Cyanotic and acyanotic Congenital heart defects
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have rich textbook content and diagrams. Let me compile the complete response.
Congenital Heart Defects: Cyanotic and Acyanotic
Congenital heart defects (CHDs) affect approximately 1 in 100 live births. They are broadly classified into acyanotic (~75%) and cyanotic (~25%) based on whether deoxygenated blood enters the systemic circulation. CHD most commonly arises from faulty embryogenesis during gestational weeks 3-8, with the cause unknown in ~90% of cases.
Incidence of major CHDs (per million live births):
| Malformation | Incidence | % |
|---|---|---|
| Ventricular septal defect (VSD) | 4,482 | 42% |
| Atrial septal defect (ASD) | 1,043 | 10% |
| Pulmonary stenosis | 836 | 8% |
| Patent ductus arteriosus (PDA) | 781 | 7% |
| Tetralogy of Fallot | 577 | 5% |
| Coarctation of aorta | 492 | 5% |
| Transposition of great arteries | 388 | 4% |
| Truncus arteriosus | 136 | 1% |
| TAPVC | 120 | 1% |
| Tricuspid atresia | 118 | 1% |
ACYANOTIC CONGENITAL HEART DEFECTS
Acyanotic defects involve left-to-right shunts (oxygenated blood recirculates into the lungs) or obstructive lesions without shunting. Cyanosis is not an early feature. They typically present as heart failure or murmur in infancy.
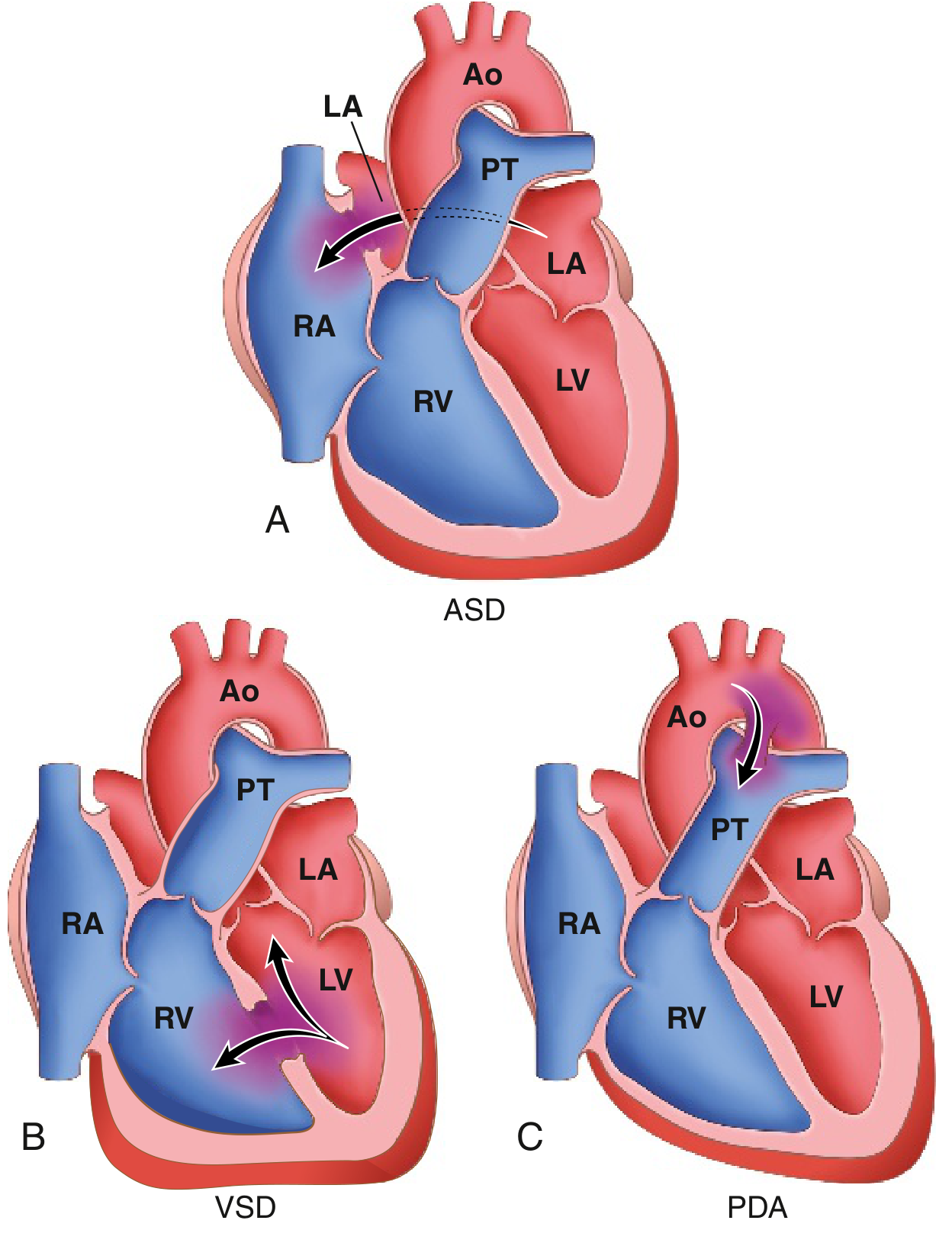
Key mechanism: Prolonged left-to-right shunting raises pulmonary vascular resistance, causing pulmonary hypertension that eventually reverses the shunt direction -- this is Eisenmenger syndrome, at which point cyanosis appears and defects become irreversible.
1. Atrial Septal Defect (ASD)
- Defect: Fixed opening in the atrial septum allowing left-to-right shunt (LA pressure > RA pressure)
