Anti tussive action of opioid (morphine)
Antitussive Action of Morphine (Opioids)
Mechanism of Action
- Lippincott Pharmacology: "Both morphine and codeine have antitussive properties and cause cough suppression by direct depression of the medullary cough reflex."
- Goodman & Gilman's: "Morphine, codeine, and related opioids depress the cough reflex at least in part by a direct effect on a cough center in the medulla."
Key Features
| Feature | Detail |
|---|---|
| Site of action | Medullary cough center (brainstem) |
| Receptor type | Opioid receptors - but different from those mediating analgesia |
| Dose | Achieved at doses below those needed for analgesia |
| Correlation with analgesia | No close correlation - antitussive and analgesic effects are dissociable |
| Correlation with respiratory depression | No obligatory relationship - cough can be suppressed without depressing respiration |
| Glottal function | Protective glottal function is preserved even during cough suppression |
Receptors Involved
- Stereoisomers of opioid molecules that have no analgesic activity or addiction liability (e.g., dextromethorphan) still produce antitussive effects.
- The antitussive dose is lower than the analgesic dose for codeine (15 mg antitussive vs. higher doses for analgesia).
Clinically Used Opioid Antitussives
| Drug | Notes |
|---|---|
| Codeine | Most commonly used opioid antitussive; 15 mg sufficient for cough suppression |
| Dextromethorphan | Synthetic morphine derivative; no analgesic/addictive properties at antitussive doses; blocks medullary cough center; also acts via NMDA receptor antagonism |
| Morphine | Has antitussive property but not preferred clinically for this indication due to addiction and side effect profile |
| Noscapine | Used outside the USA; devoid of opioid side effects |
| Levopropoxyphene | Stereoisomer of dextropropoxyphene; no opioid effects |
Dissociation from Respiratory Depression
Summary Points for Exams
- Morphine suppresses cough via direct depression of the medullary cough center.
- The antitussive receptors are distinct from analgesic receptors.
- Cough suppression occurs at sub-analgesic doses.
- There is no obligatory link between antitussive action and respiratory depression.
- Codeine is the prototypical opioid antitussive; dextromethorphan is the most widely used non-addictive alternative.
- The protective glottal reflex is preserved during opioid-induced cough suppression.
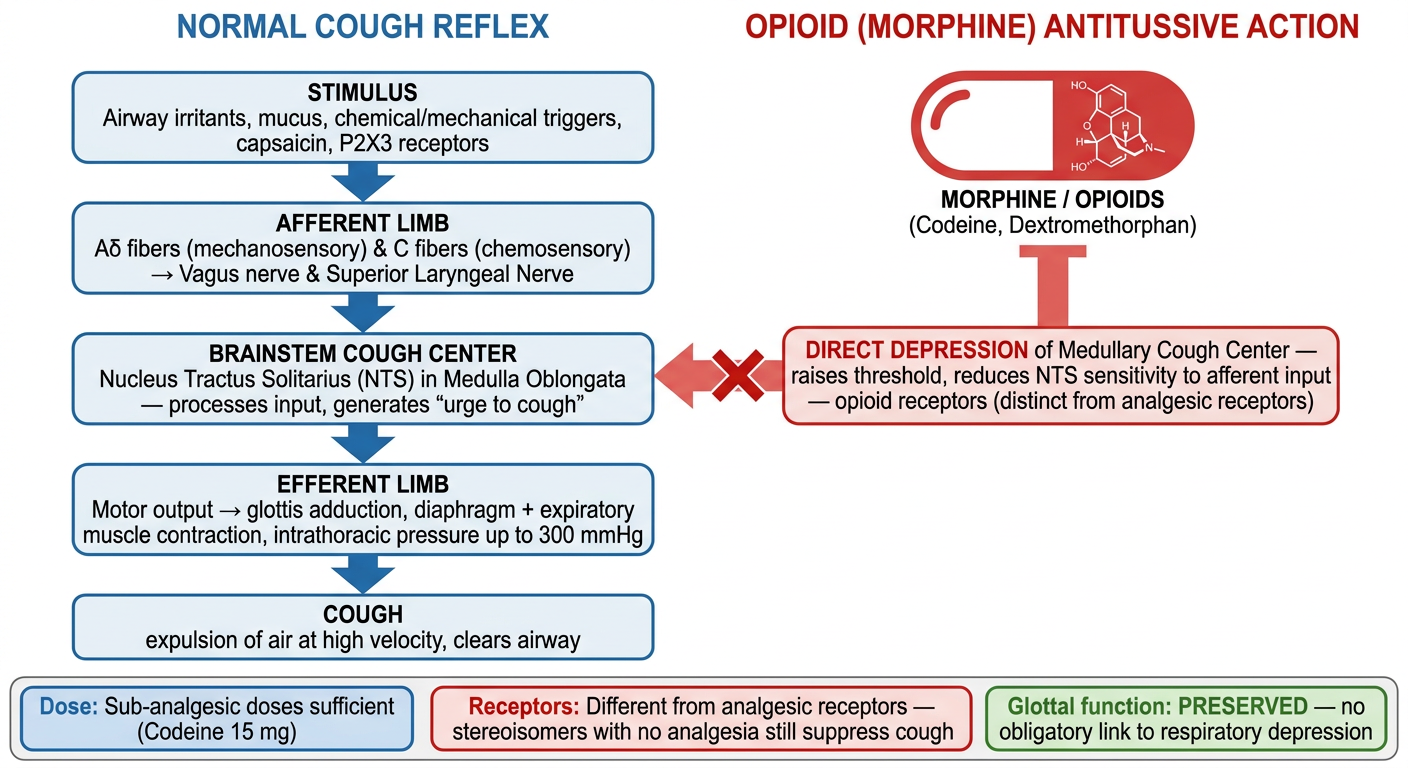
Anti tussive action of opioid (morphine) representation with reference and diagrammatic representation
A clean medical pharmacology diagram showing the antitussive action of morphine. The diagram has two parallel vertical flowcharts side by side titled "NORMAL COUGH REFLEX" and "OPIOID (MORPHINE) ANTITUSSIVE ACTION". LEFT SIDE - Normal Cough Reflex (blue arrows going downward): Box 1: "STIMULUS (Airway irritants, mucus, chemical/mechanical triggers, capsaicin, P2X3 receptors)" Arrow down Box 2: "AFFERENT LIMB: Aδ fibers (mechanosensory) & C fibers (chemosensory) → Vagus nerve & Superior Laryngeal Nerve" Arrow down Box 3: "BRAINSTEM COUGH CENTER: Nucleus Tractus Solitarius (NTS) in Medulla Oblongata — processes input, generates 'urge to cough'" Arrow down Box 4: "EFFERENT LIMB: Motor output → glottis adduction, diaphragm + expiratory muscle contraction, intrathoracic pressure up to 300 mmHg" Arrow down Box 5: "COUGH (expulsion of air at high velocity, clears airway)" RIGHT SIDE - Morphine Antitussive Action (red inhibitory arrows): Large red pill/molecule icon labeled "MORPHINE / OPIOIDS (Codeine, Dextromethorphan)" Big red inhibitory flat arrow pointing at the Brainstem Cough Center box Text in red box: "DIRECT DEPRESSION of Medullary Cough Center — raises threshold, reduces NTS sensitivity to afferent input — opioid receptors (distinct from analgesic receptors)" Below both sides, a shared footer panel with three key facts in colored boxes: - "Dose: Sub-analgesic doses sufficient (Codeine 15 mg)" - "Receptors: Different from analgesic receptors — stereoisomers with no analgesia still suppress cough" - "Glottal function: PRESERVED — no obligatory link to respiratory depression" Clean white background, medical illustration style, professional and clear labels.
