifestyle and Pharmacotherapy Algorithm
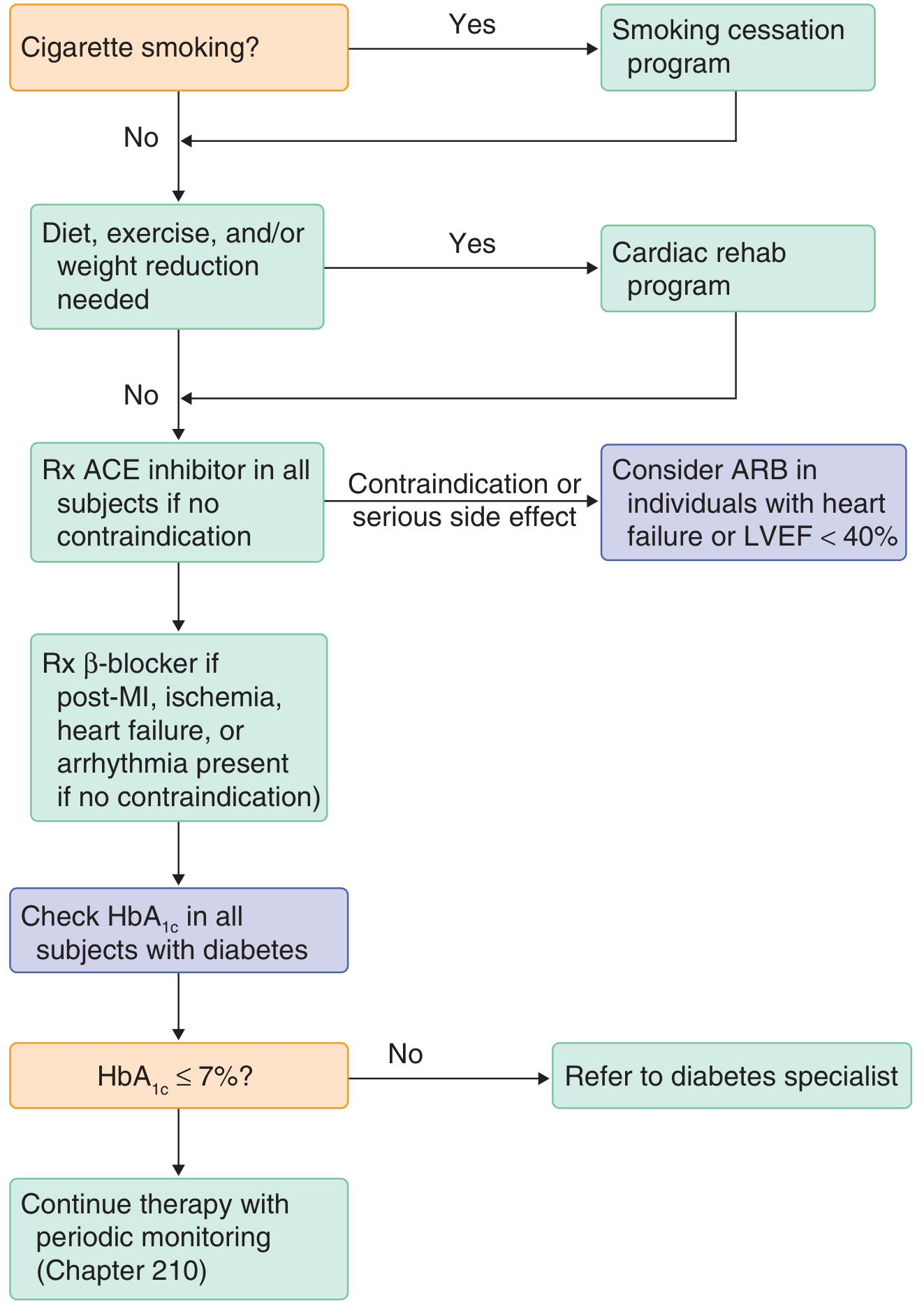
Figure: Stepwise approach - smoking cessation → lifestyle/cardiac rehab → ACE inhibitor → beta-blocker → glycemic control. (Goldman-Cecil Medicine)
4. Coronary Revascularization
Medical therapy with at least two classes of antianginal agents should be tried before revascularization is considered a failure in stable angina.
Key principle from COURAGE, BARI 2D, and ISCHEMIA trials: PCI improves anginal symptoms but does not reduce risk of death, MI, or major cardiovascular events compared to optimal medical therapy as an initial strategy in stable IHD - including patients with diabetes or chronic total occlusions.
PCI vs CABG Decision
| Anatomic Situation | Preferred Strategy |
|---|---|
| Left main disease (>50% stenosis) | CABG preferred; PCI if poor surgical candidate (STS >5%) + low SYNTAX score |
| 3-vessel severe disease | CABG |
| 3-vessel moderate disease | Medical Rx or PCI² |
| Multivessel disease + diabetes | CABG (if LIMA to LAD possible); PCI if SYNTAX <22 |
| 2-vessel + proximal LAD disease | CABG |
| 1-2 vessel disease, low risk | Medical therapy; PCI only for refractory symptoms or significant ischemia |
| Recurrent angina post-CABG | PCI (avoids repeat CABG morbidity) |
SYNTAX Score: validated angiographic model; low/intermediate scores favor PCI outcomes comparable to CABG.
Graft patency: internal mammary artery ~90% at 10 years; saphenous vein graft 40-50% at 10 years; radial artery ~80% at 5 years. After 10 years, ~50% of patients develop recurrent angina.
- Goldman-Cecil Medicine, p. 634; Washington Manual, p. 129
5. Unstable Angina
Unstable angina (new onset, rest angina, crescendo pattern) requires urgent management:
- Immediate ASA (first drug given)
- Nitrates for pain relief (sublingual or IV)
- Beta-blockers (IV esmolol if safety uncertain)
- Anticoagulation (heparin)
- Early invasive strategy (coronary angiography + PCI) for high-risk features (elevated troponin, dynamic ECG changes, hemodynamic instability, GRACE score >140)
- Dual antiplatelet therapy (aspirin + P2Y12 inhibitor: clopidogrel, prasugrel, or ticagrelor)
- Rosen's Emergency Medicine
6. Vasospastic (Prinzmetal) Angina
Characterized by rest angina with transient ST elevation, often in the early morning. Associated with heavy smoking, migraine, and Raynaud phenomenon.
- Acute attack: sublingual nitroglycerin within minutes
- Prevention (first-line): calcium channel blockers (often at higher doses)
- Adjuncts: long-acting nitrates combined with CCBs; statins, magnesium, alpha-blockers may help
- Avoid: beta-blockers (can worsen spasm); smoking cessation essential
- Fuster & Hurst's The Heart, 15th ed., p. 637
7. Refractory Angina
For patients failing maximal medical therapy who are not revascularization candidates, options include:
- Coronary sinus reducer (Reducer device) - a 2025 systematic review/meta-analysis (PMID: 40684096) confirms efficacy and safety in refractory angina
- Enhanced external counterpulsation (EECP)
- Spinal cord stimulation
- Transmyocardial revascularization
Summary Table
| Category | Agent | Main Role |
|---|---|---|
| First-line antianginal | Beta-blocker | Reduce O₂ demand, HR, workload |
| Alternative / Add-on | CCB (non-DHP) | HR control + vasodilation |
| Vasodilation | CCB (DHP) | Vasodilation, hypertensive patients |
| Acute relief + prevention | Nitrates | Preload reduction + coronary dilation |
| Refractory angina | Ranolazine | No hemodynamic effect |
| Anti-thrombotic | Aspirin 81 mg | Plaque stabilization, reduce MI |
| Plaque stabilization | High-intensity statin | LDL lowering, plaque regression |
| High-risk patients | ACE inhibitor / ARB | CV mortality reduction |
| Post-PCI / ACS | DAPT (ASA + P2Y12) | Stent thrombosis prevention |
Recent evidence note (2026): A meta-analysis of 28 RCTs (9,346 PCI vs. 9,503 medical patients; PMID: 41130952) confirmed PCI significantly reduces MI incidence (OR 0.84, p=0.01) but shows no difference in mortality, stroke, or freedom from angina vs. optimal medical therapy in stable angina - reinforcing that medical therapy remains the primary strategy for uncomplicated stable disease.
And management for unstable angina
Finding Sources
Searching PubMed
"unstable angina" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive response. Let me compile the full answer.
Management of Unstable Angina (UA) / NSTEMI
UA and NSTEMI are part of the acute coronary syndrome (ACS) spectrum. They are closely related - both involve partial coronary occlusion from plaque rupture, thrombus formation, or vasospasm. The key distinction: UA has no myocardial necrosis (negative biomarkers), while NSTEMI has positive troponin indicating necrosis. Management is largely the same, so guidelines typically address them together.
Epidemiology: ACS accounts for >780,000 events annually; 70% are NSTEMI/UA. At 1 year after UA/NSTEMI: ~6% mortality, ~11% recurrent MI, ~50-60% need revascularization. Long-term mortality of NSTEMI equals that of STEMI despite lower short-term mortality.
Definition of Unstable Angina
UA is defined as any of:
- Rest angina lasting >20 minutes, occurring within 1 week of presentation
- New-onset angina of at least CCS class II severity, within 2 months
- Crescendo angina - previously stable angina that worsens by ≥1 CCS class to at least class III within 2 months
Rosen's Emergency Medicine; Textbook of Family Medicine 9e, p. 676
Step 1: Immediate Assessment
On arrival to ED:
- ECG within 10 minutes of presentation (repeat every 5-10 min if pain continues)
- Cardiac biomarkers: troponin I or T (preferred; remains elevated for days); serial measurements at 0 and 3-6 hours. CK-MB is no longer the recommended primary marker
- CBC, metabolic panel, BNP, lipid profile, fasting glucose
- Chest X-ray
- Supplemental oxygen only if SpO₂ <90% or respiratory distress
ECG Patterns to Recognize
| Finding | Significance |
|---|---|
| ST depression (multiple leads) + ST elevation in aVR/V1 | Multivessel or left main disease |
| Biphasic/deeply inverted T waves V2-V4 + stuttering pain | Wellens syndrome - critical LAD stenosis |
| New LBBB | High-risk - treat as STEMI equivalent |
| ST depression in anterior leads with ST elevation inferiorly | Posterior MI |
Step 2: Risk Stratification
High-Risk Features - Prompt Urgent Angiography (<2 hours)
- Refractory/accelerating angina despite adequate medical therapy
- Hemodynamic instability or cardiogenic shock
- Signs of new HF or pulmonary edema (high Killip class)
- New or worsening mitral regurgitation
- Sustained VT or VF
- New LBBB
TIMI Risk Score (1 point each - higher = worse prognosis)
- Age >65 years
- Known CAD (stenosis >50%)
- ≥2 anginal episodes in 24 hours
- ST-segment or T-wave changes
- Elevated cardiac biomarkers
- ASA use in the last 7 days
- ≥3 CAD risk factors (family history, DM, HTN, hyperlipidemia, smoking)
GRACE score >140 = high risk; <109 = low risk.
