Tech me psm all national health programmes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive information from Park's textbook. Let me compile the full, well-structured response.
National Health Programmes of India (PSM)
Source: Park's Textbook of Preventive and Social Medicine
Overview
India runs a series of National Health Programmes (NHPs) to address the major disease burdens - both communicable and non-communicable. They are funded centrally (100% or partially) and implemented through the public health infrastructure (Sub-centres, PHCs, CHCs, District Hospitals).
A. COMMUNICABLE DISEASE PROGRAMMES
1. National TB Elimination Programme (NTEP)
Previously: Revised National TB Control Programme (RNTCP)
- Launched: National TB Programme (NTP) 1962; RNTCP revitalized 1993; renamed NTEP 2020
- Goal: Eliminate TB by 2025 (ahead of global target of 2030)
- Strategy: DOTS (Directly Observed Treatment Short-course)
5 components of DOTS:
- Political will and administrative commitment
- Diagnosis by quality-assured sputum smear microscopy
- Adequate supply of quality-assured short-course chemotherapy
- Directly Observed Treatment (DOT)
- Systematic monitoring and accountability
Objectives of RNTCP:
- At least 85% cure rate of infectious TB cases
- Detection of at least 70% of estimated cases by quality sputum microscopy
STOP TB Strategy (2006, adopted by RNTCP):
- Pursuing quality DOTS expansion
- Addressing TB/HIV and MDR-TB
- Contributing to health system strengthening
- Engaging all care providers
- Empowering patients and communities
- Enabling and promoting research
National Strategic Plan (NSP) 2017-2025 targets:
- Reduce TB incidence to 44/1,00,000
- Reduce TB mortality to 3/1,00,000
- Zero catastrophic expenditure for TB patients
2. National AIDS Control Programme (NACP)
- Launched: 1987
- Implementing body: NACO (National AIDS Control Organization) - a separate wing under MoHFW
Aim: Prevent HIV transmission, decrease morbidity/mortality, minimize socio-economic impact
Key Milestones:
| Year | Milestone |
|---|---|
| 1986 | First HIV case detected; AIDS Task Force by ICMR |
| 1992 | NACP-I launched; NACO set up |
| 1999 | NACP-II; State AIDS Control Societies established |
| 2002 | National AIDS Control Policy adopted |
| 2004 | ART initiated |
| 2006 | National Council on AIDS under PM |
| 2007 | NACP-III launched |
| 2014 | NACP-IV launched |
| 2017 | National Strategic Plan for HIV/AIDS and STIs 2017-2024 |
PHC-level activities:
- IEC for STIs/HIV prevention
- PPTCT (Prevention of Parent to Child Transmission) services
- Condom promotion and distribution to high-risk groups
- Linkage with VCTC at district level
- Pre and post-test counselling
3. National Leprosy Eradication Programme (NLEP)
PHC-level essentials:
- Health education to community regarding leprosy
- Diagnosis and management of leprosy, reactions, and complications
- Training of patients with ulcers for self-care
- Counselling for regularity/completion of MDT (Multi-Drug Therapy)
4. National Programme for Control of Blindness (NPCB)
- Launched: 1976 (100% centrally sponsored; incorporated trachoma control programme of 1968)
- Goal: Reduce blindness prevalence from 1.4% to 0.3%
- Current prevalence: 0.36% (2015-19 survey)
3 signature activities (12th Five Year Plan):
- 66 lakh cataract operations per year
- School eye screening + 9 lakh free spectacles/year for refractive errors
- 50,000 donated eyes/year for keratoplasty
Key strategies:
- Free cataract surgery through NGO + private practitioners
- Screening of population above 50 years
- Refractive error correction in school children
- Regional Institutes of Ophthalmology as Centres of Excellence
- Public-private partnership for underserved areas
5. National Vector-Borne Disease Control Programme (NVBDCP)
Covers the following diseases:
- Malaria - previously National Malaria Eradication Programme (NMEP, 1958), modified to National Malaria Control Programme
- Filaria - National Filaria Control Programme
- Dengue, Chikungunya, JE (Japanese Encephalitis), Kala-azar
PHC activities:
- Symptomatic treatment for suspected JE and dengue
- Complete treatment for Kala-azar cases (as per national policy)
- Treatment of microfilaria-positive cases with DEC + Albendazole
- Mass Drug Administration (MDA) for lymphatic filariasis
- Morbidity management of lymphoedema cases
6. National Programme for Prevention and Control of Deafness (NPPCD)
Essential activities:
- Early detection of hearing impairment and referral
- Basic treatment of common ear diseases (wax, otomycosis, otitis externa, otitis media)
- IEC for prevention and early detection of hearing impairment
B. NON-COMMUNICABLE DISEASE PROGRAMMES
7. National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS)
- Background: NCDs accounted for 60% of deaths in India (2016). National Programme for Diabetes, CVD, and Stroke was later integrated with National Cancer Control Programme.
- Coverage: 11th Plan - 100 districts in 21 states; 12th Plan - all districts of India
Major objectives:
- Prevent and control NCDs through behaviour and lifestyle changes
- Provide early diagnosis and management
- Build capacity at all healthcare levels
- Train health manpower (doctors, paramedics, nurses)
- Establish palliative and rehabilitative care
Key strategies:
- Opportunistic screening of persons above 30 years of age
- NCD Clinics at CHC and district level
- Mass media and IEC for behavioural change
- Implementation through 20,000 sub-centres and 700 CHCs
Cancer-specific activities at PHC level:
- IEC for cancer prevention and warning signs
- Early detection of cancer (warning signals: change in bladder/bowel habits, etc.)