- Types:
- Ostium secundum (90%): Near foramen ovale; most common. Usually isolated.
- Ostium primum (5%): Lowest part of septum; may be associated with mitral/tricuspid valve abnormalities and AV canal defects
- Sinus venosus (5%): High in atrial septum; often with anomalous pulmonary venous drainage
- Hemodynamics: Right atrial and ventricular dilation, RV hypertrophy, dilated pulmonary artery
- Note: Distinguish from PFO - a patent foramen ovale is a flap valve, not a true fixed defect; it can allow paradoxical embolism but usually is clinically silent
- Clinical features:
- Usually asymptomatic until adulthood (most common CHD presenting in adults)
- Fixed, widely split S2 is the hallmark auscultatory finding
- Chest X-ray: cardiomegaly, increased pulmonary vascular markings
- ECG: RVH, right axis deviation (RAD), incomplete RBBB
- Treatment: Surgical or transcatheter closure to prevent CHF, paradoxical embolism, irreversible pulmonary vascular disease. Mortality is low.
2. Ventricular Septal Defect (VSD)
- Most common CHD diagnosed at birth (~42% of all CHDs)
- Defect: Opening in ventricular septum; ~90% in the membranous (basal) portion
- Hemodynamics: Left-to-right shunt → RV hypertrophy, increased pulmonary blood flow and pressure, LV volume overload
- Clinical features:
- Small VSDs: asymptomatic; harsh pansystolic murmur at lower left sternal border (LLSB). About 50% close spontaneously in childhood
- Large VSDs: CHF, failure to thrive, recurrent pulmonary infections, risk of Eisenmenger syndrome earlier than ASD
- ECG: LVH or biventricular hypertrophy
- Treatment: Small defects observed. Larger defects: surgical patch closure. VSD may be isolated or part of Tetralogy of Fallot, trisomy 21, etc.
