

Decide a treatment line according to these reports wuth drug dosage
Reading File
Finding Sources
Finding Sources
Searching PubMed
type 2 diabetes HbA1c 8 treatment guidelines metformin
Reading File
Reading File
Searching PubMed
type 2 diabetes metformin dual therapy HbA1c
Reading File
Finding Sources
Reading File
I now have all the information needed to provide a thorough treatment recommendation. Here is the complete analysis:
Patient Summary - Mr. Sandeep Soni Ji, 58Y/M
Lab Results at a Glance
| Parameter | Result | Status |
|---|---|---|
| HbA1c | 8.32% | Diabetic - "Action suggested" (>8%) |
| Average Blood Glucose | 192.08 mg/dL | Poor control (>180) |
| Total Cholesterol | 168.64 mg/dL | Normal (<200) |
| Serum Triglycerides | 171.96 mg/dL | Borderline High (150-199) |
| HDL | 48.32 mg/dL | Normal |
| LDL | 85.93 mg/dL | Normal |
| VLDL | 34.39 mg/dL | Normal |
| Cholesterol/HDL Ratio | 3.49 | Low Risk |
| LDL/HDL Ratio | 1.78 | Low Risk |
Treatment Plan
Problem 1: Type 2 Diabetes - Poorly Controlled (HbA1c 8.32%)
An HbA1c of 8.32% crosses the "action suggested" threshold. The ABG of 192 mg/dL confirms poor glycemic control. Target for a 58-year-old male without known severe comorbidities should be HbA1c <7.0% (standard goal) or up to 7-8% if risk factors warrant a relaxed target.
Since this patient likely requires dual oral therapy to bring HbA1c down by ~1.3%, the recommended approach is:
Step 1 - Lifestyle Modification (mandatory alongside medications):
- Low-carbohydrate diet, reduced refined sugars and saturated fats
- 30 min moderate exercise 5 days/week
- Target 5-7% weight reduction if overweight
Step 2 - Dual Oral Antidiabetic Therapy:
Drug 1: Metformin (first-line)
- Start: Metformin 500 mg once daily with dinner (to minimise GI side effects)
- Titrate after 1-2 weeks: Metformin 500 mg twice daily with meals
- Target dose: Metformin 1000 mg twice daily (2000 mg/day total), max 2550 mg/day
- Check renal function (eGFR) before starting; hold if eGFR <30 mL/min
- Monitor Vitamin B12 annually on long-term use
(Goldman-Cecil Medicine, p.2478 - "Metformin is the preferred initial therapy for type 2 diabetes")
Drug 2 (add-on): DPP-4 Inhibitor (preferred in this patient profile)
Given HbA1c 8.32% with no mention of established cardiovascular disease or CKD, a DPP-4 inhibitor is a safe, weight-neutral second agent:
- Sitagliptin 100 mg once daily (most studied), OR
- Vildagliptin 50 mg twice daily, OR
- Teneligliptin 20 mg once daily (widely used in South Asia, affordable)
DPP-4 inhibitors reduce HbA1c by ~0.5-0.8%, have low hypoglycemia risk, and are well tolerated.
Alternatively, if the patient has cardiovascular risk factors or is overweight, an SGLT-2 inhibitor is preferred as the second agent:
- Dapagliflozin 10 mg once daily in the morning, OR
- Empagliflozin 10 mg once daily
- These also lower triglycerides and body weight - particularly useful given his borderline hypertriglyceridemia
(Goldman-Cecil Medicine, p.2479 - "SGLT2 inhibitors are now considered the second drug after metformin in patients with atherosclerotic cardiovascular disease, heart failure, or CKD")
Recent evidence supports this dual approach - a 2026 meta-analysis (PMID: 41676958) confirmed SGLT2i as add-on to metformin improves glycemic outcomes vs other oral agents; a 2026 meta-analysis (PMID: 42216339) supports triple therapy if dual therapy fails.
Problem 2: Borderline Hypertriglyceridemia (TG 171.96 mg/dL)
TG of 171.96 mg/dL falls in the borderline-high range (150-199 mg/dL). This is likely secondary to poorly controlled diabetes (hyperglycemia drives hepatic TG synthesis). Cholesterol, LDL, and HDL are within acceptable range, so no statin is needed right now.