Step 3: Acute Pharmacologic Management (MONA + Anticoagulation + DAPT)
A. Anti-ischemic Therapy
| Drug | Dose / Notes |
|---|---|
| Aspirin | 162-325 mg chewed immediately (non-enteric coated); then 81 mg daily |
| Nitrates | Sublingual NTG 0.3-0.6 mg q5min x3; IV nitroglycerin for ongoing pain or hypertension. Contraindicated with PDE-5 inhibitors and in hypotension/RV infarct |
| Beta-blockers | Oral within 24h (e.g., metoprolol 25-50 mg); IV if ongoing ischemia or severe hypertension. Titrate to HR 50-60 bpm. Avoid in acute decompensated HF, bradycardia, AV block, or bronchospasm. IV esmolol useful if safety uncertain |
| Morphine | For acute pain unresponsive to antianginal therapy; use cautiously (some evidence of harm in ACS with routine use) |
| Oxygen | Only if SpO₂ <90% |
B. Antiplatelet Therapy
Dual antiplatelet therapy (DAPT) is a cornerstone - aspirin alone provides only partial platelet inhibition (COX pathway only); P2Y12 inhibition blocks the ADP pathway.
| Drug | Loading Dose | Maintenance | Notes |
|---|---|---|---|
| Aspirin | 162-325 mg | 81 mg daily | Give to all patients immediately |
| Clopidogrel | 600 mg | 75 mg daily | Preferred if CABG possible (stop 5 days pre-CABG) |
| Ticagrelor | 180 mg | 90 mg twice daily | More potent, faster onset; preferred over clopidogrel in most ACS (if no contraindication) |
| Prasugrel | 60 mg | 10 mg daily | Most potent P2Y12 inhibitor; contraindicated in prior stroke/TIA; avoid in age >75, weight <60 kg |
After 600 mg clopidogrel load, steady-state platelet inhibition reached in 2-3 hours (vs. days with 75 mg daily dosing).
GP IIb/IIIa inhibitors (tirofiban, eptifibatide): Consider in patients with high-risk features, ongoing ischemia, or delay to revascularization. Not used if bivalirudin is chosen as anticoagulant (except bail-out). Textbook of Family Medicine 9e, p. 677
C. Anticoagulation
Both UFH and LMWH have Level A evidence. LMWH (enoxaparin) is generally preferred in patients managed conservatively due to more predictable pharmacokinetics, resistance to platelet factor 4, lower HIT risk, and greater anti-Xa activity.
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Enoxaparin (LMWH) | 1 mg/kg SC twice daily | SC | Preferred in conservative strategy; ESSENCE trial: superior to UFH for death/MI/recurrent angina at 1 month |
| UFH | 70 units/kg bolus IV, then ~1000 units/hr | IV | Adjust to aPTT; preferred if urgent CABG planned or if creatinine clearance <30 mL/min |
| Bivalirudin | Weight-based IV infusion | IV | Direct thrombin inhibitor; alternative to UFH + GP IIb/IIIa at time of PCI; lower bleeding risk |
| Fondaparinux | 2.5 mg SC daily | SC | Lower bleeding risk; avoid if eGFR <30 |
D. Statins
Start high-intensity statin immediately regardless of baseline LDL. In-hospital initiation improves long-term compliance.
- Atorvastatin 40-80 mg or rosuvastatin 20-40 mg daily
- LDL goal: <70 mg/dL
- If LDL remains >70 despite statin: add ezetimibe 10 mg daily; if still not at goal, add a PCSK9 inhibitor (alirocumab 300 mg or evolocumab 320 mg SC every 4 weeks)
E. ACE Inhibitor / ARB
- Start early in patients with LVEF <40%, HF, hypertension, or diabetes
- ARB if ACE inhibitor intolerant
F. Aldosterone Antagonist
- Add if patient is on both ACE inhibitor and beta-blocker AND has EF <40% with either symptomatic HF or DM
Step 4: Revascularization Strategy
ACS Management Flowchart
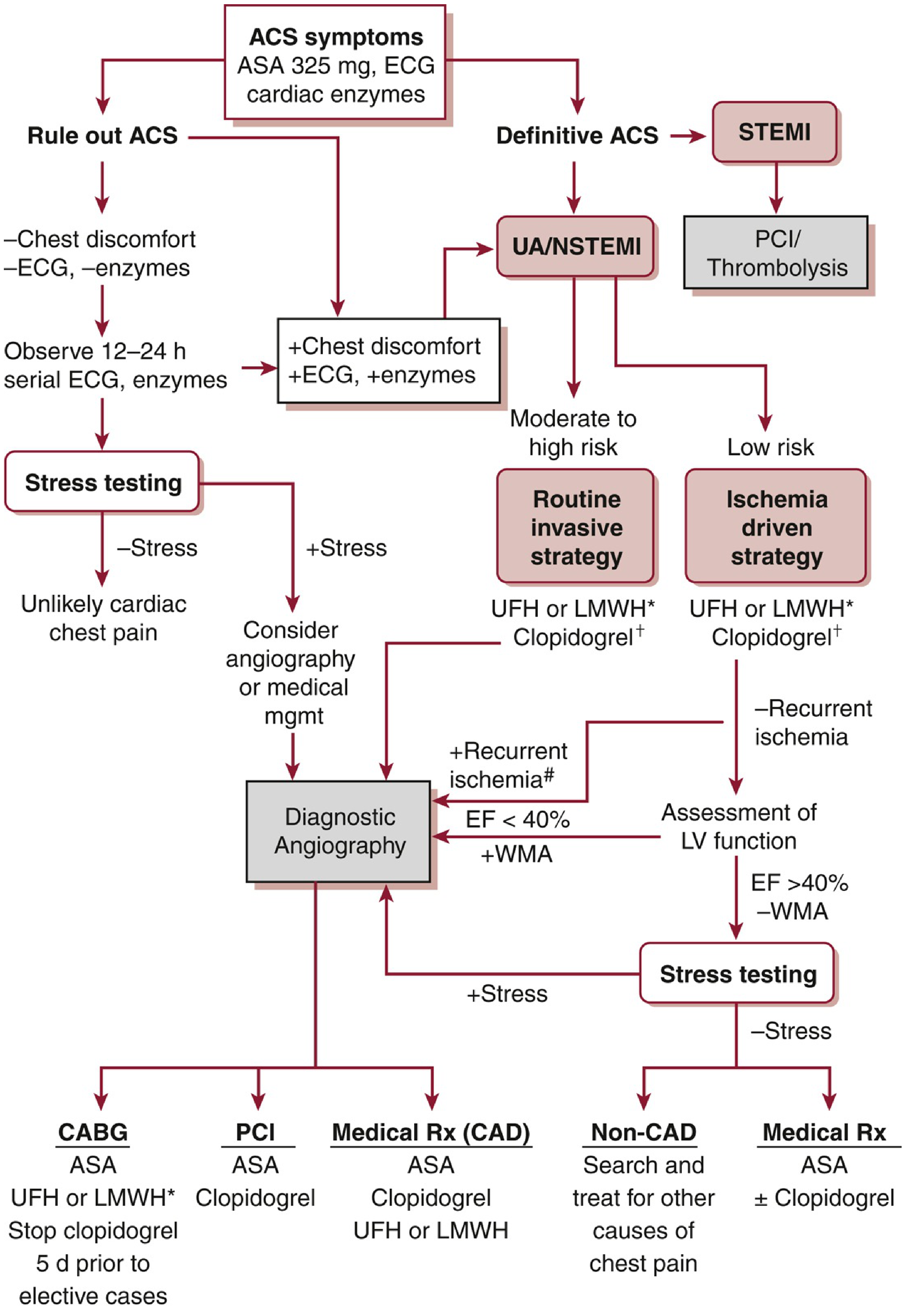
Figure: ACS management pathway - UA/NSTEMI patients stratified to routine invasive vs. ischemia-driven strategy based on risk. (Washington Manual of Medical Therapeutics)
Unlike stable angina, in ACS a routine invasive approach with PCI has been shown to reduce recurrent MI, hospitalizations, and death. All patients receive antithrombotic + antiplatelet + anti-ischemic therapy regardless of revascularization strategy.