- Referral for confirmation and treatment
8. National Mental Health Programme (NMHP)
- Launched: 1982
- Coverage: 517 districts in 36 states
- Purpose: Ensure mental health care for all, especially underprivileged; integrate mental health into general health care
Aims (3):
- Prevention and treatment of mental/neurological disorders and disabilities
- Use of mental health technology to improve general health services
- Application of mental health principles in national development
Objectives (3):
- Ensure minimum mental health care for vulnerable/underprivileged populations
- Encourage application of mental health knowledge in general health care and social development
- Promote community participation in mental health services
Programme Strategies:
- Integration with primary health care through NMHP
- Provision of tertiary care institutions
- Eradicating stigmatization; protecting rights via Central/State Mental Health Authorities
District Mental Health Programme (DMHP) components:
- Training at nodal institutes
- Public education - awareness and stigma reduction
- OPD and indoor services for early detection and treatment
- Data collection for planning, research, and improvement
DMHP promotive activities:
- School mental health services (life skills education, counselling)
- College counselling services
- Workplace stress management
- Suicide prevention services (helplines, counselling centres)
C. MATERNAL, CHILD HEALTH AND FAMILY WELFARE
9. National Family Welfare Programme
- Launched: 1952 - India was the FIRST country in the world to launch a national family planning programme
- Evolved through successive five-year plans
- 1966: Separate Department of Family Planning created
- 1977: Renamed "Family Welfare" (voluntary basis; no coercion)
- 1985-86: Universal Immunization Programme (UIP) started
- 1992: Child Survival and Safe Motherhood (CSSM) Programme
- 1994 (Cairo ICPD): Integrated as Reproductive and Child Health (RCH) Programme
- Currently under National Health Mission (NHM)
Key demographic targets (National Health Policy 1983):
- NRR = 1 by year 2000
- Birth rate of 21 per 1000
- Death rate of 9 per 1000
- Couple protection rate of 60%
D. ELDERLY AND SPECIAL POPULATION
10. National Programme for Health Care of the Elderly (NPHCE)
- Launched: 11th Five Year Plan, initially in 100 districts of 21 states
- Aim: Provide separate, specialized, comprehensive healthcare to senior citizens at all levels of the health care delivery system
Infrastructure developed:
- 8 regional geriatric centres as referral units
- Geriatric Departments at 20 super-specialized institutions (30-bed inpatient facility)
- Geriatric units at district hospitals (10-bed ward + dedicated OPD)
- Rehabilitation units at CHCs (dedicated elderly health clinics twice a week)
- 2 National Centres of Ageing (NCA) at AIIMS New Delhi and Madras Medical College, Chennai
Strategies:
- Preventive and promotive care
- Management of illness
- Health manpower development for geriatric services
- Medical rehabilitation and therapeutic intervention
- IEC activities
E. ENVIRONMENTAL HEALTH PROGRAMMES
11. National Water Supply and Sanitation Programme
- Initiated: 1954
- Renamed: Rajiv Gandhi National Drinking Water Mission (1991) → Swajaldhara (2002) → National Rural Drinking Water Programme (NRDWP) from April 2009 (now a component of Bharat Nirman)
Norms:
- 40 litres of safe water per capita per day
- At least 1 hand pump/spot source per 250 persons
"Problem village" definition: No safe water within 1.6 km OR depth > 15 metres OR excess salinity/fluorides/iron OR risk of cholera
Swajaldhara was a community-led, participatory programme with panchayat-level ownership for planning, operation, and maintenance of water schemes.
F. OTHER NATIONAL PROGRAMMES (at PHC level)
| Programme | Key Focus |
|---|---|
| National STD Control Programme | STI diagnosis, treatment, contact tracing |
| National Iodine Deficiency Disorders Control Programme | Iodized salt distribution, goitre prevalence reduction |
| National Tobacco Control Programme (NTCP) | Anti-tobacco IEC, NRT, enforcement of COTPA |
| National Programme for Health Care of Elderly (NPHCE) | Geriatric care at all levels |
Quick Exam Summary Table
| Programme | Year Launched | Key Feature |
|---|---|---|
| National Family Welfare Programme | 1952 | India = FIRST country with national FP programme |
| National Malaria Eradication Programme | 1958 | Later modified to control |
| National Tuberculosis Programme | 1962 | RNTCP (DOTS) in 1993; NTEP in 2020 |
| Trachoma Control Programme | 1968 | Merged into NPCB |
| National Programme for Control of Blindness | 1976 | Goal: reduce blindness <0.3% |
| National AIDS Control Programme | 1987 | NACO as implementing body |
| National Mental Health Programme | 1982 | DMHP in all districts |
| Universal Immunization Programme | 1985-86 | Pulse Polio added 1995 |
| NPCDCS | 11th Plan | NCD screening >30 yrs; NCD clinics |
| NPHCE | 11th Plan | Geriatric care; NCA at AIIMS & MMC Chennai |
All content sourced from Park's Textbook of Preventive and Social Medicine (ISBN: 9789382219163)
NTEP in detail with mnemonics
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have all the data needed. Now let me compile the complete, detailed NTEP notes with mnemonics.
NTEP (National TB Elimination Programme) - Complete Notes
Source: Park's Textbook of Preventive and Social Medicine
1. HISTORY & EVOLUTION
| Year | Programme | Key Event |
|---|---|---|
| 1962 | NTP (National TB Programme) | India's first; treatment success low, default rates high |
| 1993 | RNTCP (Revised NTP) | Adopted DOTS; international assistance |
| 2006 | STOP TB Strategy | WHO; adopted by RNTCP |
| 2015 | End TB Strategy | WHO global framework |
| 2020 | NTEP | Renamed from RNTCP; elimination target by 2025 |
