Irida indetailed
Reading File
Finding Sources
Finding Sources
Searching PubMed
IRIDA iron-refractory iron deficiency anemia TMPRSS6
Searching the Web
IRIDA iron-refractory iron deficiency anemia TMPRSS6 hepcidin detailed review 2024 2025
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks plus current literature. Let me compile the detailed answer.
Iron-Refractory Iron Deficiency Anemia (IRIDA)
Definition
IRIDA is a rare autosomal recessive hereditary disorder of systemic iron homeostasis characterized by:
- Microcytic, hypochromic anemia
- Complete refractoriness to oral iron therapy
- Slow or partial response to parenteral (intravenous) iron
- Inappropriately elevated hepcidin levels relative to iron stores
It is distinct from common acquired iron deficiency anemia (IDA) in that it is genetic in origin, not due to blood loss, poor diet, or malabsorption of the gut mucosa per se.
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 592; Tietz Textbook of Laboratory Medicine, 7th Ed., p. 1375; Harrison's Principles of Internal Medicine, 22E
Genetics
| Feature | Detail |
|---|---|
| Gene | TMPRSS6 (chromosome 22q12-13) |
| Inheritance | Autosomal recessive (biallelic mutations required for full phenotype) |
| Protein encoded | Matriptase-2 (MT-2) - a type II transmembrane serine protease |
| Expression site | Liver (hepatocytes) |
| Mutation spectrum | >65 IRIDA families identified of different ethnic origins; both homozygous and compound heterozygous mutations reported |
| Monoallelic effects | Rarely, single-allele defects have been described; TMPRSS6 variants also confer susceptibility to acquired iron deficiency in the general population |
Molecular Pathophysiology
Understanding IRIDA requires knowledge of the hepcidin-ferroportin axis:
Normal Iron Regulation
- Hepcidin (encoded by HAMP) is the master regulator of systemic iron homeostasis, produced by hepatocytes
- Hepcidin binds to and induces internalization/degradation of ferroportin (the only known cellular iron export protein), found on duodenal enterocytes and macrophages
- When hepcidin is elevated: ferroportin is degraded → iron is trapped inside enterocytes and macrophages → less iron enters plasma → iron-restricted erythropoiesis
- When hepcidin is low (iron-deficient states): ferroportin is upregulated → increased intestinal absorption and macrophage iron release
The BMP-SMAD-HJV Pathway (Hepcidin Activation)
- BMP ligands (particularly BMP6) bind to BMP receptors along with the co-receptor hemojuvelin (HJV) on hepatocyte surfaces
- This activates the SMAD1/5/8 signaling cascade, which enters the nucleus and drives HAMP (hepcidin) gene transcription
Role of Matriptase-2 (TMPRSS6)
- Matriptase-2 is a protease that cleaves HJV from the hepatocyte surface, thereby dampening the BMP-SMAD pathway
- In conditions of iron deficiency, matriptase-2 is upregulated, HJV is cleaved, BMP signaling is reduced, and hepcidin falls - allowing maximum iron absorption
- In IRIDA: loss-of-function mutations in TMPRSS6 → non-functional matriptase-2 → HJV remains intact → BMP-SMAD pathway is constitutively active → inappropriately high hepcidin production even in the face of iron deficiency
- Elevated hepcidin → ferroportin degradation on enterocytes → iron retained within enterocytes, cannot be exported to plasma → functional block of intestinal iron absorption