Timing of Coronary Angiography
| Strategy | Timing | Indications |
|---|---|---|
| Immediate/Urgent invasive | <2 hours | Refractory angina, hemodynamic instability, shock, sustained VT/VF, new MR/HF |
| Early invasive | <24 hours | TIMI ≥3 or GRACE >140; rapid rise in biomarkers; new or presumed new ST depressions |
| Delayed invasive | 24-72 hours | Diabetes; renal insufficiency (GFR <60); LVEF <40%; early postinfarction angina; prior PCI <6 months; prior CABG; TIMI ≥2 or GRACE 109-140 |
| Ischemia-driven (conservative) | Elective if triggered | Low-risk (TIMI ≤1 or GRACE <109); biomarker-negative; patient preference; no high-risk features |
Washington Manual of Medical Therapeutics, p. 136-138
Ischemia-Driven (Conservative) Strategy
If no high-risk features develop, biomarkers remain negative, and symptoms respond to medical therapy:
- Patient should be angina-free for ≥12 hours before noninvasive stress testing
- If EF <40% or new wall motion abnormality → proceed directly to angiography
- If stress test positive or angina at low workload → angiography and revascularization
Refractory/Recurrent Angina Despite Medical Therapy
- Urgent cardiac catheterization and revascularization
- Intra-aortic balloon pump (IABP): bridge to revascularization in hemodynamically unstable patients; inflates in diastole (augments coronary perfusion) and deflates in systole (reduces afterload). Complication: lower limb ischemia ~3%
- Revascularization (PCI or CABG) relieves refractory angina in ~90% of patients
Goldman-Cecil Medicine, p. 648
Step 5: Post-Discharge / Long-Term Management
Following stabilization (identical to post-ACS care):
| Intervention | Details |
|---|---|
| DAPT | ASA + P2Y12 inhibitor for minimum 12 months post-ACS (or post-stenting); longer if tolerated |
| High-intensity statin | Indefinitely; target LDL <70 mg/dL |
| Beta-blocker | Especially post-MI; reduces sudden cardiac death |
| ACE inhibitor / ARB | Especially with EF <40%, DM, HF, HTN |
| Lifestyle modification | Smoking cessation, cardiac rehabilitation, diet, exercise |
| Glycemic control | HbA1c ≤7% in diabetics |
| Avoid NSAIDs | Except aspirin (increase CV risk) |
| Annual influenza vaccination | Recommended |
| Screen for depression | Common post-ACS; worsens outcomes |
Summary: UA/NSTEMI Acute Management at a Glance
1. ECG within 10 min + serial troponins
2. Aspirin 162-325 mg chewed immediately
3. Anticoagulate: enoxaparin 1 mg/kg SC q12h (or UFH/bivalirudin)
4. Add P2Y12 inhibitor (ticagrelor 180 mg or clopidogrel 600 mg)
5. Beta-blocker (oral within 24h)
6. Nitrates (sublingual / IV) for ongoing pain
7. High-intensity statin (atorvastatin 40-80 mg)
8. ACE inhibitor (if EF <40%, DM, HF, HTN)
9. Risk stratify → timing of angiography (urgent/early/delayed/conservative)
10. Long-term DAPT + statin + ACE-I + lifestyle modification
Key distinction from stable angina: In UA/NSTEMI, a routine invasive strategy is the default for moderate-to-high risk patients and improves outcomes. In stable angina, medical therapy is the initial default and revascularization is reserved for refractory or high-risk anatomic disease. Washington Manual of Medical Therapeutics, p. 138
Explain all cases for exam
Reading File
Running Command
I have all 37 cases. Here is a full structured explanation of every case:
State Interdisciplinary Exam - All 37 Clinical Cases Explained
CASE 1 - Contrast-Induced Nephropathy (AKI Stage 3)
Clinical picture: 58-year-old post-coronary stenting (5 days earlier). Develops anuria (<100 mL/2 days), leg edema, BP 160/110. Creatinine 589 µmol/L, urea 50 mmol/L, K+ 6.5, pH 7.19.
Diagnosis:
- Main: Contrast-induced nephropathy → AKI Stage 3 (anuria + creatinine 589)
- Background: CAD + stenting, CHF FC II, HTN Stage III Risk 4, T2DM, Obesity II
Life-threatening complications: Hyperkalemia (6.5 mmol/L), severe metabolic acidosis (pH 7.19), uremia
Emergency management:
- ICU admission
- Urgent decision on renal replacement therapy (indication: anuria, urea >30, K+ elevated, pH <7.25)
- Hyperkalemia correction: IV calcium gluconate 10% - 30 mL bolus; IV 40% glucose + insulin (2 units/5g glucose); furosemide 40-60 mg IV; sodium/calcium polystyrene sulfonate 15g x4/day orally or rectally
Prevention before contrast studies:
- Stop nephrotoxic drugs 3-4 days before
- Hydration: 0.9% NaCl 1-1.5 mL/kg/h for 6-12h before AND after procedure
- Use minimum contrast volume
- Monitor creatinine at 48 and 72h post-procedure
- Use rosuvastatin 40/20 mg or atorvastatin 80 mg in CKD patients
CASE 2 - Acute Gouty Arthritis + CKD
Clinical picture: 50-year-old male, uric acid 895 µmol/L (12 years), attacks of arthritis at multiple joints, tophi, HTN refractory to enalapril+amlodipine. Creatinine 200 µmol/L. Urinalysis: uric acid crystals, casts, low SG.
Diagnosis:
- Main: Acute gouty arthritis (1st MTP joint), tophi, chronic tubulo-interstitial nephritis, CKD C3b
- Comorbidity: HTN Stage II uncontrolled, Risk 4
Acute treatment:
- Nimesulide 200-400 mg/day; if ineffective → Colchicine 0.5 mg start, then 1 mg x3/day (adjust dose for GFR)
- Allopurinol is contraindicated in acute attack; target uric acid <360 µmol/L
- Anti-gout diet, alcohol prohibition
HTN management in gout+CKD:
- Losartan 100 mg/day (uricosuric effect) + amlodipine 10 mg/day
- Thiazide diuretics contraindicated (raise uric acid)
- CKD C3b management: low-protein diet, phosphorus-calcium correction, anemia prevention
Differential diagnosis: Rheumatoid arthritis, osteoarthritis, drug nephropathy
Classic gout features: Nocturnal joint attacks (1st MTP), tophi, "punch-out" lesions on X-ray, hyperuricemia, gouty nephropathy
CASE 3 - Chronic Glomerulonephritis, Nephrotic Syndrome
Clinical picture: 23-year-old male with chronic tonsillitis. Massive edema, oliguria, after sore throat. BP 140/95. Protein 5.4 g/L in urine, daily proteinuria 7.3 g/day, cholesterol 9 mmol/L, albumin 33%, total protein 45.6 g/L.
Main syndrome: Nephrotic syndrome - hypoalbuminemia + hypo-oncotic edema + hypercholesterolemia + proteinuria >3.5 g/day
Diagnosis: Chronic glomerulonephritis, nephrotic syndrome, exacerbation (after tonsillitis trigger)
Life-threatening complication: Interstitial pulmonary edema (basal rales bilaterally)
Emergency:
- ICU hospitalization
- IV furosemide 40 mg (control water balance)
- If diuresis <200 mL/12h, urea >30, hyperkalemia, pH <7.25 → renal replacement therapy (hemodialysis/ultrafiltration)
Treatment:
- Morphological variant guides therapy (nephrobiopsy needed)
- Immunosuppression: GCS alternating with alkylating cytostatics (cyclophosphamide, chlorambucil) as 1st line; alternative: calcineurin inhibitors
- Edema: Loop diuretics + IV albumin, water balance monitoring, salt restriction ≤5 g/day
- VTE prevention: Enoxaparin 1 mg/kg SC x2/day or UFH 5000 IU x4/day SC (monitor aPTT)
- RAAS blockade: ACE inhibitor or ARB (if no hyperkalemia, adequate GFR)
CASE 4 - Chronic Pyelonephritis Exacerbation + DM + HTN
Clinical picture: 50-year-old male, T2DM (metformin), HTN (valsartan). Fever 37.8°C, lumbar heaviness, urinalysis: leukocytes 20-30/hpf, specific gravity 1.012, traces of protein. Leukocytosis 11×10⁹, stabs 8%. Kidney ultrasound: deformed pelvis bilaterally.
Diagnosis: Chronic bilateral complicated pyelonephritis, exacerbation; CKD C? (calculate GFR)
Features in elderly pyelonephritis:
- Bilateral forms predominate (unilateral rare by 8th decade)
- Purulent forms more frequent (up to 25% men)
- Minimal typical symptoms (no fever, no lumbar pain)
- Atypical: confusion, falls, incontinence, normochromic anemia, HTN
- Common organisms: E. coli, Enterococcus; with obstruction: anaerobes
- Possible false-negative urine culture
Work-up: Urine per Nechiporenko, Zimnitsky test, GFR calculation, urine culture, prostate/bladder ultrasound, PSA, urology referral if obstruction
Treatment:
- Levofloxacin 500 mg x1/day for 10 days + adequate hydration
After normalization (10 days):
- Transition to herbal uroseptics for 6 months
- Avoid hypothermia
- If E. coli isolated: Urovaxom (OM-89) 1 capsule/day x 3 months (immunoprophylaxis)
CASE 5 - Rheumatoid Arthritis + Multiple Comorbidities
Clinical picture: 42-year-old female manager, 6 months of symmetric polyarthritis (PIP, MCP, wrist, knee joints), morning stiffness until midday, 4 kg weight loss, RF+ 120, ACCP+ 320, ESR 45, anemia (Hb 95), X-ray: periarticular osteoporosis, erosions. Also: heartburn/epigastric pain on NSAIDs, shortness of breath on exertion.
Diagnosis:
- Main: Rheumatoid arthritis, seropositive (RF+, ACCP+), advanced stage, Activity Grade 3, Radiological Stage II, FC II
- Comorbidities: NSAID-induced interstitial nephritis, Chronic erosive gastritis HP+, Anemia of chronic inflammation
Immediate symptomatic therapy (before workup results): Prednisolone 5-30 mg/day (until DMARD takes effect)
After workup (serum iron low, ferritin low, FGDS shows erosive gastritis HP+, hypostenuria on Zimnitsky):
- Iron supplements (IDA confirmed)
- 4-component HP eradication therapy
- Methotrexate 15 mg/week + folic acid (avoid MTX side effects) as DMARD
- Stop NSAIDs (interstitial nephritis)
- Dose adjust MTX after 3 months
Biologic DMARDs for RA:
- TNF-α inhibitors: infliximab, adalimumab, golimumab, certolizumab pegol, etanercept
- Other mechanisms: rituximab (anti-CD20), abatacept (CTLA4-Ig), tocilizumab (anti-IL-6)
CASE 6 - Systemic Lupus Erythematosus (SLE)
Clinical picture: 25-year-old, 1 year of disease. Started with fever, malar rash, macrohematuria → irregular prednisolone → arthritis, lymphadenopathy, pericarditis, bilateral exudative pleurisy. CBC: Hb 84, leukocytes 3.2×10⁹, platelets 140×10⁹. Urinalysis: proteinuria 2.2%, hematuria 40/hpf. Creatinine 144 µmol/L.
