Can you make easy understanding on ABG and it's important and how we correct acidosis and alkalosis in body it's important in icu and how we can remember everything pls give good notes to understand
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the content I need to write excellent, comprehensive ABG notes. Let me compose the full response.
ABG (Arterial Blood Gas) - Complete ICU Notes
Quick Reference: Normal Values
| Parameter | Normal Value | What it Means |
|---|---|---|
| pH | 7.35 - 7.45 | Acid-base balance |
| PaCO2 | 35 - 45 mmHg | Lung function ("respiratory acid") |
| HCO3- | 22 - 26 mEq/L | Kidney function ("metabolic base") |
| PaO2 | 80 - 100 mmHg | Oxygen in blood |
| SaO2 | 95 - 100% | Oxygen saturation |
| Base Excess | -2 to +2 | Extra acid or base |
Memory trick: "The kidneys hold the HCO3-, the lungs hold the CO2"
Why ABG Matters in the ICU
ABG gives you a real-time window into 3 critical systems at once:
- Oxygenation (PaO2, SaO2)
- Ventilation (PaCO2)
- Acid-base status (pH, HCO3-, CO2)
A single ABG can tell you whether a patient needs intubation, is heading toward respiratory failure, has a metabolic crisis (sepsis, DKA, renal failure), or needs bicarbonate. Acid-base disturbances can be life-threatening - severe disorders alter hydrogen bonds, protein structures, and enzyme function, leading to cellular compromise and death within hours. - Rosen's Emergency Medicine
The Henderson-Hasselbalch Equation (Don't Memorize, Understand It)
pH = pK + log ([HCO3-] / 0.03 × PaCO2)
Simple version to remember:
pH = Kidneys (HCO3-) / Lungs (CO2)
- If HCO3- goes up or CO2 goes down → pH rises (alkalosis)
- If HCO3- goes down or CO2 goes up → pH falls (acidosis)
Step-by-Step ABG Interpretation (The 5-Step System)
STEP 1: Look at the pH
- pH < 7.35 = Acidosis
- pH > 7.45 = Alkalosis
- pH 7.35-7.45 = Normal (but may still have a compensated disorder!)
STEP 2: Look at PaCO2 (respiratory component)
- PaCO2 > 45 = too much CO2 = Respiratory Acidosis
- PaCO2 < 35 = too little CO2 = Respiratory Alkalosis
STEP 3: Look at HCO3- (metabolic component)
- HCO3- < 22 = not enough buffer = Metabolic Acidosis
- HCO3- > 26 = too much buffer = Metabolic Alkalosis
STEP 4: Match to the pH (which is the PRIMARY problem?)
The primary disorder is the one that matches the pH direction:
| pH | CO2 | HCO3- | Diagnosis |
|---|---|---|---|
| Low | High | Normal/High | Respiratory Acidosis |
| High | Low | Normal/Low | Respiratory Alkalosis |
| Low | Normal/Low | Low | Metabolic Acidosis |
| High | Normal/High | High | Metabolic Alkalosis |
STEP 5: Check for Compensation (Is the body compensating?)
This is the advanced step - the body always tries to compensate back toward normal pH.
Compensation Formulas (The ICU Must-Know Table)
From Harrison's Principles of Internal Medicine, 22nd Ed.
| Primary Disorder | Compensation Formula |
|---|---|
| Metabolic Acidosis | Expected PaCO2 = (1.5 × HCO3-) + 8 ± 2 (Winter's Formula) |
| Metabolic Alkalosis | PaCO2 rises 0.75 mmHg per 1 mmol/L rise in HCO3- |
| Respiratory Acidosis - Acute | HCO3- rises 1 mEq/L per 10 mmHg rise in CO2 |
| Respiratory Acidosis - Chronic | HCO3- rises 4 mEq/L per 10 mmHg rise in CO2 |
| Respiratory Alkalosis - Acute | HCO3- falls 2 mEq/L per 10 mmHg fall in CO2 |
| Respiratory Alkalosis - Chronic | HCO3- falls 5 mEq/L per 10 mmHg fall in CO2 |
Key rule: If the compensation is MORE or LESS than predicted = mixed disorder!