- Oral iron is absorbed into enterocytes but cannot be exported across the basolateral membrane into the circulation
- IV iron bypasses this block (delivered directly to plasma), explaining the partial response to parenteral iron
Harrison's Principles of Internal Medicine, 22E, p. 808
Clinical Features
Presentation
- Can present at any age from infancy to adulthood, but often detected in childhood or early adulthood
- More severe cases tend to present in infancy/childhood
- Female predominance (due to additional iron demands from menstruation)
- Symptoms of chronic anemia: fatigue, pallor, exercise intolerance, poor growth (in children)
- No response to oral iron supplements - this is the hallmark clinical clue
Physical Examination
- Pallor
- Tachycardia in moderate-severe anemia
- Absence of signs of GI pathology (no malabsorption signs)
- Sometimes associated with alopecia (hair loss) - documented in mouse models and some human cases
Laboratory Findings
| Parameter | Typical Result in IRIDA |
|---|---|
| Hemoglobin | Low (variable severity, often moderate) |
| MCV | Low (microcytic, often <70 fL) |
| MCH | Low (hypochromic) |
| Serum iron | Very low |
| Transferrin saturation (TSAT) | Markedly low (<5-10%) |
| TIBC | Elevated |
| Serum ferritin | Low to low-normal (may normalize or slightly elevate after IV iron) |
| Serum hepcidin | Inappropriately elevated (key diagnostic clue) |
| Hepcidin/TSAT ratio | Markedly elevated |
| TSAT/hepcidin ratio | Markedly low (useful diagnostic biomarker) |
| Reticulocytes | Decreased (hypoproliferative) |
| Peripheral smear | Microcytic, hypochromic RBCs |
| ZPP (zinc protoporphyrin) | Elevated |
Diagnostic Biomarker
- A TSAT/hepcidin ratio that is very low strongly suggests IRIDA vs. regular IDA
- In regular IDA: low iron → low hepcidin → TSAT/hepcidin ratio is normal-to-high
- In IRIDA: low iron + high hepcidin → very low TSAT/hepcidin ratio
- Studies show this ratio has an AUC of ~0.88 for discriminating IRIDA from other causes of IDA, as noted in a 2022 study on transferrin saturation/hepcidin ratio discrimination
Diagnosis
Diagnostic Criteria
- Microcytic hypochromic anemia
- Very low TSAT (often <5%)
- Low-normal ferritin
- No/poor response to oral iron (after adequate trial)
- Partial response to IV iron
- Elevated hepcidin despite iron deficiency
- Confirmation: biallelic pathogenic mutations in TMPRSS6 (genetic testing)
Differential Diagnosis
| Condition | Ferritin | TSAT | Hepcidin | Response to oral Fe |
|---|---|---|---|---|
| IRIDA | Low-normal | Very low | High | None |
| Common IDA | Low | Low | Low | Good |
| Thalassemia trait | Normal-high | Normal | Normal | N/A (not iron-deficient) |
| Anemia of chronic disease | Normal-high | Low | High | Poor (but not primary cause) |
| Sideroblastic anemia | High | High | - | None (different etiology) |
Key distinguishing features from common IDA:
- Hepcidin is inappropriately high (should be low in iron deficiency)
- No response to oral iron despite compliance
- Family history (autosomal recessive - siblings may be affected)
- No identifiable cause of IDA (no GI blood loss, no malabsorption syndrome)
Tietz Textbook of Laboratory Medicine, 7th Ed., p. 1375
Treatment
Intravenous (IV) Iron
- First-line treatment for IRIDA
- Bypasses the blocked intestinal ferroportin, delivering iron directly into plasma
- Common preparations: ferric carboxymaltose, iron sucrose, low-molecular-weight iron dextran
