Syphilis
Reading File
Finding Sources
Searching PubMed
syphilis diagnosis treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to provide a thorough answer. Let me compile it.
Syphilis
Overview
Syphilis is a systemic sexually transmitted infection caused by the spirochete Treponema pallidum subspecies pallidum. It is sometimes called the "Great Masquerader" or "Great Imitator" due to its protean manifestations across multiple organ systems. It remains a major public health problem, with an estimated 6 million new cases annually worldwide. - Sherris & Ryan's Medical Microbiology, 8e
Microbiology
T. pallidum is a delicate, motile spiral spirochete, 5-20 µm long, with 4-14 spirals. Its characteristic motility consists of three movements: forward propulsion along the long axis, rotation on its long axis, and side-to-side bending. It cannot be cultured in vitro.
Key virulence features:
-
Very few surface antigens - outer membrane contains only ~1% as many antigens as E. coli, helping the organism evade immune detection
-
Rapid dissemination - enters the bloodstream within hours of inoculation; reaches the brain within 18 hours
-
Antigen variation - outer membrane proteins mutate rapidly, generating subpopulations with different surface antigens
-
Low metabolic capacity - its genome is only one quarter the size of most bacteria; sensitive to temperature changes
-
Andrews' Diseases of the Skin, p. 4724-4728
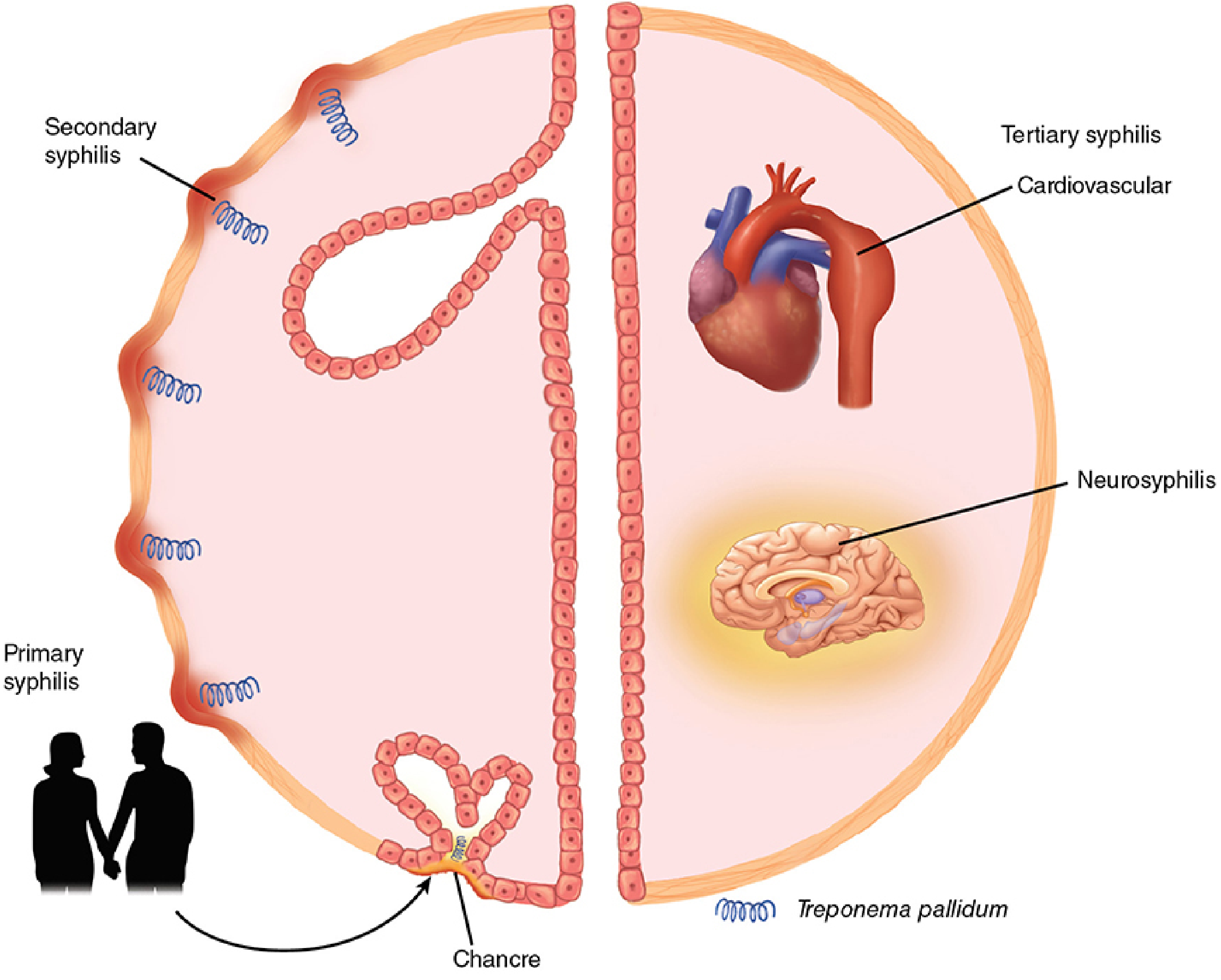
Clinical Stages
Primary Syphilis
-
Occurs after an incubation period of 10-90 days (average 3 weeks) following sexual exposure
-
Classic lesion: the chancre - a solitary (can be multiple in 32-47% of cases), painless, indurated round-to-oval ulcer with sharply demarcated, raised, regular borders and a clean base; feels cartilaginous ("hard ulcer" / ulcus durum)
-
Location: usually genital mucosa, but can be oral, anorectal, or any site of inoculation
-
Accompanied by painless regional lymphadenopathy
-
The chancre heals spontaneously in 3-6 weeks even without treatment - but the spirochetes have already disseminated
-
Darkfield examination or direct fluorescent antibody testing of the chancre is diagnostic; serology can be negative in up to 30% of primary cases
-
Fitzpatrick's Dermatology, Vol. 1-2, p. 3177-3179

Secondary Syphilis
-
Develops in 60-90% of persons with untreated primary syphilis, typically 3-12 weeks after the chancre
-
Results from hematogenous dissemination of treponemes throughout the body
-
Rash is present in nearly all cases:
- Erythematous macules or maculopapules symmetrically on trunk and extremities (40-70%)
- Classically involves palms and soles (hyperpigmented, scaly papules)
- Biett collarette - white scaly ring on papulosquamous lesions; characteristic of syphilis
- Usually NOT pruritic
- Face is typically spared, but seborrheic dermatitis-like lesions at the hairline (Corona of Venus) can occur
-
Condylomata lata - moist, flat, warty lesions in anogenital or skin fold areas; highly infectious
-
Mucous patches - shallow, painless ulcerations of the oral or genital mucosa
-
Alopecia - patchy "moth-eaten" pattern on the scalp
-
Systemic symptoms: fever, generalized lymphadenopathy, headache, sore throat, arthralgias, malaise