Winter's Formula (star formula for ICU)
Expected PaCO2 = (1.5 × HCO3-) + 8 ± 2
- If measured PaCO2 is higher than expected → also has respiratory acidosis
- If measured PaCO2 is lower than expected → also has respiratory alkalosis
- Normocapnia with severe metabolic acidosis = danger sign - suggests impending respiratory failure - Roberts & Hedges' Clinical Procedures in Emergency Medicine
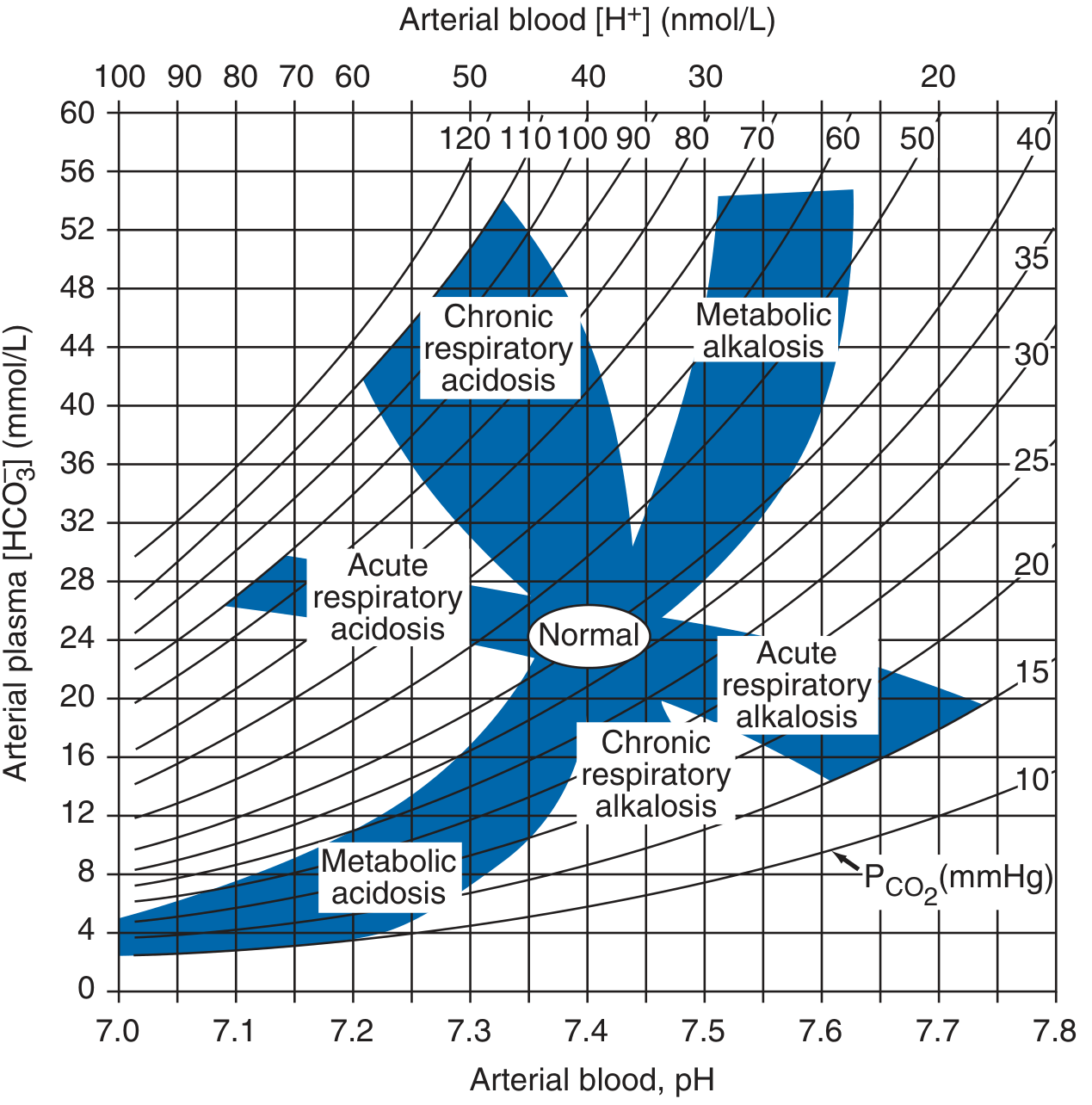
Acid-Base Nomogram
This chart plots pH against HCO3- with PCO2 lines. Any point inside the blue zones = simple disorder. Any point outside = mixed disorder.