- Response is typically partial - hemoglobin improves but may not normalize
- Repeat dosing is often required (every few months in severe cases)
- Hepcidin remains elevated even after IV iron, so effect is sustained only while iron load is being processed via macrophage recycling pathways
Oral Iron
- Ineffective - do not use as sole therapy
- Some very mild/heterozygous cases may show a partial response to high-dose oral iron, but this is not reliable
Supportive Management
- Folic acid supplementation in some cases
- Address any co-existing nutritional deficiencies
- In women: manage menstrual blood loss to reduce iron demand
Monitoring
- Hemoglobin, ferritin, TSAT at regular intervals
- Hepcidin levels to guide treatment
- Symptom assessment
Emerging/Experimental Therapies
- Anti-hepcidin antibodies / hepcidin antagonists: Block hepcidin action, potentially restoring ferroportin function and iron absorption
- TMPRSS6 upregulators: Theoretically boost matriptase-2 expression; currently experimental
- The same TMPRSS6 pathway is being investigated as a therapeutic target (inhibition) in disorders of iron overload such as beta-thalassemia (to increase hepcidin)
Henry's Clinical Diagnosis and Management, Harrison's 22E; Hoving et al., Br J Haematol, 2025
Mouse Models
- Tmprss6-knockout mice develop a phenotype closely mirroring human IRIDA: severe microcytic anemia, hepatic hepcidin overexpression, alopecia
- Duodenal enterocytes of knockout mice show decreased basolateral ferroportin protein - iron is retained within enterocytes, confirming the pathomechanism
- Both the anemia and alopecia were rescuable by iron administration in these models
Epidemiology and Clinical Relevance
- IRIDA is rare - exact prevalence unknown, but cases reported across multiple ethnicities worldwide
- Often underdiagnosed or misdiagnosed as refractory common IDA
- Patients frequently undergo unnecessary invasive workup (endoscopy, bone marrow biopsy) before the diagnosis is considered
- Recognizing IRIDA prevents costly, unhelpful investigations and directly changes management (oral iron → IV iron)
- TMPRSS6 variants in the general population may contribute to genetic susceptibility to iron deficiency even without full IRIDA - heterozygous carriers may have lower iron stores, especially with co-existing risk factors (menstruation, inflammation, infection)
Summary Table
| Feature | IRIDA |
|---|---|
| Gene | TMPRSS6 (chr 22q12-13) |
| Inheritance | Autosomal recessive |
| Protein | Matriptase-2 |
| Mechanism | Loss of HJV cleavage → high hepcidin → ferroportin degradation → blocked iron export |
| Key lab finding | High hepcidin + very low TSAT despite iron deficiency |
| Response to oral iron | None |
| Response to IV iron | Partial |
| Confirmation | Biallelic TMPRSS6 mutations |
| Treatment | IV iron (repeated dosing) |
Recent 2025 guidance from Hoving et al. in the British Journal of Haematology (PMID 39985323) provides expert-opinion-based treatment strategies for both children and adults with IRIDA, emphasizing patient-tailored IV iron regimens given the absence of formal international guidelines. Evidence-based international guidelines for IRIDA remain lacking as of 2025.
Generate a clinical decision-making flowchart for diagnosing iron-refractory anemia
Generating Image
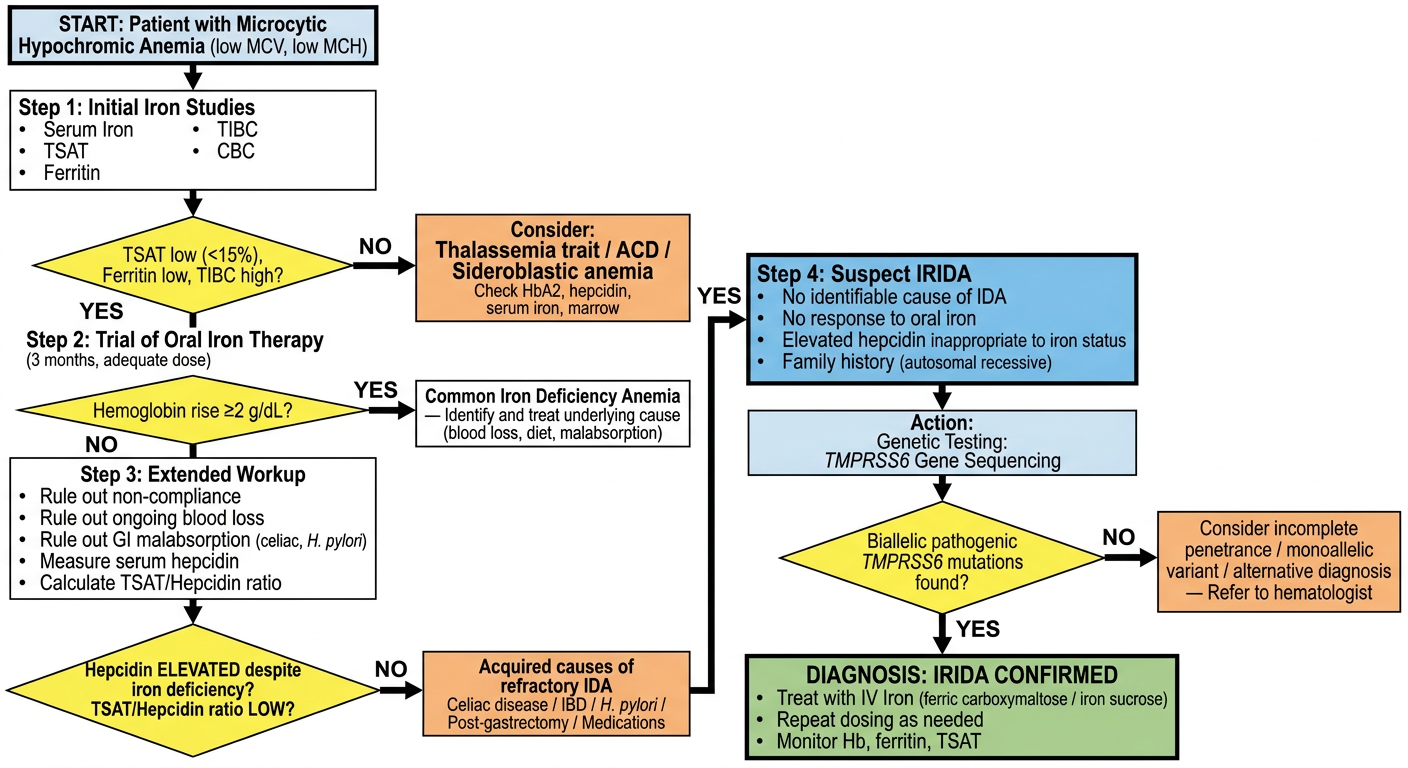