Diagnosis: SLE with nephritis, skin involvement, lymphadenopathy, pericarditis, pleuritis (polyserositis), arthritis, pancytopenia (three-lineage cytopenia), subacute course
Work-up: LE cells, ANA (antinuclear factor), anti-dsDNA, anti-Sm antibody, CIC, antiphospholipid panel (lupus anticoagulant, anti-cardiolipin antibodies), RF
Pathomechanism: SLE = hyperproduction of non-organ-specific autoantibodies (especially anti-dsDNA) → immune complex deposition → immunoinflammatory damage to organs → nephrotic syndrome + 3-lineage cytopenia
Differential diagnosis: Drug-induced lupus, granulomatous polyangiitis, HIV, primary CGN, RA
Treatment:
- Hydroxychloroquine + glucocorticoids
- High activity: pulse therapy methylprednisolone 500-1000 mg IV x3 days
- Lupus nephritis: cyclophosphamide (induction); azathioprine or mycophenolate mofetil (maintenance)
- Antihypertensives: ACE inhibitors, calcium antagonists
- Biologic: abatacept 125 mg SC weekly
- Plasmapheresis for refractory disease
CASE 7 - SLE with CNS Involvement (Neurovasculitis)
Clinical picture: 24-year-old female, 3 months: polyarthritis, malar + discoid rash, oral ulcers, peripheral + cavitary edema, stupor, neurological deficit (neurovasculitis). Pancytopenia, ESR 68, proteinuria 2.2 g/L, casts, hematuria, high-titer ANA, anti-dsDNA, anti-Sm antibodies. CRP 9.
Diagnosis: SLE, acute course, Activity Grade 3, with skin + joints + kidneys + CNS involvement + pancytopenia
Justification: Arthritis + malar rash + nephritis + cytopenia + lupus neurovasculitis + ANA + anti-native DNA + anti-Sm Ab + ESR 68
Differential: RA, primary glomerulonephritis, bone marrow disorders
Work-up: CXR, Echo, abdominal + renal US, kidney biopsy, daily proteinuria, brain MRI, LFTs, RFTs, electrolytes, lipid fractions, total protein + fractions, APS panel
Pulse therapy dose for neurovasculitis emergency: Methylprednisolone 1000 mg IV x 3 days
CASE 8 - Infective Endocarditis (IE)
Clinical picture: 53-year-old artist. Tooth extraction 2.5 months ago. Fever 39.5°C, sweating, chills, 10 kg weight loss, dyspnea, dizziness. Alcohol abuse + heavy smoker. Echo: vegetation 0.8×0.8 cm on aortic valve, aortic regurgitation Grade III, mitral regurgitation Grade II, LV dilation (EDD 6 cm, LA 5.5 cm). BP 130/40 (wide pulse pressure). Soft protodiastolic murmur at Botkin-Erb point and 2nd ICS right.
Syndromes:
- Inflammatory/septicemic (fever, chills, acute phase reactants)
- Intoxication (weakness, sweating, anorexia, weight loss, arthralgia, anemia)
- Valvular damage (aortic insufficiency)
- Thromboembolic disorders (Janeway lesions)
- Immune disorders (glomerulonephritis, hepatitis, splenomegaly, RF+)
- Heart failure
Diagnosis (DUKE criteria):
- Major: Echocardiographic evidence of intracardiac mass on valve
- Minor: Fever >38°C, predisposing heart condition, septic infarct pneumonia
- Sufficient: 1 major + 3 minor criteria
Complications: CHF Stage IIA, NYHA FC IV; glomerulonephritis; moderate anemia
Work-up: Blood cultures x3 (before antibiotics if possible) to identify organism and sensitivity
Treatment: Empirical antibiotics given severity; Grade III aortic regurgitation + large vegetation = indication for valve replacement → urgent cardiac surgery consultation
CASE 9 - Rheumatoid Arthritis + Secondary Amyloidosis
Clinical picture: 52-year-old female with 16-year RA history. Now: fever 38°C, wrist/MCP/PIP joint inflammation + stiffness. Proteinuria 6.6 g/L, daily proteinuria 9 g/day, hypoalbuminemia (albumin 30), total protein 50, creatinine 120 µmol/L (GFR ~45 ml/min = CKD C3a), cholesterol 7 mmol/L. RF+ 1:160.
Main syndromes: Articular, nephrotic, immunoinflammatory
Diagnosis:
- Main: RA, seropositive, late stage, erosive, Ro Stage II
- Complication: Secondary systemic AA amyloidosis (most likely cause of nephrotic syndrome in long-standing RA), CKD C3a A4
Differential for nephrotic in RA: Systemic vasculitis, amyloidosis, paraneoplastic nephrotic syndrome including myeloma
Work-up: ACCP, nephrobiopsy (verify amyloidosis + typing), abdominal + renal + cardiac US, ECG, coagulogram, LFTs, GFR calculation
Treatment:
- Urgent hospitalization (nephrotic syndrome + high RA activity)
- Correct DMARD therapy to reduce RA activity
- Edema: loop diuretics + IV albumin, fluid balance, salt ≤5 g/day
- VTE prevention: enoxaparin 1 mg/kg SC x2/day or UFH 5000 IU x4/day
- RAAS blockade: ACE inhibitor or ARB
CASE 10 - Isolated Systolic Hypertension in the Elderly
Clinical picture: 72-year-old retired woman, 20-year HTN history, irregular therapy. BP 162/62 → pulse pressure = 100 mmHg. BMI 30.5 (Obesity I), WC 102 cm. Insomnia, memory loss.
Diagnosis: HTN Stage II, Isolated Systolic AH (ISAH), Risk 3 (high). LVH. Obesity I.
Justification of ISAH: Pulse pressure ≥60 mmHg in elderly = sign of arterial wall stiffness. PP = 162 - 62 = 100 mmHg.
Preferred antihypertensive combination for elderly ISAH: Calcium channel blocker + thiazide diuretic (per current national recommendations). Alternative if CCB intolerant: ACE inhibitor or ARB.
After 3 months (BP 140-150/65, LDL 3.6, GFR 63, ALT 50):
- For age ≥70: target SBP 130-139 mmHg (subject to good tolerance), DBP 70-79 mmHg
- Intensify to triple fixed combination (ACE/ARB + diuretic + calcium antagonist) for better adherence
Hypertensive episode emergency (BP 180/100 + symptoms):
- Captopril 25 mg sublingual, BP check after 30-40 min
- If persistent: repeat captopril 25 mg sublingual, recheck 30-40 min
- If ineffective: call ambulance (EMS)
CASE 11 - Post-MI, Post-Stenting + Uncontrolled HTN + Dyslipidemia
Clinical picture: 75-year-old male, 3 months post-inferior STEMI (RCA stented with DES). Now: headache, dizziness, BP 190/100 on lisinopril 20 mg. LDL 3.6 mmol/L (target <1.4). Rosuvastatin 10 mg only.
Diagnosis: IHD. Post-infarction cardiosclerosis (inferior wall). RCA stenting (DES). HTN Stage III, uncontrolled, Risk 4 (very high). Dyslipidemia Type IIa (Fredrickson).
Drug groups for ongoing therapy:
- DAPT: ASA 75 mg + ticagrelor 90 mg twice daily until 1 year post-event (until June 18, 2024). Note: uncontrolled HTN increases bleeding risk → urgent BP correction
- Antihypertensives: Add calcium antagonist and/or diuretic to lisinopril
- Target BP for age + comorbidity: 130-139/70-79 mmHg
- Statin: Increase rosuvastatin dose (10 mg insufficient)
LDL target: <1.4 mmol/L (very high CV risk: established CAD)
- Current LDL 3.6 → increase statin + add ezetimibe 10 mg/day
CASE 12 - Stable Angina FC II + HTN + Dyslipidemia → STEMI
Clinical picture: 68-year-old driver, 2 months of exertional chest pain (>500m, relieved by rest). Misdiagnosed as intercostal neuralgia. HTN 5 years untreated. BMI 33.9, heredity positive (father+brother MI <55y). BP 170/100. LDL 3.57. ECG: LVH.
Diagnosis: IHD. Angina FC II. HTN Stage III, uncontrolled, Risk 4 (very high). LVH. Dyslipidemia Type IIb. Obesity I.
Work-up: OAM, CBC, biochemistry, GFR, lipid profile, ECG, Echo, carotid duplex (BCA), Holter ECG. Determine pretest probability → stress test or direct CAG if high probability.
Drug groups: Beta-blocker (1st line antianginal); short-acting nitrates PRN; antiplatelet (aspirin); high-intensity statin; RAAS blocker + diuretic or CCB (target BP <130/80)
CV risk and LDL target: Very high risk (established CAD) → LDL target <1.4 mmol/L
Emergency scenario (ST elevation V1-V4, nitrates x2 ineffective → STEMI):
- Prehospital: nitrates, morphine, oxygen, DAPT loading, anticoagulant SC
- Emergency transfer to PCI center; if delivery >120 min impossible → thrombolysis
- PCI + stenting of culprit artery
- Troponin to confirm MI
CASE 13 - Post-STEMI + Permanent Atrial Fibrillation + Dyslipidemia
Clinical picture: 75-year-old woman, 3 months post-inferior STEMI (RCA stented with DES). Permanent AF for 3 years (2 failed electrical cardioversions). HR 140, pulse 110, BP 110/80. Ankle swelling. LDL 3.2 (above target). CHA₂DS₂-VASc = 6, HAS-BLED = 2.
Diagnosis: IHD + PICS (inferior wall). RCA DES stenting. Permanent AF (EHRA 2b, CHA₂DS₂-VASc 6, HAS-BLED 2). CHF IIA.