Mnemonic: "Never Repeat, Stop Ending" = NTP (1962) → RNTCP (1993) → STOP TB (2006) → END TB (2015) → NTEP (2020)
2. MAGNITUDE OF THE PROBLEM
Global:
- ~10 million new TB cases/year (2019)
- 1.2 million TB deaths among HIV-negative + 208,000 among HIV-positive
- 1/3 of world population infected asymptomatically; 5-10% develop clinical disease
- One infectious PTB patient can infect 10-15 persons per year
- MDR/RR-TB: 3.3% of new cases, 18% of retreatment cases
India:
- India has the highest TB burden globally
- Primary MDR-TB: ~2.8%
- Drug resistance in re-treatment cases: 12% (10-13%)
3. PROBLEM STATEMENT - MNEMONIC
"5-10% of Infected will get Disease; 10-15 contacts per case"
- 5-10% of asymptomatically infected persons develop clinical TB in their lifetime
- One case infects 10-15 contacts per year
4. CASE DEFINITIONS (2013 WHO, adopted by NTEP)
A. By Bacteriology:
| Type | Definition |
|---|---|
| Bacteriologically confirmed | Smear microscopy / culture / WRD (Xpert MTB/RIF) positive |
| Clinically diagnosed | No lab confirmation; diagnosed by clinician; given full TB treatment |
| Presumptive TB | Symptoms/signs suggestive of TB (previously called "TB suspect") |
B. By Anatomical Site:
- PTB (Pulmonary TB): Lung parenchyma or tracheobronchial tree; miliary TB = PTB
- EPTB (Extrapulmonary TB): Pleura, lymph nodes, abdomen, GUT, skin, joints/bones, meninges
- Patient with both PTB + EPTB → classified as PTB
C. By Treatment History:
| Category | Meaning |
|---|---|
| New | Never treated or <1 month of ATT |
| Relapse | Previously treated, declared cured/treatment complete, now smear/culture positive |
| Treatment after failure | Previously treated; smear/culture positive at month 5 or later |
| Treatment after loss to follow-up | Interrupted for ≥2 consecutive months, now smear/culture positive |
| Other previously treated | Does not fit above |
D. By Drug Resistance:
- DS-TB: Drug sensitive
- MDR-TB: Resistant to at least INH + Rifampicin
- RR-TB: Rifampicin resistant (by any method)
- XDR-TB: MDR-TB + resistant to any fluoroquinolone + any second-line injectable
Mnemonic for DR types: "My Rifle eXpired"
- MDR = INH + Rifampicin
- RR = Rifampicin alone
- eXDR = MDR + FQ + injectable
5. DOTS STRATEGY
Classic DOTS (5 Components)
Mnemonic: "PDASS" = Political Diagnosis Adequate DOT Systematic
- Political will and administrative commitment
- Diagnosis by quality-assured sputum smear microscopy
- Adequate supply of quality-assured short-course chemotherapy drugs
- Directly Observed Treatment (DOT)
- Systematic monitoring and accountability
STOP TB Strategy (2006) - 6 Components
Mnemonic: "PAC-EEE" - Pursue, Address, Contribute, Engage, Empower, Enable
- Pursuing quality DOTS expansion and enhancement
- Addressing TB/HIV and MDR-TB
- Contributing to health system strengthening
- Engaging all care providers
- Empowering patients and communities
- Enabling and promoting research
End TB Strategy (2015) - 3 Pillars
Mnemonic: "I-B-I" = Integrated, Bold, Intensified
- Integrated, patient-centred care and prevention
- Bold policies and supportive systems
- Intensified research and innovation
6. END TB TARGETS
| Milestone | 2020 | 2025 | SDG 2030 | End TB 2035 |
|---|---|---|---|---|
| Reduction in TB deaths vs 2015 | 35% | 75% | 90% | 95% |
| Reduction in TB incidence vs 2015 | 20% (<85/lakh) | 50% (<55/lakh) | 80% (<20/lakh) | 90% (<10/lakh) |
| Catastrophic cost for TB families | 0% | 0% | 0% | 0% |
India's NTEP target: Eliminate TB by 2025 (5 years ahead of global target of 2030)
7. CASE FINDING
Types:
- Passive Case Finding: Patient presents on own initiative with symptoms (>60% seek care on their own)
- Intensified/Active Case Finding (ICF): Provider-initiated, targets vulnerable/high-risk groups
Screening Strategies:
- Community screening: mobile/fixed facility, door-to-door
- Institutional screening: hospitals, congregate settings (prisons, refugee camps, old-age homes, workplaces)
Diagnostic Algorithm for Pulmonary TB (NTEP):
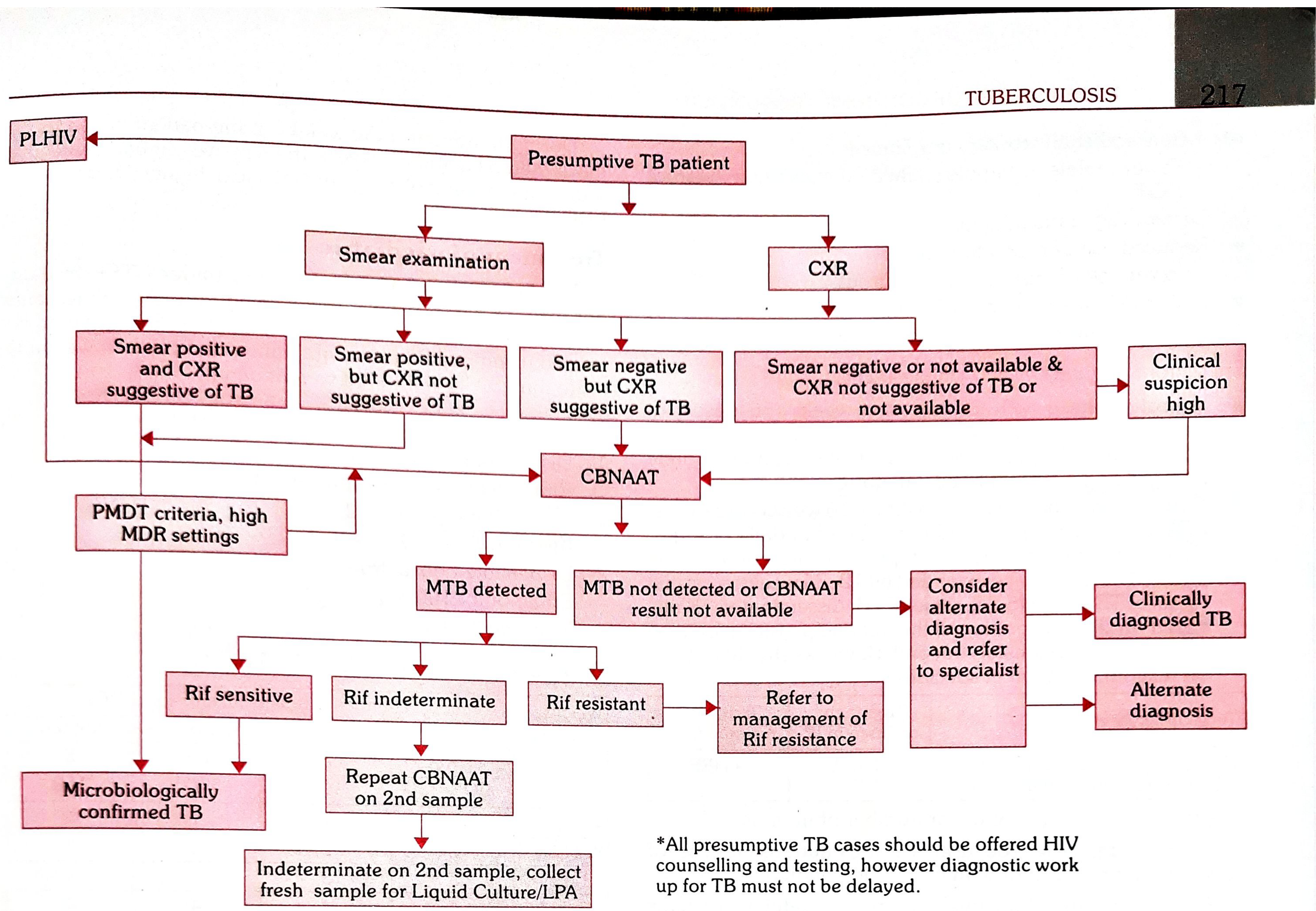
Key steps:
- All presumptive TB → Sputum smear (ZN/LEDFM) + CXR
- Smear positive + CXR suggestive → Microbiologically confirmed TB
- Smear negative + CXR suggestive → CBNAAT
- MTB detected + Rif sensitive → Microbiologically confirmed DS-TB
- MTB detected + Rif resistant → Manage as Rif-resistant TB
- MTB not detected → Consider alternate diagnosis; if clinical suspicion high → Clinically diagnosed TB
- All PLHIV (People Living with HIV) → Fast-track to CBNAAT
Mnemonic: "Smear-X-CBNAAT" = Always start with smear + CXR; escalate to CBNAAT when needed
8. ANTI-TUBERCULOSIS DRUGS
First-Line Drugs
Mnemonic: "RHZE + S" (Remember How Zebras Eat Straw)
| Drug | Abbreviation | Action |
|---|---|---|
| Rifampicin | R / RMP | Bactericidal (kills persisters too!) |
| H - Isoniazid (INH) | H / INH | Bactericidal (most powerful vs rapid multipliers) |
| Z - Pyrazinamide | Z | Bactericidal |
| E - Ethambutol | E | Bacteriostatic |
| S - Streptomycin | S | Bactericidal (injectable) |
Key Drug Points (high-yield):
- Rifampicin: Only drug active against "persisters"/dormant bacilli in caseous lesions; turns urine red (compliance test); never restart within 3 weeks if stopped (hypersensitivity risk)
- INH: Most distributed drug; crosses BBB and placenta; single daily dose preferred; peak level at 1-2 hours
- Pyrazinamide: Active in acidic pH (intracellular environment); used only in intensive phase
- Ethambutol: Bacteriostatic; causes optic neuritis (check visual acuity before starting)
- Streptomycin: Injectable; ototoxicity + nephrotoxicity; NOT in pregnancy (VIII nerve damage in fetus)
9. TREATMENT REGIMENS (NTEP - Daily Dose, 2019)
Fixed Dose Combinations (FDCs) in NTEP:
| Phase | Adults | Drugs |
|---|---|---|