Here is the complete clinical decision-making flowchart for diagnosing iron-refractory anemia (IRIDA). The flowchart walks through five key diagnostic stages:
- Entry point - Microcytic, hypochromic anemia with initial iron studies
- First branch - Confirm typical IDA pattern (low TSAT, low ferritin, high TIBC) vs. other causes of microcytosis (thalassemia, ACD, sideroblastic anemia)
- Oral iron trial - 3-month adequate-dose trial; good responders exit as common IDA
- Extended workup - For non-responders: rule out non-compliance, GI blood loss, malabsorption; then measure serum hepcidin and calculate TSAT/hepcidin ratio - the key discriminating step
- IRIDA confirmation - Inappropriately high hepcidin without inflammation → genetic testing for biallelic TMPRSS6 mutations → confirmed IRIDA → IV iron therapy
Key diagnostic red flags for IRIDA:
- No identifiable cause of IDA after full workup
- Oral iron fails despite compliance
- Hepcidin elevated when it should be suppressed by iron deficiency
- Autosomal recessive family pattern
Mam child indetailed
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
moderate acute malnutrition children management
Searching the Web
moderate acute malnutrition MAM children WHO definition diagnosis treatment 2024
Finding Sources
Finding Sources
Reading Web Page
moderate acute malnutrition MAM children definition diagnosis treatment pathophysiology
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative content from multiple sources. Here is the full detailed answer on MAM in children.
Moderate Acute Malnutrition (MAM) in Children - Detailed Overview
1. Definition and Classification
Acute malnutrition (wasting) is defined by the WHO/UNICEF/World Bank as a life-threatening wasting disorder of children caused by poor nutrient intake and/or recurrent illness. It exists on a spectrum:
| Category | WHZ Score | MUAC (6 mo - 5 yr) | Clinical Signs |
|---|---|---|---|
| Normal | > -2 Z | ≥ 125 mm | None |
| MAM (Moderate Acute Malnutrition) | -3 to -2 Z | 115-125 mm | Wasting without edema |
| SAM (Severe Acute Malnutrition) | < -3 Z | < 115 mm | Severe wasting ± bilateral pitting edema |
MAM always corresponds to moderate wasting - it never involves nutritional edema (edema automatically classifies as SAM regardless of WHZ).
Sources: WHO Elena Guidelines; Robbins, Cotran & Kumar Pathologic Basis of Disease; Sleisenger & Fordtran's GI and Liver Disease
2. Global Burden
- ~32.8 million children under 5 years are affected by MAM globally
- In 2022, ~45 million children suffered wasting (6.8% of children under 5), of which ~13.6 million had SAM
-
75% of all wasted children live in Asia; ~22% in Africa
- Over 20% of children under 5 (~148 million) suffer stunting, which overlaps with chronic undernutrition
- MAM is the gateway to SAM - untreated MAM significantly increases risk of progression to SAM and death
Robbins, Cotran & Kumar Pathologic Basis of Disease
3. Classification Frameworks
Waterlow Classification (Weight for Height / Height for Age)
| Parameter | Normal | Mild | Moderate | Severe |
|---|---|---|---|---|
| Weight for Height (Wasting) - % of NCHS median | 90-100% | 80-89% | 70-79% | <70% |
| WHZ score | +Z to -Z | -1.1 to -2 Z | -2.1 to -3 Z | < -3 Z |
| Height for Age (Stunting) - % of NCHS median | 95-105% | 90-94% | 85-89% | <85% |
| HAZ score | +Z to -Z | -1.1 to -2 Z | -2.1 to -3 Z | < -3 Z |
MAM falls in the moderate wasting band: WHZ -2.1 to -3 Z.