Anticoagulation in AF (modern approach):
- CHA₂DS₂-VASc ≥2 in men / ≥3 in women → continuous anticoagulation indicated
- Preferred: Direct oral anticoagulants - apixaban, rivaroxaban, or dabigatran
- If no contraindications to NOACs, preferred over warfarin
Drug plan:
- Antiplatelet + NOAC: Clopidogrel 75 mg + NOAC (up to 12 months post-MI); then NOAC monotherapy
- Statins (indefinitely) - intensify to reach LDL <1.4
- Beta-blockers (rate control for AF + post-MI benefit, indefinitely)
- ACE inhibitor or ARB (indefinitely)
LDL target: <1.4 mmol/L (very high CV risk)
CASE 14 - Stable Angina FC II + HTN + Dyslipidemia
Clinical picture: 55-year-old mechanic, 2 years of exertional retrosternal pain (fast walk, stairs >2 flights), relieved by 1 sublingual NTG. HTN 5 years untreated. Heavy smoker (2 packs/day). BMI 33.9. LDL 4.2 (severely elevated). LVH on ECG.
Diagnosis: IHD. Angina FC II. HTN Stage III, uncontrolled, Risk 4 (very high). LVH. Dyslipidemia Type IIb. Obesity I.
Work-up: Per stable CAD guidelines - CBC, OAM, biochemistry, GFR, lipid profile, ECG, Echo, carotid duplex, Holter ECG. Stress test (if no contraindications) or CAG if high pretest probability.
Drug groups:
- Aspirin
- High-intensity statin (lipid-lowering)
- Beta-blocker and/or CCB and/or organic nitrates (antianginal)
- RAAS blocker (ACE/ARB) in combination for BP control
LDL target: <1.4 mmol/L (established CAD = very high risk)
CASE 15 - Permanent AF + Post-STEMI → GI Bleeding on Anticoagulant
Clinical picture: 75-year-old woman, 6 years post-inferior STEMI (RCA DES). Permanent AF 2 years. HR 140, pulse 110, BP 110/80. LDL 3.9. Irregular therapy.
Diagnosis: IHD + PICS (inferior wall). Permanent AF (tachysystolic, EHRA IIb, CHA₂DS₂-VASc 6, HAS-BLED 2). CHF IIA/FC II.
Work-up: CBC, OAM, biochemistry, GFR, lipid profile, TSH, ECG, Echo, Holter ECG
Anticoagulation: Preferred: NOAC - rivaroxaban 20 mg once daily; or warfarin (INR target 2.0-3.0)
Warfarin INR monitoring:
- At target INR: check at least monthly
- If out of range: check every 3 days; when INR 2-3, then weekly, then twice monthly, then monthly
GI bleeding emergency (black stool, weakness, abdominal pain on anticoagulant):
- Stop anticoagulant immediately
- Hospitalization in surgical department
- Assess degree of blood loss
- Urgent EGDS (EGD)
- Conservative hemostasis therapy
- Reassess risk/benefit of resuming anticoagulation; adjust regimen
CASE 16 - Bronchial Asthma (First Episode)
Clinical picture: 25-year-old driver, 3 months of episodes of suffocation with expiratory difficulty, hard sputum, attacks 2-3x/week especially at night, resolve spontaneously in ~1 hour. Scattered dry high-pitched rales. Mother has asthma.
Diagnosis: Bronchial asthma, allergic, first detected, exacerbation (not severe)
Work-up: CBC, OAM, biochemistry, total IgE, CXR, spirometry with salbutamol 400 mcg reversibility test (key diagnostic test), ECG, pulse oximetry
Acute treatment:
- Hospitalization, smoking cessation
- Inhaled bronchodilators (fenoterol/ipratropium bromide 1 mL) via nebulizer x3-4/day
- Inhaled GCS (beclomethasone or budesonide) 1000-2000 mcg/day
- After exacerbation control: asthma school education + basic therapy
Basic therapy in remission: According to Step 3 clinical guidelines for BA
CASE 17 - Community-Acquired Pneumonia → Deterioration
Clinical picture: 50-year-old non-smoker, 3-day history of fever 38°C, malaise, cough with light sputum. Breath weakened in lower right lung, crepitus, dullness. RR 20, HR 100.
Diagnosis: Community-acquired pneumonia, right-sided, non-severe
Work-up: CBC, CRP, CXR in 2 projections, SpO₂
Risk stratification (CRB-65): No confusion (0), RR <30 (0), BP >90/60 (0), age <65 (0) = Score 0 → outpatient treatment
Treatment: Amoxicillin 1000 mg x2/day orally + mucolytics (ambroxol or acetylcysteine) + oral rehydration + antipyretics for fever >38.5°C
After 3 days: condition worsened, green sputum, leukocytes 3.0×10⁹ (leukopenia!), lymphocytes 86%, ESR 30:
- This suggests viral etiology (lymphocytosis, leukopenia) or inadequate treatment
- Hospitalize in pulmonology/therapeutic department
- Change antibiotic to IV: amoxicillin/clavulanic acid 1.2 g x3/day or 3rd-gen cephalosporin (ceftriaxone 2-4 g/day) + macrolide (azithromycin 500 mg/day) or respiratory fluoroquinolone monotherapy (levofloxacin 1000 mg/day or moxifloxacin 400 mg/day)
CASE 18 - Community-Acquired Pneumonia
Clinical picture: 44-year-old smoker, preceded by URTI. Sudden fever 39°C, chills, dry then productive cough, right-sided chest pain. Bronchial breathing + crepitus in lower right lung, increased bronchophony, vocal fremitus. SpO₂ 99%, RR 22.
Diagnosis: Community-acquired pneumonia, right-sided, non-severe
Work-up: CBC, CRP, CXR in 2 projections
Outpatient treatment (age <60, no comorbidities, no respiratory failure, clear mind, stable hemodynamics)
Treatment: Amoxicillin or macrolide (clarithromycin/azithromycin) orally + ambroxol + oral rehydration + antipyretics >38.5°C
Severe pneumonia criteria:
- Major ("big") criteria: Severe respiratory failure (requiring ventilation), septic shock (requiring vasopressors)
- Minor ("small") criteria: RR >30/min; PaO₂/FiO₂ ≤250; multilobar infiltration; confusion; uremia (BUN ≥20 mg/dL); leukopenia <4×10⁹; thrombocytopenia <100×10¹²; hypothermia <36°C; hypotension requiring IV fluids
CASE 19 - CAP in Diabetic Patient + Antibiotic Assessment
Clinical picture: 51-year-old engineer with T2DM (diet-controlled). 2 days of weakness, mucopurulent sputum, fever 38.5°C. Smoking 30 pack-years. Decreased percussion + crepitus right lower lobe. CXR: S9 infiltration heterogeneous. Local doctor prescribed azithromycin 500 mg x1/day x3 days outpatient.
Q1. Was the diagnosis correct? Yes - CAP right-sided, non-severe ✓
Q2. Was outpatient treatment correct?
- CRB-65: confusion 0, RR <30 0, SBP >90 0, age <65 → Score 0 → outpatient acceptable
- However, with DM inpatient is preferable (comorbidity). Outpatient acceptable per score but borderline.
Q3. Was azithromycin correct? Yes - in mild CAP, azithromycin covers all major pathogens of CAP (Streptococcus pneumoniae, atypicals)
Q4. Criteria for antibiotic effectiveness:
- Temperature persistently <37.2°C for ≥48 hours
- No intoxication syndrome
- RR <20/min (without chronic DN)
- No purulent sputum (except chronic producers)
- CBC: leukocytes <10×10⁹, neutrophils <80%, juvenile forms <6%
Severe pneumonia criteria: (same as Case 18 above)
CASE 20 - COPD Gold 4 + Cor Pulmonale Decompensated
Clinical picture: 57-year-old heavy smoker (37 pack-years). FEV1 = 30% predicted, FEV1/FVC = 0.6. SpO₂ 87%. CAT score 28. Exacerbations 2-3x/year, 1 hospitalization last year. Right heart hypertrophy on ECG. Cyanosis, leg edema, liver 2 cm below costal margin, distended neck veins. Polycythemia (Hb 168).
Diagnosis: COPD, GOLD Stage 4 (extremely severe), Group D, exacerbation. Chronic cor pulmonale (decompensated). Respiratory failure Grade 2.
Treatment:
- Hospitalize, smoking cessation
- Low-flow oxygen 2-4 L/min (maintain SpO₂ >94%)
- Nebulizer bronchodilators (fenoterol/ipratropium, salbutamol) x2-3/day
- Inhaled GCS (beclomethasone/budesonide) 1000 mcg/day
- Theophylline 100-300 mg/day
- Mucolytics (ambroxol, ACC)
- Diuretics: loop (torasemide) + potassium-sparing (spironolactone) for edema
- Heparin (thrombosis prevention in cor pulmonale)
Indications for long-term low-flow O₂ therapy (LTOT):
- Absolute: pO₂ ≤55 mmHg or SpO₂ ≤88%
- Relative (special conditions): pO₂ 55-59 mmHg or SpO₂ 89% WITH: cor pulmonale, edema, polycythemia (Ht >55%)
- No indication: pO₂ ≥60 mmHg, SpO₂ ≥90% (without special conditions)
Respiratory failure definition & grades:
- DN = PaO₂ <60 mmHg and/or PaCO₂ >45 mmHg
- Grade 1: PaO₂ 60-79 / SpO₂ 90-94%
- Grade 2: PaO₂ 40-59 / SpO₂ 75-89%
- Grade 3: PaO₂ <40 / SpO₂ <75%
CASE 21 - COPD (Emphysematous Type)
Clinical picture: 52-year-old typesetter, 30 cigarettes/day since age 20. Progressive dyspnea + weight loss for 2 years. Barrel-shaped chest, box percussion sound, diffusely weakened vesicular breathing. SpO₂ 96%. Liver +4 cm (cor pulmonale). Accent II tone over PA.
Diagnosis: COPD (emphysematous/"pink puffer" type)
Justification: Smoking history (HCI >10 pack-years), broncho-obstructive syndrome, gradual progressive course, emphysema signs on exam
Work-up: CBC, OAM, biochemistry (creatinine, glucose, bilirubin, ALT, AST, CRP), spirometry + salbutamol reversibility test, CXR, ECG
Treatment:
- Smoking cessation
- Basic therapy: Long-acting M-anticholinergic (tiotropium bromide, aclidinium bromide, glycopyrronium) - preferred in GOLD C/D emphysema
- Short-acting inhaled bronchodilator PRN (fenoterol/ipratropium, salbutamol)
LTOT indications: Same as Case 20
CASE 22 - Duodenal Ulcer + HP + GI Bleed Complication
Clinical picture: 45-year-old engineer, 3-year history of epigastric pain (hunger pain, nocturnal pain), constant heartburn, heaviness after eating, nausea. Smokes, coffee abuse, irregular meals. EFGDS: ulcer defect 0.5 cm on posterior wall of duodenal bulb, white fibrin base, urease test positive.