| Intensive Phase (IP) | 4-FDC | H + R + Z + E |
| Continuation Phase (CP) | 3-FDC | H + R + E |
Mnemonic for IP: "HAZE" = H + R + Z + E (four drugs Haze the bug) Mnemonic for CP: "HRE" = Stay calm and "HERE" without Z
Standard Regimens:
| Category | Regimen | Duration |
|---|---|---|
| New DS-TB | 2HRZE / 4HRE | 6 months total |
| MDR-TB | Longer regimen (18-24 months) | Group A + B + C drugs |
- Daily dose regimen replaced the old thrice-weekly intermittent regimen in NTEP
- Drugs given in patient-wise boxes with complete course
10. TREATMENT OUTCOMES (Definitions)
Mnemonic: "CDFLT" = Cured, Done, Failed, Lost, Transferred"
| Outcome | Definition |
|---|---|
| Cured | Bacteriologically confirmed + smear/culture negative at end of treatment |
| Treatment completed | Treatment completed without evidence of failure; no negative smear at end |
| Treatment failed | Smear/culture positive at Month 5 or later |
| Lost to follow-up (LTFU) | Treatment interrupted for ≥2 consecutive months |
| Died | Died for any reason during treatment |
| Not evaluated | No treatment outcome assigned |
| Treatment success | Cured + Treatment completed |
RNTCP targets:
- Treatment success rate: ≥85% for smear-positive cases
- Case detection rate: ≥70% of estimated cases
11. MDR-TB MANAGEMENT
Causes of MDR-TB ("Man-made phenomenon"):
| Provider/Programme | Drugs | Patient |
|---|---|---|
| No guidelines / wrong guidelines | Drug stock-outs | Poor adherence / Poor DOT |
| Non-compliance with guidelines | Poor quality drugs | Lack of information |
| Inadequate training of staff | Wrong dosages | Social/economic barriers |
| No monitoring of treatment | Poor storage | Malabsorption, substance abuse |
Mnemonic: "3 Ps cause MDR" = Poor Provider, Poor Pills, Poor Patient compliance
Drug Grouping for Longer MDR-TB Regimens:
| Group | Drugs | Action |
|---|---|---|
| Group A (include all 3) | Levofloxacin/Moxifloxacin, Bedaquiline, Linezolid | Core backbone |
| Group B (add 1 or both) | Clofazimine, Cycloserine/Terizidone | Add-on |
| Group C (complete regimen) | Ethambutol, Delamanid, Pyrazinamide, Imipenem, Amikacin, Ethionamide, PAS | Fill in |
Mnemonic for Group A: "My Best Leprosy drugs" = Moxifloxacin/Levo + Bedaquiline + Linezolid
India MDR-TB data:
- Primary MDR-TB: ~2.8%
- Re-treatment MDR-TB: 12%
12. LATENT TB INFECTION (LTBI) TREATMENT
Who gets treated (High-risk groups):
Mnemonic: "SHIP-DIM" = Silicosis, HIV, Immigrants, Prison, Diabetes, Immunocompromised, Malnutrition/homeless
- HIV + TB co-infected
- Silicosis
- Recent contact with infectious case
- Prisoners
- Immigrants from high to low burden countries
- Homeless persons
- Illicit drug users
- Diabetes, chronic renal failure
- Children <5 years who are household contacts of PTB (high TB burden countries)
Regimens for LTBI:
| Regimen | Duration |
|---|---|
| Isoniazid daily/twice weekly | 9 months (9H) |
| INH + Rifapentine once weekly | 12 weeks (3HP) |
| Rifampicin daily | 4 months (4R) - safest option |
| INH + Rifampicin daily | 3 or 4 months |
| INH daily | 6 months |
13. TB IN SPECIAL SITUATIONS
Childhood TB:
- 6-8% of all TB in age <15 years
- Source: Usually an adult family member (smear-positive PTB)
- Children rarely smear-positive → not major source of transmission
- Risk highest in children <5 years (up to 20% develop disease within 2 years of infection)
- Commonest age: 1-4 years
- India = first country to introduce paediatric patient-wise boxes
- Diagnosis: CBNAAT preferred; Mantoux (2 TU PPD RT23); CXR; culture
TB + HIV:
- All TB patients must be tested for HIV
- HIV-positive TB patients must receive ART + Co-trimoxazole preventive therapy (CPT)
- HIV counselling and testing must NOT delay TB diagnosis
TB + Diabetes:
- Opportunistic screening for DM in all TB patients (blood sugar mandatory)
- DM triples the risk of TB
TB + COVID-19:
- Both respiratory diseases; co-infection worsens outcomes
14. PRE-TREATMENT EVALUATION
Mnemonic: "WBCBS + CXR + Pregnancy" (for DS-TB)
- Detailed history (mental illness, seizures, substance abuse)
- Weight and height
- Blood - CBC, Blood sugar (DM screen), Blood urea/creatinine (renal function)
- Chest X-ray
- Sputum (baseline)
- LFT (liver function tests)
- Urine routine
- HIV testing (mandatory)
- Pregnancy test (all women of childbearing age)
For DR-TB: Additional - Audiogram, TSH, ECG (if using Mfx, Dlm, Bdq, Cfz), Serum electrolytes, Ophthalmologist opinion
15. NIKSHAY & PROGRAMME SUPPORT
- Nikshay: India's web-based TB notification system (mandatory notification for all TB cases - government and private)
- Nikshay Poshan Yojana: DBT (Direct Benefit Transfer) of ₹500/month to TB patients for nutritional support during treatment
- TB-free India Campaign: NSP target 2017-2025 - eliminate TB by 2025
- ASHA, DOTS providers: Community-level treatment supporters
MASTER MNEMONIC FOR NTEP
"DOTS SAVES"
- DOTS strategy (5 components: PDADS)
- Objective: 85% cure + 70% detection
- Treatment: Daily FDC (2HRZE/4HRE)
- Screening: Passive + Intensified case finding
- STOP TB (6 components: PAC-EEE)
- Anti-TB drugs: RHZES first-line
- Vulnerable groups: LTBI treatment
- End TB (3 pillars: I-B-I; target eliminate by 2025/2035)
- Surveillance: Nikshay notification (mandatory)
Source: Park's Textbook of Preventive and Social Medicine (ISBN: 9789382219163)
NLEP
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I have all the data needed. Let me deliver the complete NLEP notes.
NLEP - National Leprosy Eradication Programme
Source: Park's Textbook of Preventive and Social Medicine
1. LEPROSY - THE DISEASE
Definition: Leprosy (Hansen's disease) is a chronic infectious disease caused by Mycobacterium leprae, primarily affecting the peripheral nerves, and also the skin, muscles, eyes, bones, testes, and internal organs.