The 4 Disorders in Detail
1. METABOLIC ACIDOSIS (Most important in ICU)
Definition: Low pH + Low HCO3-
First question: What is the Anion Gap?
AG = Na+ - (Cl- + HCO3-)
Normal AG = 8-12 mEq/L
Always correct AG for albumin if hypoalbuminemic:
For every 1 g/dL of albumin BELOW 4.5, add 2.5 to your calculated AG.
HIGH Anion Gap Metabolic Acidosis - Mnemonic: MUDPILES
| Letter | Cause |
|---|---|
| M | Methanol |
| U | Uremia (kidney failure) |
| D | DKA (diabetic ketoacidosis) |
| P | Paraldehyde / Paracetamol (acetaminophen) |
| I | Iron / Isoniazid |
| L | Lactic acidosis (sepsis, shock) |
| E | Ethylene glycol |
| S | Salicylates |
NORMAL Anion Gap Metabolic Acidosis - Mnemonic: HARDUP
| Letter | Cause |
|---|---|
| H | Hyperalimentation / Hospital saline (normal saline infusion) |
| A | Acid infusion / Addison's disease / Carbonic anhydrase inhibitors |
| R | Renal Tubular Acidosis (RTA) |
| D | Diarrhea |
| U | Ureterosigmoidostomy |
| P | Pancreatic fistula / drainage |
How to CORRECT Metabolic Acidosis:
Treat the underlying cause FIRST!
| Cause | Treatment |
|---|---|
| DKA | Insulin + fluids + electrolyte replacement |
| Lactic acidosis/Sepsis | Fluids, vasopressors, treat infection |
| Renal failure | Dialysis |
| Diarrhea | IV fluids (NS or LR) |
When to give Sodium Bicarbonate (NaHCO3)?
- pH < 7.10 in severe metabolic acidosis, OR
- pH < 7.20 in metabolic acidosis with acute kidney injury
- (Rosen's Emergency Medicine)
Note: Routine bicarbonate for lactic acidosis is controversial - treat the cause first.
2. METABOLIC ALKALOSIS
Definition: High pH + High HCO3-
Common causes in ICU:
- Vomiting (loss of HCl)
- NG suctioning
- Loop/thiazide diuretics (Cl- loss)
- Steroid excess (Cushing's, exogenous)
- Over-correction of acidosis with bicarbonate
How to CORRECT Metabolic Alkalosis:
Step 1: Check urine chloride to classify:
| Urine Cl- | Type | Treatment |
|---|---|---|
| < 20 mEq/L | Saline-responsive (vomiting, NG loss, old diuretics) | Give IV Normal Saline |
| > 20 mEq/L | Saline-resistant (Cushing's, Conn's, active diuretics) | Treat the underlying condition |
Saline-responsive alkalosis = give NS + KCl (correct potassium too!)
Saline-resistant = spironolactone, acetazolamide, or treat primary cause
3. RESPIRATORY ACIDOSIS
Definition: Low pH + High PaCO2
Causes - anything that reduces ventilation:
- COPD exacerbation
- Severe asthma
- Opioid/sedative overdose (respiratory depression)
- Neuromuscular disease (Guillain-Barre, myasthenia)
- Pneumothorax
- Post-op incomplete reversal of neuromuscular blockade
Acute vs Chronic:
- Acute: CO2 rises fast, kidneys haven't compensated yet → pH drops sharply
- Chronic: Kidneys compensate over days by retaining HCO3-
In perioperative/ICU medicine, slow shallow breathing = impaired respiratory drive; rapid shallow = chest/lung problem; obstructed = airway problem - Miller's Anesthesia, 10th Ed.
How to CORRECT Respiratory Acidosis:
| Situation | Action |
|---|---|
| Awake, mild | Oxygen, bronchodilators, treat cause |
| Worsening/severe | NIV (BiPAP) first line |
| Respiratory failure | Intubate + mechanical ventilation |
| Opioid OD | Naloxone |
| COPD (chronic) | Target CO2 to THEIR baseline, not normal 40 |
ICU tip: In chronic COPD, their "normal" CO2 may be 60-70 mmHg. Never over-oxygenate or over-ventilate them - aim for their baseline.