-
Organ involvement (less common): CNS, eyes, liver, kidneys (immune-complex glomerulonephritis)
-
Secondary syphilis is the stage with the highest serologic sensitivity: RPR is ~99% sensitive, MHA-TP ~100% sensitive
-
Fitzpatrick's Dermatology, p. 3180-3186; Textbook of Family Medicine 9e, p. 2592

Latent Syphilis
- Defined by reactive serologic tests in the absence of any clinical signs or symptoms
- Early latent: acquired within the preceding 12 months; up to 25% may relapse into secondary syphilis
- Late latent: acquired more than 12 months ago; much lower risk of relapse
- Treatment differs between early and late latent stages
Tertiary (Late) Syphilis
Develops years to decades after initial infection in ~25-40% of untreated patients. Three major forms:
| Form | Manifestations |
|---|---|
| Gummatous | Granulomatous nodular lesions in skin, bone, liver, or other organs; "gumma" = necrotizing granuloma |
| Cardiovascular | Aortic aneurysm (ascending aorta), aortic regurgitation, coronary ostial stenosis; from endarteritis of the vasa vasorum |
| Neurosyphilis | General paresis, tabes dorsalis, meningovascular syphilis, CNS gumma; Argyll Robertson pupil (accommodates but does not react to light) |
- Neurosyphilis and ocular syphilis can occur at any stage of infection, not only tertiary
- Textbook of Family Medicine 9e, p. 2592-2594
Congenital Syphilis
-
Transmission rates from untreated mothers: 70-100% in primary syphilis, 40% in early latent, 10% in late latent
-
Fetal infection can occur at any stage of pregnancy; leads to stillbirth in 30-40% of cases
-
Early congenital syphilis (<2 years): fever, rash, hepatosplenomegaly, "snuffles" (persistent rhinitis), osteochondritis causing pseudoparalysis of Parrot
-
Late congenital syphilis: Hutchinson teeth (notched incisors), interstitial keratitis, VIII nerve deafness (Hutchinson triad), saddle-nose deformity, saber shins
-
Routine serologic screening in early pregnancy is standard; should be repeated in the last trimester for high-risk women
-
Fitzpatrick's Dermatology, p. 3187; Sherris & Ryan's, p. 1416
Diagnosis
Direct Detection
- Darkfield microscopy: gold standard for primary chancre and moist secondary lesions; identifies characteristic corkscrew morphology and motility. NOT valid for oral or anal lesions (commensal treponemes present)
- Direct fluorescent antibody (DFA): confirms T. pallidum in lesion exudate; more specific than darkfield
- PCR: available in specialized centers; high sensitivity/specificity
Serologic Tests
Nontreponemal tests (RPR, VDRL):
- Detect antibodies to cardiolipin-lecithin-cholesterol antigen (reagin)
- Used for screening and monitoring treatment response
- Titers correlate with disease activity; a fourfold fall after treatment = adequate response
- RPR sensitivity: ~79% in primary, 99% in secondary, 87% in latent, 73% in tertiary syphilis
- False positives occur with pregnancy, autoimmune disease, viral infections (EBV, HIV, hepatitis), Lyme disease, and narcotic addiction
Treponemal tests (FTA-ABS, TPHA, MHA-TP, TP-EIA):
- Detect antibodies against T. pallidum antigens
- Higher sensitivity in primary and late stages; higher specificity overall