Cardinal Features (at least ONE must be present for diagnosis):
Mnemonic: "SAN" = Skin patch + Anesthesia + Nerve thickening
- Hypopigmented/reddish skin lesion(s) with definite sensory loss
- Thickened peripheral nerves with loss of sensation ± weakness/paralysis
- Demonstration of M. leprae in slit-skin smear (acid-fast bacilli)
Earliest sensation affected: Light touch (before pain and temperature)
Spectrum of Disease:
Tuberculoid (TT) ←→ Borderline TT ←→ Borderline ←→ Borderline LL ←→ Lepromatous (LL)
High immunity Low immunity
Few bacilli (PB) Many bacilli (MB)
2. EPIDEMIOLOGICAL DETERMINANTS
Agent - M. leprae
- Acid-fast; occurs intracellularly + extracellularly in human host
- Grows in characteristic clumps/bundles called "GLOBI"
- Affinity for Schwann cells and reticuloendothelial cells
- Bacteria load: 2-7 billion per gram of leproma (lepromatous cases)
- NOT grown in artificial medium; grown in 9-banded armadillo and nude mouse
- Specific antigen: Phenolic Glycolipid (PGL-1)
Source of Infection
- Multibacillary cases (LL and BL) = most important source
- Inapparent infections also contribute
- All patients with "active leprosy" must be considered infectious
- Natural infection also found in armadillos, mangabey monkeys, chimpanzees
Portal of EXIT
- Nose = major portal of exit (lepromatous nasal mucosa = millions of bacilli)
- Also through ulcerated/broken skin
Portal of ENTRY
- Nose (respiratory tract) = main portal of entry
- Skin (minor route)
Infectivity
- Highly infectious, but low pathogenicity
- Rendered non-infectious by:
- Dapsone for ~90 days
- Rifampicin for 3 weeks (faster)
Host Factors
- Most susceptible: Children (family contacts)
- Immunity: Cell-mediated immunity (CMI) protects → tuberculoid end of spectrum
- Loss of CMI → lepromatous end
- Incubation period: Average 3-5 years (range: 6 months to 20 years; longest of any known bacterial disease)
Mnemonic for Incubation: "Leprosy is Leisurely" = Longest IP = 3-5 yrs average, up to 20 years
Transmission
- Prolonged close contact with untreated MB patient
- Droplet from nose (primary)
- Broken skin (secondary)
- Leprosy is NOT hereditary
3. CLASSIFICATION
WHO Classification (used in NLEP/programme):
| Feature | Paucibacillary (PB) | Multibacillary (MB) |
|---|---|---|
| Skin lesions | 1-5 | >5 |
| Nerve involvement | Only 1 nerve trunk | More than 1 nerve trunk |
| Slit skin smear | Negative | Positive |
| Ridley-Jopling | TT, BT, I | BB, BL, LL |
Mnemonic: "PB = 1-5 patches (Poor Bacilli); MB = More than 5 (Many Bacilli)"
Ridley-Jopling Classification (Spectrum):
| Type | Full Form | CMI | Bacilli |
|---|---|---|---|
| TT | Tuberculoid | High | Absent/very few |
| BT | Borderline Tuberculoid | Moderate-high | Few |
| BB | Mid-Borderline | Unstable | Moderate |
| BL | Borderline Lepromatous | Low | Many |
| LL | Lepromatous | Absent | Many (globi) |
| I | Indeterminate | Variable | Variable |
4. DIAGNOSIS
Cardinal Signs (minimum 1 needed):
- Hypopigmented patch with sensory loss
- Thickened nerve + loss of sensation ± motor deficit
- AFB in slit-skin smear
Commonly Affected Nerves:
Mnemonic: "ULTRA-P" = Ulnar, Lesser occipital (Greater auricular), Tibial, Radial, Abducent/Facial, Peroneal
| Nerve | Deformity Caused |
|---|---|
| Ulnar | Claw hand (ring + little finger) |
| Median | Claw hand (index + middle finger) |
| Radial | Wrist drop |
| Common peroneal | Foot drop |
| Posterior tibial | Claw toes, plantar anesthesia |
| Facial (zygomatic branch) | Lagophthalmos (eye cannot close) |
| Greater auricular | Thickened, visible |
| Lateral popliteal | Foot drop |
Slit-Skin Smear (SSS):
- Site: Active lesion + ear lobe
- "Slit and scrape" method; stained with Ziehl-Neelsen
- Bacterial Index (BI): Measures bacillary load (0 to 6+)
- Morphological Index (MI): % of solid-staining (viable) bacilli - used to assess treatment response
Lepromin Test (Mitsuda Test):
- NOT a diagnostic test (cannot diagnose leprosy)
- Measures cell-mediated immunity (CMI)
- Read at 28 days (Mitsuda reaction - papule/nodule >5 mm = positive)
- Positive in TT, Negative in LL
- Used to classify leprosy and assess prognosis
5. MDT - MULTI-DRUG THERAPY
Introduced by WHO in 1982 - the cornerstone of NLEP
Why MDT? Because of:
- Primary and secondary dapsone resistance
- Need to kill persisters
- Reduce treatment duration
MDT Regimens (WHO):
Adults - Multibacillary (MB) Leprosy:
| Drug | Dose | How Given |
|---|---|---|
| Rifampicin | 600 mg | Once monthly, supervised |
| Dapsone | 100 mg | Daily, self-administered |
| Clofazimine | 300 mg monthly + 50 mg daily | Monthly supervised + daily self |
Adults - Paucibacillary (PB) Leprosy:
| Drug | Dose | How Given |
|---|---|---|
| Rifampicin | 600 mg | Once monthly, supervised |
| Dapsone | 100 mg | Daily, self-administered |
Children (10-14 years) - MB:
- Rifampicin 450 mg once monthly (supervised)
- Dapsone 50 mg daily (self)
- Clofazimine 150 mg monthly (supervised) + 50 mg alternate days
Children (10-14 years) - PB:
- Rifampicin 450 mg once monthly (supervised)
- Dapsone 50 mg daily (self)
Mnemonic for MB: "RDC" = Rifampicin + Dapsone + Clofazimine Mnemonic for PB: "RD" = Rifampicin + Dapsone
Duration:
| Type | Duration | Completion deadline |
|---|---|---|
| MB | 12 months (12 blisterpacks) | Within 18 months |
| PB | 6 months (6 blisterpacks) | Within 9 months |
Mnemonic: "MB = 12/18; PB = 6/9" (double the time as cushion for defaults)
Key Drug Points:
- Rifampicin: Most potent bactericidal; renders patient non-infectious within 3 weeks
- Dapsone: Bacteriostatic; cheapest; resistance can develop (hence MDT)
- Clofazimine: Bactericidal + anti-inflammatory (reduces reactions); causes skin discolouration (reddish-brown) - if unacceptable, substitute ethionamide/protionamide
6. LEPROSY REACTIONS
Two types of immunological reactions that can occur during/after treatment:
Mnemonic: "T1 = Type 1 = Tuberculoid (Reversal Reaction); T2 = Type 2 = Two-system (ENL)"
| Feature | Type 1 (Reversal Reaction) | Type 2 (ENL - Erythema Nodosum Leprosum) |
|---|---|---|
| Immunology | Cell-mediated (delayed hypersensitivity) | Immune complex (Humoral) |
| Who gets it | BT, BB, BL | BL, LL |
| Skin | Existing patches become red, raised, swollen | New tender red nodules appear |
| Nerves | Sudden nerve damage (acute neuritis) | May have neuritis |
| Systemic features | None | Fever, malaise, iridocyclitis, orchitis |
| Treatment | Corticosteroids (Prednisolone) | Thalidomide (males); Clofazimine; Steroids |
Continue MDT during reactions - never stop MDT for reactions!