4. RESPIRATORY ALKALOSIS
Definition: High pH + Low PaCO2 (hyperventilation)
Common causes:
- Anxiety / pain
- Sepsis (early)
- Salicylate poisoning
- Pulmonary embolism
- Liver failure (hepatic encephalopathy)
- Iatrogenic over-ventilation on mechanical ventilator
- Pregnancy (normal in 3rd trimester)
How to CORRECT Respiratory Alkalosis:
| Cause | Treatment |
|---|---|
| Anxiety | Reassurance, rebreathing (paper bag), benzodiazepines |
| Pain | Analgesia |
| Sepsis | Treat infection |
| Mechanical ventilator | Reduce RR or tidal volume |
| Salicylate OD | NaHCO3 (alkalinize urine to trap salicylate) |
Mixed Acid-Base Disorders (Common in ICU)
When compensation is too much or too little, you have a mixed disorder - two problems at once. These are life-threatening. - Harrison's, 22nd Ed.
| Mixed Disorder | Example Clinical Setting |
|---|---|
| Met Acidosis + Resp Acidosis | Severe pneumonia + shock (worst combination, extreme acidemia) |
| Met Acidosis + Resp Alkalosis | Sepsis in ICU (lactic acidosis + hyperventilation) |
| Met Alkalosis + Resp Alkalosis | End-stage liver disease |
| Met Alkalosis + Resp Acidosis | COPD patient on diuretics |
| High-AG + Normal-AG acidosis | Diarrhea + lactic acidosis |
Rule of thumb to detect mixed disorder:
- If compensation is OUTSIDE the predicted range = mixed disorder
- If Paco2 and HCO3- move in OPPOSITE directions = always mixed
ICU Pearls & Memory Tricks
The ROME Mnemonic (Which is Primary)
R.O.M.E.
- Respiratory Opposite: CO2 up → pH down / CO2 down → pH up
- Metabolic Equal: HCO3- up → pH up / HCO3- down → pH down
The pH tells you which is DOMINANT
When pH < 7.35 → the acidosis dominates
When pH > 7.45 → the alkalosis dominates
Quick Trick: PaCO2 ≈ Last two digits of pH (in metabolic acidosis)
If HCO3- = 10, expected pH ≈ 7.23, expected PCO2 ≈ 23 mmHg - Roberts & Hedges
CO2 = Acid produced by lungs; HCO3- = Base managed by kidneys
- Lungs fix problems in minutes
- Kidneys fix problems in hours to days
Putting It All Together: 5-Question Approach
When you get an ABG in the ICU, ask these 5 questions in order:
1. Is pH normal, low, or high?
2. Does the CO2 explain it? (respiratory cause?)
3. Does the HCO3- explain it? (metabolic cause?)
4. Is there compensation? (use formulas above)
5. Calculate Anion Gap - is there a hidden metabolic acidosis?
Practice Example (ICU Sepsis Patient):
- pH: 7.28, PaCO2: 24 mmHg, HCO3-: 11 mEq/L, Na: 140, Cl: 105
Step 1: pH 7.28 → Acidosis
Step 2: CO2 24 (low) → not the cause; respiratory is compensating
Step 3: HCO3- 11 (low) → Metabolic Acidosis is primary
Step 4: Winter's: Expected CO2 = (1.5 × 11) + 8 = 24.5 → measured 24 ✓ appropriate compensation, simple disorder
Step 5: AG = 140 - (105 + 11) = 24 → HIGH AG metabolic acidosis → think MUDPILES → in this septic patient = Lactic acidosis
Management: IV fluids, vasopressors, blood cultures, antibiotics, lactate clearance
Summary Cheat Sheet
ACIDOSIS (pH < 7.35)
├── CO2 HIGH → Respiratory Acidosis → Fix the lungs (ventilate)
└── HCO3- LOW → Metabolic Acidosis → Fix the cause; bicarb if pH <7.10
ALKALOSIS (pH > 7.45)
├── CO2 LOW → Respiratory Alkalosis → Fix ventilation / treat cause
└── HCO3- HIGH → Metabolic Alkalosis → NS + KCl (if saline-responsive)
ALWAYS calculate Anion Gap in any metabolic acidosis
ALWAYS apply compensation formula - if wrong, it's MIXED
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Roberts & Hedges' Clinical Procedures in Emergency Medicine
- Rosen's Emergency Medicine, Concepts and Clinical Practice
- Miller's Anesthesia, 10th Ed.
- Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.