Diagnosis: Peptic ulcer of duodenal bulb, HP-associated, subacute phase, with pain and dyspeptic syndromes, moderate severity
Work-up: X-ray (niche sign, convergence of folds), endoscopy (visual + targeted biopsy), intragastric pH-metry, electrogastrography, HP detection (breath test, PCR of feces, morphological biopsy)
Treatment (4-component eradication):
- PPI (omeprazole 20 mg x2/day) + clarithromycin 500 mg x2/day + amoxicillin 1000 mg x2/day x14 days
- Gastroprotector: De-Nol (bismuth subcitrate)
- Antacids (Maalox/Almagel) or alginates (Gaviscon)
GI bleeding complication (coffee-ground vomiting, weakness, dizziness):
- Lay patient flat, lower head if hemodynamically unstable
- Cold compress to epigastric region, NPO (nothing by mouth or water)
- Etamsylate 12.5% 2-4 mL IV
- Urgent hospitalization to surgical department
CASE 23 - Cholelithiasis + Chronic Calculous Cholecystitis → Biliary Colic
Clinical picture: 48-year-old obese woman, mother had cholecystectomy. 10-15 years of biliary pain after fatty food, stops with drotaverine. Now 2 weeks of constant pain + nausea + chills. Murphy+, Lepene+, Ortner+. US: gallbladder enlarged, walls 4 mm, multiple calculi up to 2.5 cm. CBD 6 mm.
Diagnosis: GSD. Chronic calculous cholecystitis, without exacerbation. Hypomotor GB dysfunction. Chronic reflux gastritis (type C), exacerbation. Chronic duodenitis. Duodeno-gastric reflux.
Additional work-up:
- Fecal elastase-1 (exocrine pancreatic function)
- Pancreatic amylase + lipase (exclude pancreatitis)
- MR-pancreatocholangiography or endo-US (CBD stones, pancreatobiliary zone)
- Duodenal sounding (biliary dyskinesia type + bile culture)
Treatment:
- Planned laparoscopic cholecystectomy
- UDCA (Ursofalk, Ursosan) courses under US control
- Antispasmodics (Odeston, Buscopan)
- Prokinetics (metoclopramide, domperidone)
- Diet: no fatty, fried, smoked, flour
Biliary colic emergency (acute pain, nausea, vomiting):
- Myotropic antispasmodics IV/IM (drotaverine) or selective antispasmodics (Odeston, Buscopan)
- If persistent: hospitalize in surgical department
CASE 24 - Chronic Alcoholic Pancreatitis Exacerbation
Clinical picture: 46-year-old driver, alcohol abuse 7 years. After celebration: constant epigastric pain radiating to back/left abdomen, nausea, vomiting, bloating, steatorrhea x3/day (greasy, fetid). US: heterogeneous pancreas, calcifications, dilated duct, head 5 cm. Liver enlarged (alcoholic steatosis). Gallstone 8 mm.
Diagnosis: Chronic alcoholic pancreatitis, pain form, with exocrine insufficiency, exacerbation. Alcoholic hepatic steatosis. GSD, chronic calculous cholecystitis, latent.
Work-up: Biochemistry (glucose, lipase, amylase, LFTs, bilirubin, alkaline phosphatase), urinary diastase, fecal elastase-1, glycemic profile + HbA1c (exclude DM), abdominal CT (exclude cysts/tumors), EGDS (exclude duodenal ulcer), surgical consultation
Treatment:
- Hospitalize, absolute alcohol abstinence, diet #5
- Antispasmodic: drotaverine 80 mg IM x2/day
- Analgesics: baralgin, paracetamol
- Enzyme replacement therapy (Creon) for exocrine insufficiency
- Glycemia correction if needed
Refractory pain management:
- If NSAIDs insufficient: narcotic analgesics (promedol, morphine) or tramadol
- Antioxidant therapy
- Tricyclic antidepressants (amitriptyline) as pain modulators
CASE 25 - Chronic Biliary-Dependent Pancreatitis + Pancreatogenic Diabetes
Clinical picture: 47-year-old, post-cholecystectomy (age 40). 6 months post-op: persistent upper abdominal pain, radiating to back, worse with diet errors. Last 1.5-2 years: chronic loose stool, 8 kg weight loss, perineal itching, polydipsia, polyuria. Positive Kerte's sign, Mayo-Robson's sign (head of pancreas involvement).
Diagnosis: Chronic biliary-dependent pancreatitis, pain form, with exocrine AND endocrine insufficiency, exacerbation. Pancreatogenic diabetes mellitus (mild course)
Work-up: CBC, OAM, urine amylase, biochemistry including lipase, amylase, glucose, C-peptide, coprogram, fecal elastase-1, abdominal US, endoscopic US, MR-cholangiopancreatography, CT abdomen
Treatment:
- Diet #5p (fasting x3 days initially)
- PPIs (suppress gastric secretion)
- Enzyme preparations (Creon, Micrasim)
- M-anticholinergics (platyphylline)
- Myotropic antispasmodics (mebeverin, drotaverine)
- Insulin therapy in low doses (pancreatogenic DM)
Differential diagnosis: Gastric ulcer, GSD/chronic cholecystitis, inflammatory bowel disease, abdominal ischemic syndrome, pancreatic cancer, duodenitis with SIBO
Pathogenesis: Biliary tract disease → ↑pressure in CBD → biliary-pancreatic reflux of infected bile → partial activation of pancreatic enzymes in ducts → edema-hemorrhage-destruction → fibrosis → exo- and endocrine insufficiency
CASE 26 - Chronic Atrophic Gastritis Associated with H. pylori
Clinical picture: 45-year-old woman, 20-year chronic gastritis, exacerbations 1-2x/year, never had eradication therapy. Current exacerbation after diet error. EFGDS: atrophic mucosa in antrum, rapid urease test positive. Biopsy: atrophy + chronic polymorphocellular infiltration.
Diagnosis: Chronic atrophic gastritis, HP-associated, exacerbation
Additional work-up: CBC, abdominal US, GI fluoroscopy, coprogram, stool for dysbiosis
Treatment:
- Nolpaza (pantoprazole) 40 mg morning x3 weeks
- De-Nol 120 mg x4/day x3 weeks
- Ganaton (itopride) 50 mg x3/day x3 weeks (prokinetic)
- If patient consents: eradication - clarithromycin 500 mg x2/day + amoxicillin 1000 mg x2/day x14 days + PPI
Role of H. pylori: Central etiopathogenetic factor in: chronic gastritis type B, duodenitis/gastroduodenitis, peptic ulcer (gastric and duodenal), MALT lymphoma, non-cardiac gastric cancer. HP pathogenicity factors: colonization (motility, adhesins, urease), persistence (enzymes, LPS, coccal forms), disease-causing (vacuolating cytotoxin VacA, CagA antigen, pro-inflammatory factors)
CASE 27 - GERD with Erosive Esophagitis
Clinical picture: 45-year-old woman, 3 months of heartburn + acid regurgitation, worse lying down + bending after meals. Smoker (10 cigarettes/day). BMI 31. EGDS: multiple areas of mucosal hyperemia + non-confluent erosions of distal esophagus <5 mm.
Diagnosis: GERD, endoscopically positive form, Stage II (Grade A), with typical symptoms
Work-up: 24h esophageal pH-metry; EGDS + biopsy; barium fluoroscopy; PPI diagnostic test. Additional: manometry (LES tone), esophageal impedancemetry, scintigraphy, genetic screening for Barrett's esophagus
Treatment (combination):
- PPIs (rabeprazole, dexlansoprazole)
- Antacids
- Prokinetics (itopride)
Lifestyle recommendations:
- Fractional meals in small volumes, 2-3h intervals; no food 2-3h before bed
- Exclude: canned food, smoked meats, fatty/fried food; reduce coffee
- Weight loss
- Avoid: excessive physical exertion, bending forward, lying down <30-60 min after eating
- Sleep with elevated head of bed
- Smoking cessation
Pathogenesis: ↓LES pressure → ↓esophageal peristalsis → delayed gastric emptying → duodenogastric + gastroesophageal reflux → mucosal exposure to acid/pepsin → esophagitis
CASE 28 - Chronic Alcoholic Hepatitis + Intrahepatic Cholestasis
Clinical picture: 48-year-old, 13 years heavy alcohol use (>60 g ethanol/day). Jaundice, telangiectasias (chest/back/shoulders), palmar erythema, right hypochondrium pain. ALT 203, AST 214, GGTP 89, ALP 298, total bilirubin 25. Indirect bilirubin elevated (22.5). Hepatitis B and C markers negative. Elastometry: F2 fibrosis (METAVIR). No varices findings.
Diagnosis: Chronic alcoholic hepatitis, moderate activity, moderate fibrosis (F2). Intrahepatic cholestasis.
Work-up: EGDS (assess esophageal varices, assess mucosa), abdominal US (other organs, gallbladder, pancreas), MR liver + MR-cholangiopancreatography
Treatment:
- Alcohol abstinence (primary etiological treatment) + narcologist consultation
- Antispasmodic for pain: mebeverine 200 mg x2/day
- Hepatoprotector: S-adenosylmethionine (Heptral) 400-1600 mg/day x1 month
- UDCA 8-10 mg/kg/day x3 months (cholestasis + hepatoprotection)
After 1 month (improvement, normalized LFTs):
- Abdominal US every 6 months
- Hepatoprotector courses x2/year
- Long-term UDCA 2 tablets (600 mg)/day
Pathogenesis: Ethanol → acetaldehyde accumulation → ↓β-oxidation of fatty acids → lipid peroxidation → disruption of phospholipid cell membranes → alcoholic hyaline → disruption of intracellular transport → balloon dystrophy → hepatocyte necrosis → fibrosis. Cytolysis: ↑ALT, ↑AST.