7. DISABILITY GRADING
Mnemonic: "0-1-2 = Zero, Look, Lost"
| Grade | Hands/Feet | Eyes |
|---|---|---|
| Grade 0 | No anesthesia, no deformity | No eye problem |
| Grade 1 | Anesthesia present, NO visible deformity | Reduced vision but visual acuity >6/60 |
| Grade 2 | Visible deformity/damage (claw hand, foot drop, ulcer) | Severe visual impairment <6/60; lagophthalmos |
8. HISTORY OF NLEP
Mnemonic: "Control → Eradication → World Bank → Integrated"
| Year | Event |
|---|---|
| 1874 | Mission to Lepers founded by Baily at Chamba, HP (first organized anti-leprosy work in India) |
| 1954 | NLCP (National Leprosy Control Programme) launched - centrally aided; dapsone monotherapy |
| 1980 | Govt of India declared resolve to "eradicate" leprosy by year 2000 |
| 1982 | Working Group submitted report; recommended MDT-based strategy |
| 1983 | NLCP renamed NLEP (National Leprosy Eradication Programme) |
| 1993 | 1st World Bank supported project |
| 2001 | 2nd World Bank project (ended December 2004) |
| 2002-03 | Integrated with general health care system; services at all PHCs |
| 2005 | India achieved elimination at national level (PR < 1 per 10,000) |
Elimination threshold: Prevalence Rate (PR) < 1 case per 10,000 population
9. NLEP - PROGRAMME DETAILS
Goal:
Eliminate leprosy (PR <1/10,000) at sub-district (block) level
5 Components of NLEP:
Mnemonic: "DICIM" = Decentralized, Integration, Capacity, IEC, Monitoring
- Decentralized integrated leprosy services through general health care system
- Integration - capacity building of general health services staff
- Capacity building of all functionaries
- Intensified IEC (Information, Education, Communication)
- Monitoring - Prevention of Disability + Medical Rehabilitation (DPMR) + intensified supervision
Key Indicators:
- ANCDR (Annual New Case Detection Rate) - main monitoring indicator (replaced prevalence)
- Treatment Completion Rate - calculated by states yearly
- PR - Prevalence Rate (elimination target: <1/10,000)
Status of India (current data from textbook):
- 34 states/UTs achieved elimination (PR <1/10,000)
- Chhattisgarh and Dadra & Nagar Haveli: PR of 2-5/10,000 (pending)
- Bihar, Goa, Chandigarh, Odisha: achieved elimination but PR slipped back >1/1,000
- 209 high-endemic districts identified for special action
10. MAJOR INITIATIVES UNDER NLEP
ASHA Involvement:
ASHAs paid incentive for leprosy work (ASHA-Based Surveillance for Leprosy Suspects = ABSULS, launched 1st July 2019):
| Activity | Incentive |
|---|---|
| Confirmed diagnosis of brought case | Rs. 250/- |
| Treatment completion - PB case | Rs. 400/- |
| Treatment completion - MB case | Rs. 600/- |
| Early case (no visible deformity) | Rs. 250/- |
| New case with visible deformity | Rs. 200/- |
DPMR - Disability Prevention & Medical Rehabilitation:
- Dressing materials, ulcer kits, supportive medicines
- Micro-cellular rubber (MCR) footwear for insensitive feet
- 83 centres (41 NGOs + 42 Govt Medical Colleges) for reconstructive surgery
- Rs. 5,000/- incentive for BPL patients undergoing reconstructive surgery
- Rs. 8,000/- for ALL patients undergoing major reconstructive surgery (irrespective of financial status)
- 115 RCS centres (61 Government + 54 NGO) as of January 2017
Sparsh Leprosy Awareness Campaign:
- Launched: 2017
- Through Gram Sabhas, Panchayat, Village Health and Sanitation Committees
- Aim: Generate awareness, reduce stigma, improve self-reporting
- Covered 60% of total villages across India
SET Scheme (Survey, Education, Treatment):
- NGOs involved in: disability prevention, ulcer care, IEC, referral for RCS, research, rehabilitation
Research Institutions:
- Central JALMA Institute of Leprosy - Agra
- Central Leprosy Teaching and Training Institute - Chingleput (Chennai)
- Regional Training and Referral Institutes at Aska (Odisha), Raipur (Chhattisgarh), Gouripur (West Bengal)
International Support:
- ILEP (International Federation of Anti-Leprosy Associations) - 10 agencies in India
- WHO technical support
11. CONTROL MEASURES SUMMARY
Medical Measures (10):
Mnemonic: "EECM-SIDRH" or just remember these 10:
- Estimation of the problem (surveys)
- Early case detection (passive + active)
- Chemotherapy = MDT
- Monitoring
- Surveillance
- Immunoprophylaxis (BCG - partial protection ~50%)
- Chemoprophylaxis (dapsone for contacts in some settings)
- Deformity prevention (DPMR)
- Rehabilitation
- Health education
3 Goals of Leprosy Control:
- Interrupt transmission → reduce incidence
- Treat patients → cure + rehabilitation
- Prevent deformities
BCG Vaccination:
- Gives partial protection (~50%) against leprosy
- Correlation: positive lepromin test after BCG = protective immunity
- Countries with good BCG coverage show lower leprosy rates
MASTER EXAM MNEMONICS SUMMARY
| Topic | Mnemonic |
|---|---|
| Cardinal features | SAN = Skin + Anesthesia + Nerve |
| MB drugs | RDC = Rifampicin + Dapsone + Clofazimine |
| PB drugs | RD = Rifampicin + Dapsone |
| MB duration | 12/18 months |
| PB duration | 6/9 months |
| Classification | PB = 1-5 patches; MB = >5 patches |
| Reactions | T1 = reversal (CMI); T2 = ENL (immune complex) |
| Disability grade | 0 = normal; 1 = anaesthesia; 2 = visible deformity |
| History | 1954 NLCP → 1983 NLEP → 2005 Elimination |
| NLEP components | DICIM |
| Programme indicator | ANCDR (not PR anymore) |
| Sparsh campaign | 2017 - stigma reduction |
| ABSULS | 2019 - ASHA surveillance |
Source: Park's Textbook of Preventive and Social Medicine (ISBN: 9789382219163)
Polio and national programme for it
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I have all the information needed. Now compiling the complete, well-structured notes.