Sleisenger & Fordtran's GI and Liver Disease, Table 5.16
4. Etiology and Risk Factors
Primary Causes
- Insufficient caloric/protein intake - inadequate food supply, poverty, food insecurity
- Early/inappropriate weaning - transitioning from breast milk to calorie-dense but protein-poor diets (e.g., carbohydrate-only porridge)
- Poor diet quality - monotonous diets lacking micronutrients (zinc, iron, vitamin A)
- Low birth weight / preterm birth - starting with depleted nutritional reserves
Secondary/Contributing Causes
- Recurrent infections - diarrhea, respiratory infections, malaria, measles all increase catabolism and reduce appetite (the malnutrition-infection cycle)
- Intestinal malabsorption - chronic diarrhea, parasitic infections (Giardia, hookworm), celiac disease
- Inadequate breastfeeding practices
- Poor water, sanitation, and hygiene (WASH) - enteric infections and environmental enteropathy
- Maternal malnutrition - in utero programming and poor breast milk composition
- Socioeconomic factors - poverty, food insecurity, displacement (refugees/humanitarian crises), inadequate caregiving
The Malnutrition-Infection Cycle
Malnutrition impairs immune function → increased susceptibility to infection → infections increase catabolism, reduce appetite, impair absorption → worsening malnutrition. This self-perpetuating cycle is the central driver of morbidity in MAM.
5. Pathophysiology
Protein and Energy Compartments
The body maintains two protein compartments that respond differently to malnutrition:
| Compartment | Represents | Affected in |
|---|---|---|
| Somatic | Skeletal muscle proteins | Primarily marasmus |
| Visceral | Liver and organ proteins (albumin, transferrin) | Primarily kwashiorkor |
In MAM (Moderate Wasting / Pre-Marasmic State)
- Caloric deficit develops over weeks to months
- Body mobilizes subcutaneous fat and muscle glycogen as initial energy reserves
- With ongoing deficit, muscle catabolism begins - providing amino acids for gluconeogenesis
- The somatic protein compartment is moderately depleted but not severely
- Visceral protein compartment (albumin) is largely preserved in pure wasting (MAM/marasmus)
- Leptin production falls → stimulates hypothalamic-pituitary-adrenal axis → elevated cortisol → promotes lipolysis and muscle catabolism
- Immune compromise: T-cell mediated immunity is impaired; secretory IgA levels fall; complement components decrease → increased vulnerability to infections
- Gut microbiome alterations have been documented - differences in microbial flora between malnourished and well-nourished children may play a pathogenic role
Comparison of MAM vs Marasmus vs Kwashiorkor

Fig. Childhood malnutrition. (A) Marasmus: severe loss of muscle mass and subcutaneous fat; head appears large relative to emaciated body. (B) Kwashiorkor: generalized edema (ascites, facial puffiness, pedal edema) with relative preservation of fat - Robbins, Cotran & Kumar Pathologic Basis of Disease
| Feature | MAM | Marasmus (Severe Wasting) | Kwashiorkor |
|---|---|---|---|
| Deficit type | Calories + protein (moderate) | Severe caloric deficit | Predominantly protein deficit |
| WHZ | -2 to -3 | < -3 | -2 to -3 (but edema present) |
| Edema | Absent | Absent | Present (bilateral pitting) |
| Subcutaneous fat | Reduced | Severely reduced | Relatively preserved |
| Muscle wasting | Moderate | Severe | Moderate |
| Serum albumin | Normal/borderline | Normal/slightly low | Markedly low |
| Mood | Alert | Alert | Apathetic/irritable |
| Appetite | Preserved | Good | Poor |
| Weight for age | 70-79% | <60% | 60-80% (masked by edema) |
| Fatty liver | Absent | Absent | Present |
| Skin/hair changes | Mild | Dry, lax, fine scaling | "Flaky paint" hyperpigmentation, flag sign in hair |
Sleisenger & Fordtran's GI Disease, Table 5.17; Robbins & Kumar
6. Clinical Features of MAM
Anthropometric
- Weight-for-height Z-score: -2 to -3
- MUAC: 115-125 mm (in 6 months to 5 years)
- Mid-arm muscle circumference: reduced (reflects somatic protein depletion)