- Remain positive for life even after successful treatment in most people (15-25% become nonreactive 2-3 years after treatment of primary syphilis)
- Used to confirm a reactive nontreponemal test
- NOT used to monitor treatment response (titers do not correlate with activity)
Traditional algorithm: Nontreponemal test first → confirm with treponemal test if positive
Reverse algorithm: Treponemal EIA first → RPR for staging if positive
- Fitzpatrick's Dermatology, p. 3190-3195
CSF Examination (Lumbar Puncture) - Indications
- Neurologic, ophthalmic, or otologic signs or symptoms
- Evidence of active tertiary syphilis
- Treatment failure
Treatment
Treatment is stage-dependent. Penicillin G is the drug of choice for all stages.
| Stage | Treatment |
|---|---|
| Primary, secondary, early latent (<1 year) | Benzathine penicillin G 2.4 million units IM x 1 dose |
| Late latent (>1 year) or unknown duration | Benzathine penicillin G 2.4 million units IM weekly x 3 doses |
| Tertiary (non-neurologic) | Benzathine penicillin G 2.4 million units IM weekly x 3 doses |
| Neurosyphilis / ocular syphilis | Aqueous crystalline penicillin G 18-24 million units/day IV x 10-14 days |
| Congenital syphilis | Aqueous penicillin G IV or procaine penicillin G IM x 10 days |
| Penicillin allergy (non-pregnant) | Doxycycline 100 mg twice daily x 14 days (early) or 28 days (late) |
| Penicillin allergy in pregnancy | Desensitize and treat with penicillin; no acceptable substitute in pregnancy |
-
Jarisch-Herxheimer reaction: fever, headache, myalgias occurring 2-8 hours after the first dose of treatment; results from cytokine release due to rapid spirochete killing. Manage with antipyretics; do NOT discontinue treatment.
-
Treatment response is monitored by fourfold fall in nontreponemal titer (e.g., 1:32 to 1:8) within 6-12 months of therapy. Failure to achieve this is considered treatment failure.
-
Textbook of Family Medicine 9e, p. 2598; Fitzpatrick's Dermatology, p. 3197-3200
Key Points Summary
| Feature | Detail |
|---|---|
| Causative organism | Treponema pallidum subsp. pallidum |
| Transmission | Sexual contact; transplacental (congenital) |
| Primary lesion | Painless indurated chancre + painless lymphadenopathy |
| Secondary hallmark | Palm/sole rash, condylomata lata, mucous patches |
| Most infectious stage | Secondary syphilis |
| Best serologic stage | Secondary (RPR 99%, MHA-TP 100%) |
| Tertiary complications | Gumma, aortitis/aortic regurgitation, neurosyphilis |
| Treatment of choice | Penicillin G (preparation and dose varies by stage) |
| Test to monitor treatment | Nontreponemal titer (RPR/VDRL) - expect fourfold fall |
Recent evidence note: A 2024 systematic review and meta-analysis on neurosyphilis treatment alternatives [PMID: 38661311] and a 2024 AEDV expert consensus guideline for syphilis management [PMID: 39111574] are available. A 2026 systematic review examining the immunopathology of serofast syphilis (persistent positive serology despite treatment) [PMID: 41983122] adds nuance to monitoring, particularly for patients whose RPR titers do not fall as expected.
This is a shared conversation. Sign in to Orris to start your own chat.