First-line: Non-pharmacologic
- Eliminate alcohol, refined carbohydrates, and fruit juices
- Increase omega-3 rich foods (fish, flaxseed)
- Aerobic exercise
- Improved glycemic control alone will likely reduce triglycerides significantly
Pharmacologic (if TG remains >200 mg/dL after 3 months glycemic control):
- Fenofibrate 145 mg once daily (preferred over gemfibrozil when combined with statins if statin becomes needed later), OR
- Omega-3 fatty acids (EPA+DHA) 1-2 g/day as dietary supplement; prescription-grade 4 g/day if TG >500 mg/dL
(Washington Manual of Medical Therapeutics: "Fibrates lower TG by 30-50%; fenofibrate 48-145 mg/day PO")
Do NOT start a fibrate concurrently with a statin without monitoring for myopathy.
Summary Prescription
| Drug | Dose | Timing | Indication |
|---|---|---|---|
| Metformin 500 mg | Start 500 mg OD, titrate to 1000 mg BD | With meals | Diabetes - first line |
| Sitagliptin 100 mg or Dapagliflozin 10 mg | 100 mg OD or 10 mg OD | Morning | Diabetes - add-on (pick one) |
| Fenofibrate 145 mg | 145 mg OD | With food | Only if TG >200 after 3 months |
| Omega-3 1-2 g/day | 1-2 capsules OD | With meal | Borderline TG - optional now |
Follow-Up
- Repeat HbA1c in 3 months to assess response
- Fasting lipid profile in 3 months - if TG normalises with glycemic control, no lipid drug needed
- Check renal function, liver enzymes, CBC before starting therapy
- Counsel on diet, weight loss, and exercise as the most impactful interventions at this HbA1c level
Important disclaimer: This recommendation is based on the lab values provided. The treating physician must correlate with the patient's full clinical history, current medications, renal/hepatic function, cardiovascular status, and contraindications before prescribing.
Scorpion bite management
Reading File
Finding Sources
Searching PubMed
scorpion envenomation management treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, authoritative information from four major textbooks. Here is the complete management guide:
Scorpion Bite (Sting) Management
Pathophysiology of Venom
Scorpion venom contains neurotoxins that keep neuronal sodium channels open, causing prolonged and excessive depolarization of somatic and autonomic (both sympathetic and parasympathetic) nervous systems. It also contains hemolysins, phospholipase A, and coagulins. The toxin is more potent per unit weight than most snake venoms.
Key dangerous species to know (especially in South Asia):
- Mesobuthus tamulus - India, Nepal, Pakistan - massive catecholamine release, cardiovascular toxicity
- Androctonus spp. - Middle East, North Africa - pulmonary edema, arrhythmias
- Leiurus quinquestriatus - Middle East/North Africa
- Tityus spp. - South America (also causes pancreatitis)
- Centruroides sculpturatus - USA (Southwest) - neurotoxic
- Hemiscorpius lepturus - Iran - cytotoxic, causes hemolysis + AKI
Clinical Grading (Centruroides / Severity-Based)
| Grade | Clinical Features | Antivenom |
|---|---|---|
| 1 | Local pain and paresthesia at sting site only | No |
| 2 | Local + remote pain and paresthesias | No |
| 3 | Cranial nerve OR neuromuscular dysfunction (drooling, abnormal eye movements, slurred speech, jerking, tachycardia, diaphoresis) | Yes |
| 4 | Cranial nerve AND neuromuscular dysfunction | Yes |
Clinical Features by System
| System | Signs & Symptoms |
|---|---|