Poliomyelitis & National Programme (Pulse Polio / UIP)
Source: Park's Textbook of Preventive and Social Medicine
1. POLIOMYELITIS - THE DISEASE
Definition: Poliomyelitis is an acute viral infection caused by an RNA virus (Poliovirus). It primarily infects the human alimentary tract, but the virus may infect the CNS in ~1% of cases, causing varying degrees of paralysis and possibly death.
2. EPIDEMIOLOGICAL DETERMINANTS
Agent - Poliovirus
| Feature | Detail |
|---|---|
| Type | RNA enterovirus |
| Serotypes | 3 types - Type 1, 2, 3 |
| Most paralytogenic | Type 1 (Wild Poliovirus = WPV1) |
| Most VAPP-associated | Type 3 (Sabin 3) - 60% of VAPP cases |
| Type 2 last detected | 1999 (declared eradicated September 2015) |
| Type 3 last detected | November 2012 |
Mnemonic for types: "1 Paralyses, 2 Perished, 3 VAPP" = Type1 most paralytic, Type2 eradicated, Type3 causes most VAPP
Source of Infection
- Humans (patients + inapparent/subclinical cases)
- Inapparent infections vastly outnumber clinical cases
Portal of Exit
- Faeces (primary - virus shed in stools for weeks)
- Pharyngeal secretions (early, short-lived)
Mode of Transmission
- Faeco-oral route (main) - contaminated water/food
- Droplet/contact (oral-pharyngeal secretions, early)
"Polio = Poop to Mouth" - faeco-oral is dominant
Portal of Entry
- Oropharynx and intestinal tract
Incubation Period
- Range: 3-35 days
- Typically 7-14 days
- For paralytic disease: 7-21 days
Host Factors
- Most susceptible: Children under 5 years (hence "Infantile Paralysis")
- Immunity: Type-specific and life-long after infection
- Risk factors for paralysis: Tonsillectomy, IM injections during incubation ("provocation paralysis"), pregnancy, physical exertion, immunodeficiency
3. CLINICAL SPECTRUM
Mnemonic: "AMAB" = Asymptomatic → Minor → Abortive → Big (Major)
| Form | % of cases | Features |
|---|---|---|
| Inapparent/Subclinical | ~90-95% | No symptoms; still shed virus; most common |
| Abortive (Minor illness) | ~4-8% | Fever, headache, sore throat, GI symptoms; NO CNS involvement; recovers fully |
| Non-paralytic (Aseptic meningitis) | ~1% | Meningeal signs; no paralysis; full recovery |
| Paralytic | ~0.1-1% | Flaccid paralysis; asymmetric; lower limbs; ± bulbar |
Types of Paralytic Polio:
- Spinal (most common) - anterior horn cells affected; flaccid, asymmetric paralysis of limbs; lower limbs > upper
- Bulbar - cranial nerve nuclei affected; respiratory/swallowing muscles → life-threatening
- Bulbospinal - combined
Hallmarks of Paralytic Polio:
- Asymmetric flaccid paralysis
- Fever at onset
- Rapid onset (24-48 hours)
- No sensory loss
- Proximal muscles > distal
- Residual paralysis at 60 days = diagnostic criterion
4. DIAGNOSIS
Case Definition (WHO - for AFP surveillance):
Suspected Polio: Any child under 15 years with Acute Flaccid Paralysis (AFP) of one or more limbs
Confirmed Polio: AFP case with wild poliovirus isolated from stool specimen
AFP Surveillance - 4 Steps:
Mnemonic: "FILM" = Find, Isolate (lab), Locate (map), Move (stool samples)
- Find and report AFP cases in children <15 years
- Move stool samples - 2 specimens, 24-48 hours apart, within 48 hours of onset, stored at 4-8°C, reach lab within 72 hours
- Isolate poliovirus in lab; distinguish WPV from vaccine virus
- Map the virus - genetic typing to trace geographic origin
AFP Surveillance Indicators:
- Non-Polio AFP Rate (NP-AFP): Should be ≥2 per 1,00,000 children under 15 (indicates sensitive surveillance)
- Stool adequacy: 2 adequate specimens from ≥80% of AFP cases
- Follow-up all AFP cases at 60 days to check residual paralysis
5. VACCINES - COMPARISON (HIGH YIELD)
OPV vs IPV - The Classic Comparison:
| Feature | OPV (Oral Polio Vaccine / Sabin) | IPV (Inactivated Polio Vaccine / Salk) |
|---|---|---|
| Type | Live attenuated | Killed (inactivated) |
| Route | Oral (2 drops) | IM injection (or fID - fractional intradermal) |
| Immunity - Humoral | Yes (IgG, IgM) | Yes (IgG, IgM, IgA serum) |
| Immunity - Intestinal (IgA) | YES (mucosal immunity) | NO |
| Herd immunity | YES - excreted in stool, spreads to unvaccinated contacts | NO - virus can still multiply in gut; no community benefit |
| VAPP risk | YES - 4 cases/10 lakh birth cohort | None |
| Stability | Less stable - needs cold chain | More stable at ambient temperature; avoid freezing |
| Use in immunocompromised | CONTRAINDICATED (live virus) | SAFE |
| Use in pregnancy | Caution | Safe |
| Use in epidemic | YES (rapid immunity, single dose) | NO (slow, needs multiple doses; IM in epidemic provokes paralysis) |
| Cost | Cheaper | Expensive |
Mnemonic: "OPV = Oral Gut-immunity, Herd immunity; IPV = Injected blood-only immunity"
OPV Details:
- Composition: trivalent (tOPV) - types 1, 2, 3; now replaced by bOPV (types 1 and 3 only) after 2016 switch
- Dose: 2 drops orally
- Schedule (India): Birth + 6, 10, 14 weeks (as part of UIP) + booster at 16-24 months
- Storage: 2-8°C; freezing enhances potency (unlike most vaccines)
- Contraindications: Immunodeficiency states (HIV, steroid therapy)
- VAPP: Most commonly from Type 3 (Sabin 3) - 60% of cases; occurs in both recipients and unimmunized contacts
IPV Details:
- Composition: Inactivated types 1, 2, 3 (D-antigen: 40 + 8 + 32 units)
- Route: IM or fractional IPV (fIPV) - 0.1 ml intradermal (India)
- India schedule: fIPV at 6 weeks and 14 weeks
- Introduced in India: 30 November 2015 (as part of Endgame strategy)
- Advantages: Safe in immunocompromised, pregnancy, elderly
- Disadvantage: No intestinal/mucosal immunity; cannot stop gut replication/shedding
6. VACCINE-DERIVED POLIOVIRUS (VDPV)
- OPV virus can undergo genetic changes during replication
- In communities with low vaccination coverage, mutant attenuated virus can become neurovirulent = VDPV
- VDPV paralysis is clinically indistinguishable from WPV paralysis
- Diagnosed by: rRT-PCR (real-time reverse transcription PCR)
Types of VDPV:
Mnemonic: "CIA" = Circulating, Immunodeficiency, Ambiguous
| Type | Description |
|---|---|
| cVDPV | Person-to-person transmission in community; same threat as WPV |
| iVDPV | From persons with primary immunodeficiency; prolonged excretion |
| aVDPV | Ambiguous - clinical isolates from person with no known immunodeficiency OR sewage isolates |
- Most cVDPV and VAPP = Type 2 (was in tOPV) → reason for tOPV → bOPV switch
7. GLOBAL ERADICATION TIMELINE
Mnemonic: "1988 - 125 countries; 1999 - Type 2 gone; 2012 - Type 3 gone; 2014 - India free; 2015 - Type 2 declared eradicated"
| Year | Event |
|---|---|
| 1988 | World Health Assembly resolution to eradicate polio globally; >125 endemic countries |
| 1994 | Americas declared polio-free |
| 1999 | Last WPV Type 2 case (Aligarh, India) |
| 2000 | Western Pacific Region declared polio-free |
| 2002 | European Region declared polio-free |
| 2012 | Last WPV Type 3 case (November 2012) |
| 2013 | Polio Eradication and Endgame Strategic Plan 2013-2018 launched |
| 2014 | India certified polio-free: 27th March 2014 |
| 2015 | WPV Type 2 declared eradicated (September 2015) |
| 2015 | IPV introduced in India (30 November 2015) |
| 2016 | tOPV → bOPV switch (18 April - 1 May 2016) |
| 2017 | Only 3 endemic countries: Afghanistan (14 cases), Pakistan (8), Nigeria (4); all WPV1 |
8. POLIO ERADICATION ENDGAME STRATEGIC PLAN 2013-2018
3 Key Steps:
- Introduce at least 1 dose of IPV into all routine immunization systems by end 2015 (at least 6 months before switch)
- Switch from tOPV to bOPV in 2016 (synchronized global cessation of OPV type 2 use)
- Plan for eventual withdrawal of all OPV
Why switch tOPV → bOPV?