CASE 29 - GERD + Erosive Gastritis + Possible HP + GI Bleed
Clinical picture: 48-year-old welder, shift worker, smoker (20 cigarettes/day since age 13). 2 years of severe heartburn, acid regurgitation especially lying down/bending. Episode of black liquid stool 3 days ago (resolved). EGDS: multiple small erosions lower third esophagus (up to 50% circumference), cardia incompetent, gastric mucosal prolapse into esophagus, multiple flat erosions in antrum. Occult blood positive.
Diagnosis: GERD. Chronic erosive reflux esophagitis Stage II, exacerbation. Chronic erosive antral gastritis, HP-associated(?), exacerbation, complicated by mild bleeding.
Work-up: 24h intraluminal esophageal pH-metry, esophageal manometry, barium fluoroscopy (with lateroposition), mucosal biopsy (esophagus + stomach), HP blood test
Treatment plan:
- Non-drug: fractional meals, no lying 3h post-meal, elevated headboard, no tight clothes, smoking cessation, avoid heavy loads
- Rabeprazole 20 mg x1/day before meals x8 weeks, then maintenance 20 mg/day x52 weeks
- Itopride (Ganaton) 1 tab x3/day before meals x4 weeks
- Maalox 1 tab x3/day 40-60 min after meals
- UDCA 250 mg x2/day x4 weeks (for bile reflux)
Eradication if HP confirmed:
- Rabeprazole 20 mg x2/day + amoxicillin 1000 mg x2/day + clarithromycin 500 mg x2/day x10-14 days
- Add bismuth subcitrate 2 tabs x2/day or rebamipide for mucosal protection
Control endoscopy: annually; gastroenterologist review every 6 months; disability certificate 21-28 days (complicated form up to 2.5 months)
Pathogenesis: ↓LES function + ↓esophageal clearance + damaging refluxant (acid/bile/pepsin) + esophageal hypersensitivity → esophagitis/erosions/Barrett's/strictures
CASE 30 - Peptic Ulcer + Accomplished GI Bleeding + IHD (Complex Comorbidity)
Clinical picture: 69-year-old with post-MI (1.5 years ago), post-stenting (10 months), on aspirin + clopidogrel (stopped rosuvastatin 5 months ago). 4-5 weeks epigastric pain, black stools for 2 days a week ago (resolved). Anemia: Hb 103, MCV 22 (microcytic, hypochromic). Cholesterol 7.8, TG 2.6. ECG: old anterior MI (Q waves V1-V4, negative T).
Diagnosis: Peptic ulcer of stomach/duodenum, exacerbation. Accomplished GI bleeding. Posthemorrhagic anemia (mild). Possible NAFLD, chronic pancreatitis. IHD, PICS, post-stenting, angina FC II, CHF IIA. Dyslipidemia.
Work-up: OAM, biochemistry (LFTs, bilirubin, alkaline phosphatase, GGTP, amylase, total protein, glucose), abdominal US, EGDS, colonoscopy, anti-HP antibodies, cardiologist consultation
Management:
- Diet 4-5x/day, avoid spicy/salty/fried/smoked
- De-Nol, Duspatalin, fibrate (Trakor for high TG), iron preparations
- PPI, HP eradication if confirmed
PPI choice for this patient:
- Pantoprazole or rabeprazole - these are NOT metabolized via CYP450 system → less liver burden + less interaction with clopidogrel (unlike omeprazole/esomeprazole which reduce clopidogrel efficacy)
- PPI standard dose x2/day + bismuth subcitrate 120 mg x4/day + clarithromycin 500 mg x2/day + amoxicillin 1000 mg x2/day (or metronidazole 500 mg x2/day)
Pathogenesis of PUD: Imbalance between aggressive factors (HCl, pepsin, HP, bile, NSAIDs, smoking) and mucosal protective factors (mucus, bicarbonate, prostaglandins, blood flow, cell regeneration). HP + blood group 0 are key risk factors for duodenal ulcer.
CASE 31 - Ulcerative Colitis, Left-Sided, Moderate Attack
Clinical picture: 29-year-old programmer, 5 months of progressive diarrhea 5-6x/day (including at night) with blood and mucus, tenesmus, left flank pain, 5 kg weight loss. Worsened after self-treatment with chloramphenicol. Sigmoidoscopy: diffuse hyperemia, edema, contact bleeding, confluent erosions, fibrin, blood-mucus. Fecal calprotectin 532 µg/g. CRP 95 mg/L.
Diagnosis: Ulcerative colitis, acute course, left-sided lesion, moderate severity attack
Work-up: Bacterial stool culture, abdominal X-ray, colonoscopy with biopsy (full extent assessment), irrigoscopy, abdominal US, CT with bowel contrast
Treatment:
- Non-drug: Diet #4, psychological support
- 5-ASA (mesalazine): 3-4.8 g/day orally + 2-4 g/day as enemas x6-8 weeks
- Remission maintenance: mesalazine 1.2-2.4 g/day orally + 2 g x2/week enemas
- If 5-ASA insufficient: GCS budesonide 9 mg/day x8 weeks
Disability assessment: Moderate disease in exacerbation phase = temporary disability 1.5-2 months
Pathogenesis: Immune dysregulation (genetic factors, food allergy, stress, dysbiosis) → activation of pro-inflammatory cytokines → lymphoplasmacytic infiltration of colonic mucosa
CASE 32 - B12 Deficiency Anemia, Severe (Funicular Myelosis + CHF)
Clinical picture: 65-year-old woman, 6 months progressive weakness, difficulty swallowing, dyspnea, leg swelling. Bright red smooth cracked tongue (Hunter's glossitis). Pancytopenia: Hb 40, erythrocytes 1.0×10¹², MCV 110, MCH 40, reticulocytes 0.1%. Macro- and anisocytosis, megalocytes, Jolly bodies, Cabot rings. Neurological: distal hyperesthesia, ↑deep tendon reflexes, ↓muscle strength (funicular myelosis).
Diagnosis:
- Main: Chronic DNA/RNA-dependent hyperchromic macrocytic anemia, severe
- Complications: Leukopenia; funicular myelosis (subacute combined degeneration of spinal cord); myocardial dystrophy, LVH, CHF Stage IIB, FC III-IV
Work-up: Biochemistry (bilirubin fractions - to type jaundice); Echo (CHF verification); EGDS + colonoscopy (exclude GI pathology); stool for helminth ova (exclude Diphyllobothrium latum); serum B12 + folic acid + methylmalonic acid levels; antibodies to parietal cells + Castle's intrinsic factor; bone marrow aspirate (exclude leukemia)
Differential:
- Folic deficiency anemia - no funicular myelosis
- IDA - microcytic, ↓serum iron
- Hemolytic anemia - reticulocytosis, not macrocytic
- Acute leukemia - no thrombocytopenia here, no blast cells
Treatment:
- Cyanocobalamin 500 mcg IM daily x1 week (neurological symptoms = higher dose); then 500 mcg every 5-7 days until Hb/WBC normalize; then 500 mcg weekly x2 months (depot formation)
- Given severity of anemia + myocardial dystrophy: erythrocyte suspension transfusion indicated
- Efficacy: reticulocyte rise at days 5-7; Hb rise after 1-1.5 weeks; LDH/bilirubin normalization
CASE 33 - Iron Deficiency Anemia, Severe (Sideropenic Syndrome)
Clinical picture: 21-year-old disabled female (cerebral palsy), never ate meat, frequently ate soil (pica/geophagia). Fatigue, hair loss, cheilitis, taste perversion. Hb 60 g/L, color index 0.63, MCV ↓ (microcytic, hypochromic). Serum iron 4.1 µmol/L (low), TIBC 103 µmol/L (↑ = unsaturated), occult blood negative x3.
Diagnosis: Chronic iron deficiency anemia, severe (Hb 60 g/L)
Justification:
- Anemic syndrome: fatigue, anorexia, functional cardiac murmur
- Sideropenic syndrome: hair loss, cheilitis, taste perversion (geophagia), ↓serum iron, ↑TIBC, low color index
Work-up: LFTs (hepatomegaly); stool for helminth ova (eats soil → Ascaris, Toxocara); stool occult blood; EGDS + sigmoidoscopy/colonoscopy; ferritin (exclude relative iron deficiency); abdominal + pelvic US; gynecology consultation
Differential: B12-deficiency anemia (exclude - hypochromic, ↓iron, ↑TIBC = opposite of B12); anemia of chronic disease (no sideropenic syndrome); thalassemia (↑reticulocytes, target cells, normal/elevated iron, splenomegaly, bilirubin)
Treatment:
- Oral iron preparations (ferrous or ferric), 100-120 mg elemental iron/day in 1-2 doses (polymaltose complex preferred - good absorption, fewer side effects)
- Continue until Hb normalizes, then maintenance 50-60 mg/day x3-4 months to replenish depot
- Efficacy: clinical improvement days 5-6; reticulocytes rise days 8-12; Hb rises after 2.5-3 weeks
- Consider IV iron (iron carboxymaltose, iron hydroxide sucrose) given cognitive deficit and need for compliance
- Transfusion NOT indicated (no cardiovascular compromise, no circulatory-hypoxic syndrome meeting transfusion threshold)
CASE 34 - Acute Leukemia (First Attack)
Clinical picture: 35-year-old male, 1 month of severe weakness, dyspnea, bruising all over, nosebleeds, gingival bleeding, fever 38.1°C. CBC: Hb 76, leukocytes 35×10⁹, blasts 21%, platelets 21×10⁹. No lymphocytes/monocytes/stabs. Hepatomegaly to navel level. Splenomegaly. Elevated bilirubin 48.8, prolonged aPTT 50s.
Clinical syndromes:
- Hemorrhagic (bruising, nose/gum bleeding, thrombocytopenia)
- Circulatory-hypoxic (weakness, dyspnea, anemia)
- Hyperplastic (hepatosplenomegaly, leukemic infiltration)
- Intoxication (fever, weakness)
Diagnosis: Acute leukemia (unspecified), 1st attack, extended phase. Metaplastic anemia (moderate). Metaplastic thrombocytopenia with hemorrhagic syndrome. Leukemic liver infiltration.