| Local | Burning pain, paresthesia, hyperesthesia, redness, swelling; "tap test" positive (tapping sting site worsens pain) |
| Neuromuscular | Restlessness, involuntary jerking/writhing, muscle twitching (can mimic seizure), opisthotonos |
| Cranial Nerve | Blurred vision, abnormal eye movements, slurred speech, dysphagia, hypersalivation, rhinorrhea |
| Autonomic (Sympathetic) | Tachycardia, hypertension, diaphoresis, mydriasis, pulmonary edema, myocardial injury |
| Autonomic (Cholinergic) | Bradycardia, salivation, abdominal pain, diarrhea (mainly Tityus spp.) |
| Cardiovascular | Arrhythmias, hypertensive crisis, pulmonary edema, cardiogenic shock |
| Severe/Fatal | Respiratory arrest (especially children/elderly), rhabdomyolysis, AKI, multiorgan failure |
Management
Step 1 - Immediate First Aid (at scene)
- Keep the patient calm - agitation worsens venom absorption
- Pressure dressing + cold/ice pack to sting site - slows venom absorption
- Do NOT cut, suck, or apply tourniquet routinely (older forensic texts recommend tourniquet; modern EM guidelines do not endorse this for most envenomations)
- Remove clothing/footwear in case scorpion is still present
- Tetanus prophylaxis if not current on immunization
- Transport to emergency department immediately for grade 2+
Step 2 - Initial Assessment in ED
- History: Species if known, time of sting, progression of symptoms, age, weight (especially in children)
- Vitals: HR, BP, RR, SpO2, temperature
- Tap test: Tapping sting site - increased pain/paresthesia suggests significant envenomation
- Labs (for severe envenomation): CBC, metabolic panel, renal function, cardiac enzymes, ABG, urinalysis (myoglobinuria/hemoglobinuria), lipase (if Tityus suspected)
- ECG in all patients with cardiovascular symptoms
Step 3 - Pharmacologic Treatment by Effect
| Clinical Problem | Drug | Dose/Route |
|---|---|---|
| Local pain only (Grade 1-2) | Acetaminophen | 500-1000 mg PO every 6h |
| NSAIDs (Ibuprofen) | 400 mg PO every 8h | |
| Local lidocaine (without epinephrine) | Infiltrate around sting site | |
| Moderate/Severe pain | Fentanyl or Morphine | IV, titrated; monitor closely for respiratory depression |
| Agitation / Neuromuscular hyperactivity | Midazolam (preferred) | 0.05-0.1 mg/kg IV infusion; continuous if needed |
| Diazepam | 0.1-0.2 mg/kg IV; repeat as needed | |
| Tachycardia / Hypertension / Catecholamine excess | Prazosin (alpha-blocker) | 0.5 mg PO (child <5 yrs), 1 mg PO (>5 yrs/adult); may repeat every 3h - drug of choice in India for M. tamulus stings |
| Nifedipine | 10 mg sublingual/oral for hypertensive urgency | |
| Nitroprusside | IV infusion for hypertensive emergency with pulmonary edema | |
| Nitroglycerin | IV/sublingual for pulmonary edema (reduces preload/afterload) | |
| Pulmonary edema + cardiogenic shock | Dobutamine | IV infusion (use caution if vasodilators also given) |
| Cholinergic effects (bradycardia, salivation, diarrhea) | Atropine | 0.5-1 mg IV; repeat every 5 min to effect (mainly Tityus/Parabuthus stings) |
| Airway secretions / hypersalivation | Atropine | Reduces secretions in neurotoxic cases too |
Prazosin is the cornerstone of management in India for cardiovascular compromise from Mesobuthus tamulus stings - it blocks the catecholamine storm responsible for pulmonary edema and hypertension. (Rosen's Emergency Medicine)
Step 4 - Antivenom