- WPV Type 2 absent since 1999
- Risk of VAPP and cVDPV2 from OPV type 2 now outweighs benefits
- 97% of global cVDPV and 40% of global VAPP = due to type 2 component
9. NATIONAL PROGRAMME - INDIA
A. Universal Immunization Programme (UIP)
- Launched: 1985-86 (as Expanded Programme on Immunization started 1978)
- OPV given as routine immunization: Birth, 6, 10, 14 weeks + booster doses
- Covers all vaccine-preventable diseases under national schedule
B. Pulse Polio Immunization (PPI) Programme
- Launched in India: 1995
- First NIDs (National Immunization Days): 2nd December 1995 and 3rd January 1996
Target: All children under 5 years of age
Strategy:
- Additional OPV drops given on fixed days (usually December and January each year)
- From 1999-2000: House-to-house vaccination of missed children added
- NIDs (National Immunization Days): Cover ~172 million children
- SNIDs (Sub-National Immunization Days): Cover ~40-80 million children
C. Strategies for Polio Eradication in India:
Mnemonic: "PULSE CAMP" = Pulse Polio, UIP sustained, Line listing, Surveillance-AFP, Collect stools, Alert (outbreak control), Mopping up, Prevention (follow-up at 60 days)
- Conduct Pulse Polio Immunization days every year
- Sustain high levels of routine immunization coverage
- Monitor OPV coverage at district level and below
- AFP surveillance - detect all AFP cases (polio + non-polio)
- Rapid case investigation - collect stool samples for virus isolation
- Follow-up all AFP cases at 60 days for residual paralysis
- Outbreak control within 48 hours of notification
- Mopping Up - door-to-door immunization in high-risk districts
D. Mopping Up:
- Last stage of eradication
- Door-to-door immunization in high-risk districts where WPV known/suspected
- Used to catch children missed during fixed-post campaigns
E. Line Listing of Cases:
- Started: 1989
- Purpose: Check for duplication, track high-risk areas, document age distribution, guide follow-up
F. AFP Reporting:
Report to Chief Medical Officer/District Immunization Officer with:
- Name, age, sex, father's name, complete address
- Vaccination status
- Date of onset of paralysis + date of reporting
- Clinical diagnosis
- Doctor's name and contact
G. Introduction of IPV in India (Endgame Strategy):
- IPV introduced: 30 November 2015
- Given as fractional IPV (fIPV): 0.1 ml intradermal at 6 weeks and 14 weeks
- Reason: Mitigate risk of VDPV type-2 after tOPV withdrawal
H. Key Milestones - India:
| Year | Event |
|---|---|
| 1978 | EPI (Expanded Programme on Immunization) launched |
| 1985-86 | UIP launched |
| 1992 | AFP surveillance extended to all causes |
| 1995 | Pulse Polio Programme launched |
| 1999-2000 | House-to-house vaccination of missed children added |
| 1999 | Last WPV Type 2 case (Aligarh) |
| 2011 | Only 1 case of polio (January 2011 - last case in India) |
| 25 Feb 2012 | India removed from list of polio endemic countries |
| 27 March 2014 | India certified polio-free |
| 30 Nov 2015 | IPV introduced in India |
10. MASTER COMPARISON TABLE - OPV vs IPV
| Feature | OPV | IPV |
|---|---|---|
| Inventor | Sabin | Salk |
| Year | 1961 | 1955 |
| Type | Live attenuated | Killed |
| Route | Oral (2 drops) | IM / fID (0.1 ml) |
| Intestinal IgA | YES | NO |
| Herd immunity | YES | NO |
| VAPP | YES (4/10 lakh) | NO |
| Immunocompromised | CONTRA | SAFE |
| Epidemic use | YES | NO |
| Cold chain | 2-8°C (freeze = better) | 2-8°C (do NOT freeze) |
| India schedule | Birth, 6, 10, 14 wks + booster | 6 wks + 14 wks (fIPV) |
| India introduction | 1985 (EPI) | 30 Nov 2015 |
11. HIGH-YIELD EXAM POINTS WITH MNEMONICS
| Fact | Mnemonic |
|---|---|
| ~90-95% infections are inapparent | "Polio is mostly SILENT" |
| Paralytic polio = ~1% | "1% get Paralysed" |
| AFP surveillance rate = ≥2/1,00,000 under 15 | "TWO alert triggers" |
| Stool specimens: 2 samples, 24-48 hrs apart | "Poop TWICE in 2 days" |
| Specimens reach lab within 72 hours | "72 hours = 3 days = triple urgent" |
| Residual paralysis check at 60 days | "60 day CHECKUP" |
| India polio-free date = 27 March 2014 | "27/3/14 = India FREE" |
| Pulse Polio launched 1995 | "1995 = Pulse starts" |
| Last Indian polio case = January 2011 | "2011 = Adios Polio" |
| fIPV = 0.1 ml ID at 6 and 14 weeks | "Six + fourteen ID" |
| tOPV switch to bOPV = April 2016 | "2016 TYPE 2 EXITS" |
| Type 2 last WPV = 1999, eradicated 2015 | "99 last seen, 15 declared dead" |
| VAPP most common from Sabin 3 = 60% | "3 causes SIXTY percent VAPP" |
| OPV contraindicated in immunodeficiency | "Live virus = Lethal in immunodeficient" |
Source: Park's Textbook of Preventive and Social Medicine (ISBN: 9789382219163)
This is a shared conversation. Sign in to Orris to start your own chat.