- Skinfold thickness: reduced (reflects fat depletion)
Physical Examination
- General: Child is thin but alert and has preserved appetite (distinguishes from kwashiorkor)
- Skin: Dry, pale, slightly lax; mild scaling
- Hair: May be slightly dull; thin
- Muscles: Visibly reduced bulk, particularly in buttocks, thighs, shoulders
- Subcutaneous fat: Reduced in cheeks, limbs, abdomen
- No edema (presence of edema = SAM by definition)
- No hepatomegaly typically
- May have co-existing micronutrient deficiency signs (angular cheilitis from riboflavin, Bitot's spots from vitamin A, pallor from iron deficiency)
Co-morbidities
- Recurrent diarrhea
- Acute respiratory infections
- Malaria
- Anemia (iron, folate, B12)
- Vitamin A, zinc, iodine deficiencies are common co-morbidities
7. Diagnosis
Step 1 - Screening (Community Level)
- MUAC tape measurement: Simple, low-cost, performed by community health workers
- Green zone: ≥ 125 mm (normal)
- Yellow zone: 115-125 mm (MAM)
- Red zone: < 115 mm (SAM)
- Bilateral pitting edema check: Press thumbs on dorsum of both feet for 3 seconds - pitting = SAM (kwashiorkor)
Step 2 - Anthropometric Confirmation (Health Facility)
- Weight-for-height Z-score (WHZ): Requires weight scale and height board; compared against WHO Child Growth Standards 2006
- MUAC: Confirmatory measurement
- Weight for age and height for age to assess stunting alongside wasting
Step 3 - Clinical Assessment
- Full history: dietary intake, breastfeeding, illness episodes, immunization status
- Appetite test (offer RUTF - ready-to-use therapeutic food; good appetite = MAM / poor = SAM indicator)
- Check for bilateral edema
- Signs of infection (fever, respiratory rate, jaundice)
- Examination for micronutrient deficiency signs
Step 4 - Laboratory Tests (if available)
- Hemoglobin / complete blood count (anemia)
- Blood glucose (hypoglycemia risk in SAM but also MAM with illness)
- HIV testing (where indicated)
- Stool microscopy (parasites)
- Malaria RDT (endemic areas)
- Serum albumin (low in kwashiorkor, normal in MAM/marasmus)
Differential Diagnosis of Wasting in Children
- Chronic infection (TB, HIV)
- Malabsorption (celiac disease, cystic fibrosis, giardiasis)
- Congenital heart disease
- Chronic renal disease
- Inflammatory bowel disease
- Endocrine causes (diabetes mellitus type 1)
- Thalassemia / hemolytic anemias
8. Management of MAM
Core Principles
The management of MAM involves a continuum of care - treatment of MAM is inseparable from prevention of SAM. Management is primarily outpatient through Supplementary Feeding Programmes (SFP).
Setting
- MAM → Outpatient management (Supplementary Feeding Programme)
- SAM without complications → Outpatient (Community-based Management of Acute Malnutrition - CMAM)
- SAM with complications → Inpatient (Therapeutic Feeding Centre)
Nutritional Treatment
A. Dietary Counselling (All settings)
- Optimize local available foods: animal-source proteins, legumes, fortified cereals, vegetables
- Promote continued breastfeeding in children <2 years
- Increase meal frequency: 5-6 small meals/day
- Improve complementary feeding practices
B. Supplementary Foods (Context-dependent)
In settings with food insecurity or humanitarian crises, WHO recommends specially formulated supplementary foods:
| Product | Type | Use |
|---|---|---|
| Ready-to-Use Supplementary Food (RUSF) | Lipid-based, peanut-based paste | Primary supplementary food for MAM |
| Super Cereal Plus (CSB++) | Corn-soy blend + milk powder | Blanket supplementary feeding |
| Lipid-Based Nutrient Supplements (LNS-MQ) | Medium-quantity LNS | MAM treatment in community |
| Fortified blended foods (FBF) | Corn-soy blend | Supplementary feeding |
2023 WHO Update: WHO's updated guidelines (2023) now include the first-ever standards specifically for managing MAM, recommending that moderately malnourished children in humanitarian crises be prioritized for specially formulated supplementary foods to prevent progression to SAM.