- Indication: Grade 3 and 4 envenomations (cranial nerve or neuromuscular dysfunction)
- Mechanism: Antivenom binds circulating toxin - most effective when given early, before toxin binds to tissue
- Note: Antivenom does NOT reverse established injury, it prevents further toxin binding
| Species/Region | Antivenom |
|---|---|
| Centruroides (USA) | Anascorp - equine F(ab')2 IgG - FDA approved |
| India (Mesobuthus tamulus) | Scorpion antivenom (available from Haffkine Institute, Mumbai; VINS Bioproducts) |
| Middle East/North Africa | Species-specific antivenoms by country |
Anascorp dosing (Centruroides):
- Initial: 3 vials IV as soon as possible after envenomation
- Additional: 1 vial IV every 30-60 minutes as needed for persisting symptoms
Indian scorpion antivenom:
- 10 mL IV (1 vial) diluted in normal saline over 30 minutes; repeat if symptoms persist
- Best given within the first few hours of envenomation
Step 5 - Supportive Care
- Airway: Be prepared for early intubation in children, elderly, or those with pharyngeal dysfunction + hypersalivation
- IV access: Establish immediately in all moderate-severe cases
- Oxygen: Supplemental O2 for all; mechanical ventilation if respiratory compromise
- Fluids: IV NS for hypotension, rhabdomyolysis (target urine output 200-300 mL/hr if myoglobinuria present)
- Cardiac monitoring: Continuous ECG in all moderate-severe cases
- Dangerous bradyarrhythmias: Atropine 0.5-1 mg IV
Disposition
| Severity | Disposition |
|---|---|
| Grade 1 - Local only | Observe 2-4 hours; discharge home with return precautions |
| Grade 2 - Remote pain/paresthesia | Observe 4-6 hours; discharge if stable |
| Grade 3-4 / Systemic toxicity | Admit to ICU/monitored bed |
| Children with ANY systemic symptom | Admit (higher risk of fatal respiratory arrest) |
| Hemolysis / AKI (H. lepturus) | Admit; watch for hemoglobinuria, dialysis if needed |
Key Points for India (South Asia context)
- Prazosin is the mainstay for cardiovascular management of M. tamulus stings - start early at first sign of autonomic storm
- Scorpion antivenom + Prazosin combination is superior to either alone for cardiovascular compromise (Rosen's Emergency Medicine)
- Children are disproportionately affected - low threshold for ICU admission
- Scorpion antivenom is available at most district/government hospitals in high-envenomation zones (Maharashtra, Rajasthan, Gujarat)
- Monitor for pulmonary edema even in initially stable patients - can develop within 1-2 hours
Sources: Harrison's Principles of Internal Medicine 22E (2025), Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, PC Dikshit Forensic Medicine & Toxicology | Systematic Review on scorpion myocarditis: PMID 37018229
Explsin me insulin therapy and how to dose different kinds of insulin
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
I now have comprehensive data from Goldman-Cecil, Harrison's, Katzung, Lippincott, and Washington Manual. Here is the full, detailed explanation:
Insulin Therapy - Complete Guide
1. Why Insulin is Used
Insulin is the hormone produced by pancreatic beta cells that lowers blood glucose by facilitating glucose uptake into cells. It is mandatory in Type 1 DM (no beta cells remain) and used in Type 2 DM when oral agents fail to achieve glycemic targets.
Goals of insulin therapy:
- HbA1c <7.0% for most patients
- Fasting glucose: 80-130 mg/dL
- Post-meal glucose: <180 mg/dL