Work-up:
- Sternal puncture (cytological bone marrow exam - confirm blast cell dominance)
- Cytochemical reactions on blast cells (lineage determination)
- Immunophenotyping - most informative (distinguish AML vs ALL)
- Cytogenetic/molecular biology (prognosis, targeted therapy eligibility)
- Biochemistry: bilirubin fractions, GFR, LDH, AST, ALT, urea, uric acid
- Viral hepatitis markers
- Abdominal US, ECG, Echo, CXR
Treatment:
- Admit to hematology department
- Specific chemotherapy depends on AML vs ALL variant
- Blood component therapy:
- Anemia correction: erythrocyte suspension transfusion
- Hemorrhagic syndrome: FFP (fresh frozen plasma) + platelet concentrate transfusion
- Hepatoprotectors (UDCA) for hyperbilirubinemia/liver involvement
- Infusion therapy + forced diuresis + xanthine oxidase inhibitors (allopurinol) for tumor lysis nephropathy prevention
CASE 35 - IDA in Young Woman + Menorrhagia (Mild, then Follow-up)
Clinical picture: 28-year-old woman, anemia since age 16, irregular iron therapy. Profuse menstruation x5-7 days every 21 days. 2 pregnancies. Weakness, palpitations (HR 110), dizziness, taste perversion (dry pasta, buckwheat), sore throat. Hb 94 g/L, MCH 25 pg, MCV 76 fl (microcytic), serum iron 7.6, ferritin 8.8 µg/L.
Diagnosis: Chronic IDA, mild degree (Hb >90 g/L). Circulatory-hypoxic + sideropenic syndromes confirmed by lab.
Work-up: Gynecologist consultation; stool for occult blood; abdominal + pelvic US; EGDS; sigmoidoscopy (exclude GI blood loss source)
Drug choice: Oral iron (polymaltose iron complex) 200 mg/day until Hb normalizes
After 2 months (Hb normalized to 122, but ferritin still low at 12 µg/L):
- Continue therapy at reduced dose 100 mg/day for 4-6 months to replenish iron depot
- Monitor ferritin every 6 months while menorrhagia persists
CASE 36 - B12 Deficiency Anemia, Severe (Elderly + Anginal Symptoms)
Clinical picture: 67-year-old woman, 6 months progressive weakness, "shaky gait," tingling in limbs (funicular myelosis). New: pressing retrosternal pain + dyspnea on exertion (last 2 months). Jaundiced + pale skin. Splenomegaly. Hb 68 g/L, MCV 104.6, MCH 40.6, reticulocytes 0.8%, thrombocytopenia (70×10⁹), leukopenia (2.3×10⁹). Macrocytosis, hypersegmented neutrophils, Jolly bodies, Cabot rings. Indirect bilirubin 38.4 µmol/L (hemolytic component). Bone marrow: megaloblastic hematopoiesis.
Diagnosis: Chronic hyperchromic macrocytic anemia, severe (Hb <70 g/L). Circulatory-hypoxic syndrome, neurological deficit (unsteadiness, hyperesthesia, tingling) = funicular myelosis.
Work-up: Serum B12 + folic acid; antibodies to helminths; stool for helminths; abdominal US; EGDS + colonoscopy
Expected EGDS finding: Atrophy of gastric mucosa (autoimmune atrophic gastritis → ↓intrinsic factor → ↓B12 absorption)
Transfusion indications:
- Age + increasing anginal symptoms on exertion + Hb <70 → erythrocyte suspension transfusion indicated
Treatment:
- If B12 deficiency: cyanocobalamin 500 mcg/day IM x1 month, then 500 mcg IM x1/week x2 months
- If folic acid deficiency: folic acid 1-2 mg/day x1 month
CASE 37 - B12 Deficiency Anemia, Severe + Cognitive Decline + Atrophic Gastritis
Clinical picture: 63-year-old woman, HTN on lisinopril+amlodipine. 6 months of severe weakness + cognitive impairment (forgetfulness, word-finding difficulty). Crimson tongue (Hunter's glossitis). Pale + mucous membranes. Epigastric sensitivity. Liver +2 cm. CBC: Hb 52 g/L, MCV 108, MCH 36.1, thrombocytopenia (PLT 76×10⁹), leukopenia (WBC 2.8×10⁹). Macrocytosis.
Diagnosis: DNA/RNA-dependent anemia (B12 deficiency, folic acid deficiency), severe (Hb <60 g/L = emergency hospitalization)
Management:
- Emergency hospitalization in therapeutic hospital (Hb <60 g/L + moderate thrombocytopenia = urgent)
- EGDS → atrophic gastritis found (confirms mechanism of B12 deficiency)
- Cyanocobalamin 500 mcg/day IM started
After 1 month (Hb improved to 96, but cognitive symptoms remain):
- Atrophic gastritis confirmed → continue cyanocobalamin 500 mcg IM every 2 weeks
- Add folic acid (atrophic gastritis impairs folate absorption also)
- Cognitive symptoms may be slow to resolve (neurological damage is slower to reverse than hematological)
Q4 - Can diet increase Hb?
- No - because atrophic gastritis impairs intrinsic factor production → B12 cannot be absorbed from food or oral multivitamins regardless of diet quality. Only parenteral B12 is effective. Dietary advice alone is ineffective in pernicious anemia.
Quick Reference Summary Table
| Case | Diagnosis | Key Drug(s) |
|---|---|---|
| 1 | Contrast-induced nephropathy, AKI Stage 3 | Calcium gluconate IV, glucose+insulin, furosemide |
| 2 | Acute gouty arthritis + CKD | Nimesulide/colchicine; losartan (not thiazides!) |
| 3 | CGN nephrotic syndrome | GCS + cyclophosphamide; furosemide + albumin; enoxaparin |
| 4 | Chronic pyelonephritis exacerbation | Levofloxacin 500 mg x10 days; urovaxom maintenance |
| 5 | Rheumatoid arthritis | Prednisolone bridge → methotrexate 15 mg/week + folic acid |
| 6 | SLE + nephritis + polyserositis | Hydroxychloroquine + GCS; pulse methylprednisolone; cyclophosphamide |
| 7 | SLE + neurovasculitis | Methylprednisolone 1000 mg IV x3 days |
| 8 | Infective endocarditis (aortic valve) | Empiric antibiotics; valve replacement surgery |
| 9 | RA + secondary AA amyloidosis | DMARD correction; diuretics + albumin; enoxaparin; RAAS blockade |
| 10 | ISAH elderly | CCB + thiazide diuretic; captopril SL for crisis |
| 11 | Post-STEMI + HTN uncontrolled | DAPT (ASA + ticagrelor 90 mg x2); add CCB/diuretic; statin ↑ + ezetimibe |
| 12 | Stable angina II + HTN | Beta-blocker; aspirin; statin; RAAS+diuretic/CCB; STEMI→PCI |
| 13 | Post-MI + permanent AF | Clopidogrel + NOAC (12 months) → NOAC monotherapy; statins; beta-blocker |
| 14 | Stable angina II + HTN + dyslipidemia | Aspirin; statin; beta-blocker ± CCB ± nitrates; RAAS + diuretic |
| 15 | Permanent AF + post-MI → GI bleed | Rivaroxaban or warfarin (INR 2-3); surgical admission for GI bleed |
| 16 | Bronchial asthma (first episode) | Fenoterol/ipratropium nebulizer + inhaled GCS; step 3 basic therapy |
| 17 | CAP right non-severe → deterioration | Amoxicillin → if deterioration: IV amoxiclav or cephalosporin + macrolide |
| 18 | CAP right non-severe | Amoxicillin or macrolide orally |
| 19 | CAP (diabetic, outpatient) | Azithromycin appropriate for mild CAP |
| 20 | COPD GOLD 4 + cor pulmonale | O₂ therapy; nebulized bronchodilators; inhaled GCS; diuretics; heparin |
| 21 | COPD (emphysematous) | Long-acting anticholinergic (tiotropium); SABA PRN |
| 22 | Duodenal ulcer HP+ | PPI + clarithromycin + amoxicillin x14 days; De-Nol; GI bleed: surgery |
| 23 | Calculous cholecystitis | Laparoscopic cholecystectomy; UDCA; antispasmodics |
| 24 | Alcoholic pancreatitis exacerbation | Abstinence; drotaverine; analgesics; enzymes; insulin if DM |
| 25 | Biliary-dependent pancreatitis + pancreatogenic DM | PPIs; Creon; anticholinergics; antispasmodics; insulin |
| 26 | Atrophic gastritis HP+ | PPI + De-Nol + prokinetic; eradication (clarithromycin + amoxicillin) |
| 27 | GERD erosive esophagitis Stage II | PPI (rabeprazole) + prokinetics + antacids; lifestyle modification |
| 28 | Alcoholic hepatitis + cholestasis | Abstinence; S-adenosylmethionine; UDCA |
| 29 | GERD + erosive gastritis + HP | Rabeprazole x8 weeks; itopride; UDCA; HP eradication |
| 30 | PUD + GI bleed + post-MI (complex) | Pantoprazole/rabeprazole (not CYP450-metabolized); De-Nol; iron; EGDS |
| 31 | Ulcerative colitis moderate left-sided | Mesalazine 3-4.8 g/day oral + enemas; GCS if refractory |
| 32 | B12 deficiency anemia severe + funicular myelosis | Cyanocobalamin 500 mcg IM daily x1 week; blood transfusion |
| 33 | IDA severe (pica) | Oral iron 100-120 mg/day; consider IV iron |
| 34 | Acute leukemia | Bone marrow biopsy + immunophenotyping → chemotherapy; blood products |
| 35 | IDA mild + menorrhagia | Iron polymaltose 200 mg/day → reduce to 100 mg/day x4-6 months |
| 36 | B12 deficiency severe + angina | Cyanocobalamin 500 mcg IM; erythrocyte transfusion (anginal symptoms) |
| 37 | B12 deficiency + atrophic gastritis + cognitive decline | Cyanocobalamin 500 mcg IM x2 weeks; add folic acid; diet alone ineffective |
This is a shared conversation. Sign in to Orris to start your own chat.