Important caveat: Routine provision of supplementary foods to all moderately wasted children presenting to primary health care facilities is NOT recommended (risk of promoting unhealthy weight gain with non-targeted use). Supplementary foods are recommended when:
- High community prevalence of wasting
- Food insecurity at household/community level
- As part of an integrated care continuum
C. Micronutrient Supplementation
- Vitamin A supplementation (per national schedule; therapeutic dosing if deficiency signs present)
- Iron and folic acid if anemia is confirmed
- Zinc supplementation (especially during diarrheal illness)
- Iodine (via iodized salt)
- Multivitamin formulations in some protocols
D. Treatment of Concurrent Illness
- Antibiotics for confirmed infections (not routinely prophylactic in MAM, unlike SAM)
- Anti-malarial treatment if malaria confirmed
- Antihelminthics (mebendazole/albendazole) if parasitic infection present or in endemic areas
- Oral rehydration for diarrhea
- Vaccination catch-up (especially measles, which causes acute nutritional deterioration)
Modified Dosage Strategy (2023 WHO Innovation)
A new WHO-endorsed option modifies RUTF dosages for children recovering from SAM (transitioning to MAM status) - allowing more efficient use of limited therapeutic food supplies while maintaining safety and efficacy.
Community Health Worker (CHW) Role (2023 WHO Endorsement)
In 2023, WHO endorsed treatment of acute malnutrition by community health workers outside health facilities. Evidence (notably from Action Against Hunger programs) shows CHW-delivered programs achieve cure rates similar to nursing staff at health facilities, at lower cost and with greater coverage. CHWs must be integrated as formal health workers with adequate training and supervision.
9. Monitoring Response
Frequency
- Weekly or bi-weekly visits during supplementary feeding
Response Criteria (Discharge from MAM programme)
- WHZ > -2 (or MUAC ≥ 125 mm)
- No bilateral edema
- Minimum stay of 8 weeks (to ensure sustained recovery)
- No acute illness
Failure to Respond (Transfer criteria to SAM programme)
- Deterioration: WHZ falls to < -3 or MUAC < 115 mm
- Development of bilateral edema
- Development of medical complications
- No weight gain after 4 weeks
10. Consequences of Untreated MAM
Short-term
- Progression to SAM (2-3x increased risk)
- Increased mortality from common infections (pneumonia, diarrhea, malaria)
- Prolonged hospitalization
Long-term (if MAM occurs in early life)
- Stunting (impaired linear growth) - permanent height deficit
- Neurocognitive impairment - reduced brain development, lower IQ, poor school performance
- Impaired immunity - increased lifetime susceptibility to infection
- Metabolic programming - paradoxically increased risk of obesity, type 2 diabetes, and cardiovascular disease later in life (if high-energy foods given non-selectively during recovery - the "thrifty phenotype" hypothesis)
WHO Elena Guidelines 2023; Robbins, Cotran & Kumar Pathologic Basis of Disease
11. Prevention
| Strategy | Mechanism |
|---|---|
| Exclusive breastfeeding for 6 months | Optimal nutrition + immune protection |
| Appropriate complementary feeding from 6 months | Prevent dietary gap |
| Fortification of staple foods | Address micronutrient deficiencies at scale |
| WASH (water, sanitation, hygiene) | Reduce infection burden |
| Growth monitoring (monthly weight checks) | Early detection |
| Vaccination programs | Reduce measles and other infections that precipitate acute wasting |
| Social protection / cash transfers | Address household food insecurity |
| Maternal nutrition programs | Prevent low birth weight and in utero malnutrition |
12. Recent Evidence
A 2023 systematic review and meta-analysis by Padhani et al. (PMID 37686813) in Nutrients comprehensively reviewed management of moderate wasting in children >6 months, supporting evidence-based supplementary feeding approaches.
A 2025 review by Bita (PMID 40341873) evaluated simplified approaches to acute malnutrition care, supporting integrated SAM+MAM management protocols to improve coverage in resource-limited settings.
Summary
| Feature | MAM |
|---|---|
| Definition | WHZ -2 to -3 OR MUAC 115-125 mm, no edema |
| Pathology | Moderate caloric/protein deficit; somatic wasting; preserved visceral proteins |
| Key clinical signs | Wasting (muscle/fat loss), alert, good appetite, no edema |
| Diagnosis | MUAC + WHZ + clinical assessment |
| Treatment setting | Outpatient (Supplementary Feeding Programme) |
| Nutrition | Dietary counselling ± RUSF/LNS in food-insecure contexts |
| Micronutrients | Vitamin A, iron, zinc as indicated |
| Monitoring | Bi-weekly; discharge when WHZ > -2 |
| If worsens | Transfer to SAM protocol |
| Prevention | Breastfeeding, complementary feeding, WASH, vaccines, social protection |
This is a shared conversation. Sign in to Orris to start your own chat.