2. Types of Insulin - The Full Spectrum
The chart below shows graphically how each insulin type behaves over time:
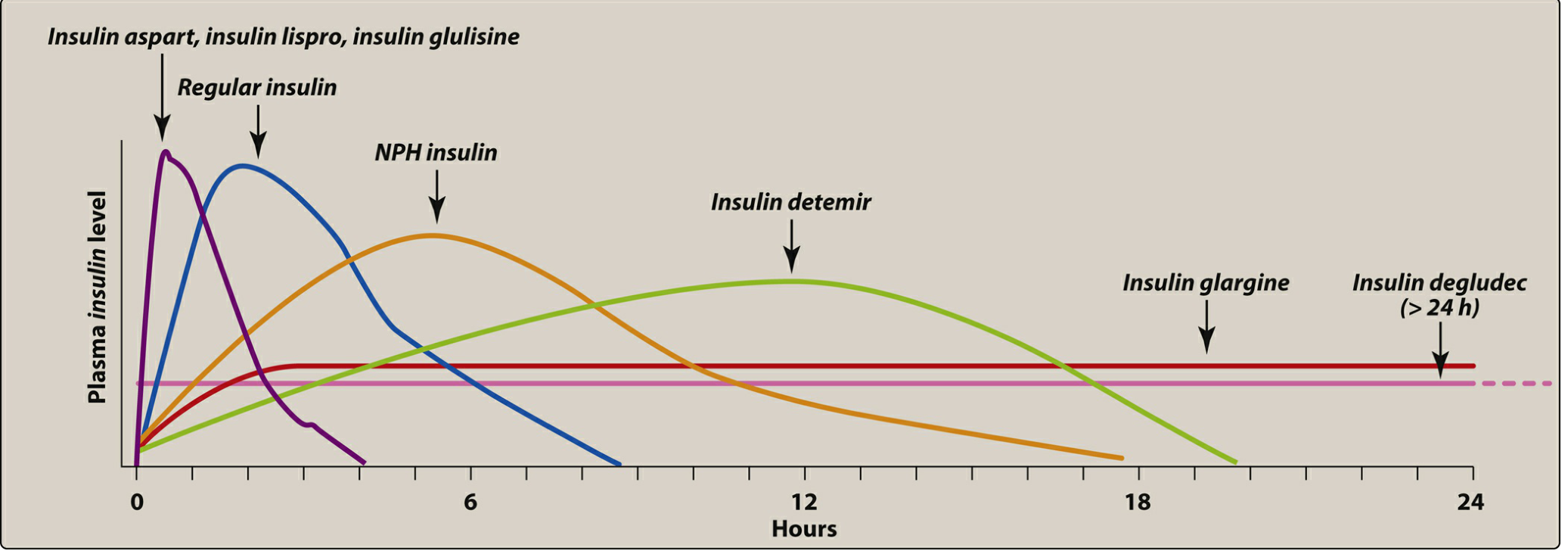
Insulin Pharmacokinetics Table
| Category | Insulin | Onset | Peak | Duration | Route |
|---|---|---|---|---|---|
| Rapid-Acting | Lispro (Humalog) | 5-15 min | 30-90 min | 3-4 h | SC / pump |
| Aspart (NovoLog/Fiasp) | 5-15 min | 1-1.5 h | 3-4 h | SC / pump | |
| Glulisine (Apidra) | 5-15 min | 1-1.5 h | 3-4 h | SC / pump | |
| Inhaled insulin | 5-15 min | 10-20 min | 3 h | Inhaled | |
| Short-Acting | Regular (Humulin R / Novolin R) | 30-60 min | 2-4 h | 6-8 h | SC / IV / IM |
| Intermediate-Acting | NPH (Humulin N / Novolin N) | 2-4 h | 6-10 h | 10-20 h | SC only |
| Long-Acting (Basal) | Glargine U100 (Lantus) | 0.5-2 h | Peakless (flat) | ~24 h | SC only |
| Glargine U300 (Toujeo) | 0.5-2 h | Peakless (flat) | 30-36 h | SC only | |
| Detemir (Levemir) | 0.5-1 h | Peakless (flat) | 17-20 h | SC only | |
| Degludec U100/U200 (Tresiba) | 0.5-1.5 h | Peakless (flat) | >42 h | SC only |
Key rule: Long-acting insulins (glargine, detemir, degludec) must NEVER be mixed in the same syringe with other insulins - mixing alters their pharmacodynamic profile.
3. The Concept: Basal-Bolus Physiology
The pancreas normally secretes insulin in two patterns:
- Basal secretion - continuous low-level secretion all day to suppress hepatic glucose output between meals and overnight
- Bolus (prandial) secretion - large spike at every meal to handle post-meal glucose
Physiologic insulin replacement mimics this by:
- Basal insulin (long-acting) = background glucose control
- Bolus insulin (rapid-acting) = mealtime glucose spikes
4. Insulin Regimens
Regimen 1: Basal Insulin Only (Starting point for Type 2)
Used when oral agents are insufficient but full insulin replacement is not yet needed.
Drug: Glargine (Lantus) or Degludec (Tresiba)
Dose:
- Start: 10 units SC at bedtime (or 0.1-0.2 units/kg/day)
- Bedtime dosing is preferred for Type 2 because fasting hyperglycemia and hepatic glucose excess are the main problems
- Titration ("treat to target"): Increase by 2 units every 3 days until fasting glucose reaches 80-130 mg/dL
- Glargine given at bedtime has less nocturnal hypoglycemia than NPH
Regimen 2: Basal + Bolus (Intensified / Basal-Bolus Regimen)
The physiologic gold standard. Used in Type 1 DM (always) and Type 2 DM when basal alone is not enough.
Step 1 - Calculate Total Daily Dose (TDD)
| Patient Type | Starting TDD |
|---|---|
| Type 1, newly diagnosed / insulin-naive | 0.3-0.5 units/kg/day |
| Type 2, insulin-naive | 0.3-0.5 units/kg/day |
| Type 1, established (average) | 0.5-1.0 units/kg/day |
| Type 2, obese / insulin resistant | 0.5-1.0 units/kg/day (may need higher) |
Example: 70 kg patient → TDD = 70 × 0.5 = 35 units/day
Step 2 - Split TDD into Basal and Bolus
- 50% as Basal (long-acting, once daily) = 17-18 units glargine/degludec at bedtime
- 50% as Bolus (rapid-acting, divided across 3 meals) = ~6 units per meal
Step 3 - Bolus Dose Timing
| Insulin | When to inject |
|---|---|
| Rapid-acting (lispro, aspart, glulisine) | 15 minutes before a meal (or within 15-20 min after starting the meal) |
| Regular insulin | 30 minutes before a meal |
Regimen 3: NPH-Based (Twice-Daily / "Standard" Regimen)
Older, less flexible regimen. Two injections per day. Common where cost is a concern.