Antitussive Action of Morphine - Full Reference Notes
The Normal Cough Reflex (What Morphine Suppresses)
| Step | Component | Detail |
|---|---|---|
| 1 | Stimulus | Chemical (capsaicin, irritants) or mechanical (mucus, particles) triggers |
| 2 | Sensory receptors | Transient receptor potential (TRP) channels and P2X3 ion channels on afferent nerve endings |
| 3 | Afferent fibers | Aδ fibers (mechanosensory) and C fibers (chemosensory); innervate pharynx, larynx, airways down to terminal bronchioles |
| 4 | Afferent pathway | Signals travel via vagus nerve and superior laryngeal nerve |
| 5 | Brainstem integration | Nucleus Tractus Solitarius (NTS) in the medulla processes input → generates "urge to cough" |
| 6 | Efferent output | Glottis adducts → expiratory muscles contract → intrathoracic pressure up to 300 mmHg → rapid expiratory airflow clears airway |
How Morphine Suppresses Cough
"Morphine, codeine, and related opioids depress the cough reflex at least in part by a direct effect on a cough center in the medulla; this cough suppression can be achieved without altering the protective glottal function."
"Both morphine and codeine have antitussive properties and cause cough suppression by direct depression of the medullary cough reflex. In general, cough suppression does not correlate closely with analgesic and respiratory depressant properties of opioid drugs. The receptors involved in the antitussive action appear to be different from those involved in analgesia."
Key Pharmacological Dissociations
ANALGESIC ACTION ≠ ANTITUSSIVE ACTION
μ-opioid receptors Different opioid receptors
Higher doses needed Sub-analgesic doses sufficient
Addiction liability Stereoisomers without addiction work
RESPIRATORY DEPRESSION ≠ ANTITUSSIVE ACTION
Obligatory with high doses NO obligatory link
Dextromethorphan: antitussive but NO respiratory depression
Clinically Used Opioid Antitussives
| Drug | Type | Antitussive Dose | Notes |
|---|---|---|---|
| Codeine | Natural opioid | 15 mg | Prototype; also analgesic at higher doses |
| Dextromethorphan | Synthetic morphine stereoisomer | 15-30 mg q6-8h | No analgesia, no addiction; also NMDA antagonist; most widely used OTC |
| Noscapine | Opium alkaloid | - | No opioid effects; used outside USA |
| Levopropoxyphene | Stereoisomer | 50-100 mg q4h | Devoid of opioid effects |
"The opioid analgesics are among the most effective drugs available for the suppression of cough. This effect is often achieved at doses below those necessary to produce analgesia... The antitussive effect is also produced by stereoisomers of opioid molecules that are devoid of analgesic effects and addiction liability."
Summary - Exam High-Yield Points
- Site: Direct depression of medullary cough center (NTS region)
- Dose: Below analgesic dose (codeine 15 mg antitussive vs. higher for pain)
- Receptors: Distinct from analgesic receptors - proven by stereoisomers
- Glottal reflex: Preserved (protective function maintained)
- No obligatory link to respiratory depression
- Best clinical choice: Codeine (opioid) or dextromethorphan (non-addictive)
- Caution: Avoid in asthma (morphine releases histamine causing bronchoconstriction)
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 472 - Cough section
- Lippincott Illustrated Reviews: Pharmacology, p. 711 - Depression of cough reflex
- Katzung's Basic and Clinical Pharmacology, 16e, p. 896 - Antitussives section
- Harrison's Principles of Internal Medicine, 22e, p. 2216 - Cough mechanism