- NPH + Regular in the morning (before breakfast)
- NPH + Regular in the evening (before dinner)
- Premixed 70/30 (70% NPH + 30% Regular): Given twice daily - convenient but less adjustable
Regimen 4: Insulin Pump (CSII - Continuous Subcutaneous Insulin Infusion)
- Only rapid-acting insulin is loaded into the pump
- Delivers a variable basal rate throughout the day (programmed by the clinician)
- Patient enters meal carbohydrates → pump calculates and delivers the bolus automatically
- Reduces HbA1c by an additional 0.3-0.5% vs multiple daily injections
- Also reduces severe hypoglycemia risk
- Requires expert supervision and patient education
5. Dose Calculation Tools
Correction Factor (Insulin Sensitivity Factor)
Used to calculate a corrective dose when blood glucose is above target.
Formula:
Correction Factor = 1500 ÷ Total Daily Dose (TDD)
Example: Patient on 50 units/day total → 1500 ÷ 50 = 30
This means 1 unit of insulin will drop blood glucose by ~30 mg/dL.
Correction dose = (Actual BG - Target BG) ÷ Correction Factor
If BG = 250 mg/dL, target = 120 mg/dL, CF = 30: Correction = (250 - 120) ÷ 30 = 4.3 units extra
Insulin-to-Carbohydrate Ratio (ICR)
Used for bolus dosing based on meal size.
Formula:
ICR = 500 ÷ TDD
Example: TDD = 50 → ICR = 500 ÷ 50 = 10
→ 1 unit covers 10 grams of carbohydrate
6. Monitoring and Adjustment
| Parameter | When to Check | Target |
|---|---|---|
| Fasting glucose | Every morning | 80-130 mg/dL |
| Pre-meal glucose | Before each meal | 80-130 mg/dL |
| Post-meal (2h) glucose | 2h after meals | <180 mg/dL |
| Bedtime glucose | Before sleep | 100-140 mg/dL |
| HbA1c | Every 3 months | <7.0% |
| Urine/blood ketones | When BG >250 mg/dL unexpectedly | Negative |
7. Hypoglycemia - The Main Risk
Definition: Blood glucose <70 mg/dL
Severe hypoglycemia: Patient unable to self-treat
Treatment of mild-moderate hypoglycemia (Rule of 15):
- Give 15g fast-acting carbohydrate (4 glucose tablets, 150 mL juice, 3-4 teaspoons sugar)
- Recheck glucose in 15 minutes
- Repeat if still <70 mg/dL
Treatment of severe hypoglycemia:
- Glucagon 1 mg IM/SC (if unconscious / unable to swallow)
- Or 50 mL of 50% dextrose IV in hospital setting
8. Special Considerations
| Situation | Adjustment |
|---|---|
| Illness / surgery | Do not stop basal insulin; check glucose more frequently; may need dose increase |
| Exercise | Reduce bolus for meal before exercise; reduce basal by 20-50% if prolonged activity |
| Renal impairment | Reduce dose (kidneys clear insulin); degludec and glargine preferred over NPH |
| Elderly | Relaxed HbA1c target (7-8%); avoid NPH (erratic absorption risk) |
| Pregnancy | Regular or rapid-acting analogues preferred; NPH for basal; avoid glargine (limited safety data) |
| Intensive vs Standard | Intensive (3+ injections/day) reduces microvascular complications but increases hypoglycemia risk; not for elderly, hypoglycemia unawareness, or advanced complications |
9. Adjunct: Pramlintide (Amylin Analog)
- Given SC immediately before meals as an add-on to mealtime insulin
- Reduces post-meal glucose, lowers HbA1c by 0.3-0.5%, and promotes weight loss
- When starting pramlintide, reduce mealtime insulin dose by 50% to avoid severe hypoglycemia
- Starting dose: 15 mcg SC; titrate up to 120 mcg maintenance
Sources: Goldman-Cecil Medicine International Edition; Harrison's Principles of Internal Medicine 22E (2025); Katzung's Basic & Clinical Pharmacology 16E; Lippincott Illustrated Reviews: Pharmacology; Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.