3. Patent Ductus Arteriosus (PDA)
- Defect: Failure of the ductus arteriosus to close after birth (normally closes within 1-2 days in response to increased O2, decreased PGE2)
- Shunt: Aorta (higher pressure) → left pulmonary artery → pulmonary circulation (left-to-right)
- Murmur: Classic "machinery-like" continuous murmur, best heard at upper left sternal border
- Clinical features:
- Small PDA: asymptomatic
- Large PDA: pulmonary hypertension, LV dilation, risk of infective endocarditis, eventual Eisenmenger syndrome
- Associated with prematurity, maternal rubella, Down syndrome
- Treatment: Indomethacin (inhibits prostaglandins, stimulates closure) in premature infants; surgical or catheter-based closure in term infants and adults
4. Aortic Coarctation
- Defect: Narrowing of the aorta, classically at or near the ductus arteriosus (juxtaductal). Males > females (2:1); females with Turner syndrome frequently have coarctation
- Two presentations:
- Infantile type (preductal): Severe obstruction; presents with heart failure in neonate; requires urgent intervention
- Adult type (postductal): Collateral circulation develops; presents with upper extremity hypertension, differential arm-leg blood pressure, weak/delayed femoral pulses
- Examination finding: Radio-femoral pulse delay; rib notching on CXR (from collateral intercostal arteries)
- Associations: Bicuspid aortic valve (in 50%), berry aneurysms, Turner syndrome
- Treatment: Surgical resection and anastomosis, or balloon angioplasty with stenting
5. Pulmonary Stenosis
- Defect: Obstruction at the level of the pulmonary valve
- Clinical: Systolic ejection murmur at upper left sternal border; right ventricular hypertrophy; usually well tolerated
- Treatment: Balloon pulmonary valvuloplasty for moderate-to-severe stenosis
6. Aortic Stenosis (Congenital)
- Defect: Obstruction at the aortic valve level (commonly bicuspid valve), subvalvular, or supravalvular
- Clinical: Systolic ejection murmur at upper right sternal border; LV hypertrophy; risk of sudden cardiac death with severe stenosis
CYANOTIC CONGENITAL HEART DEFECTS
Cyanotic defects involve right-to-left shunts, meaning deoxygenated blood bypasses the lungs and enters systemic circulation, producing cyanosis, clubbing, and polycythemia. They account for ~25% of CHDs and are more complex.
Systemic consequences of chronic cyanosis:
- Clubbing (hypertrophic osteoarthropathy)
- Polycythemia (erythropoietin-driven, due to hypoxia)
- Paradoxical embolization (venous clots enter systemic circulation)
- Infective endocarditis risk
1. Tetralogy of Fallot (TOF)
Most common cyanotic CHD (~5% of all CHDs; most common cyanotic defect surviving to 1 year)
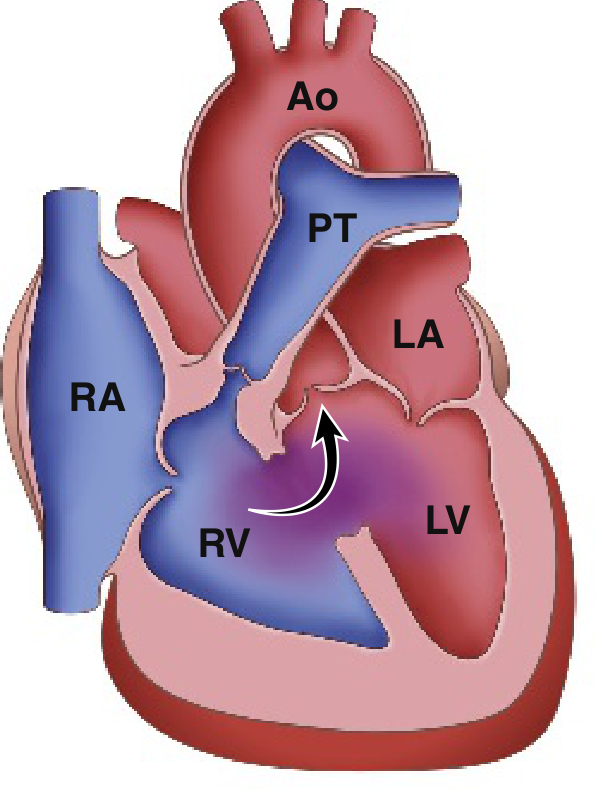
Four cardinal features (all result from anterosuperior displacement of the infundibular septum):
- Large VSD
- Right ventricular outflow tract (RVOT) obstruction - subpulmonic/infundibular stenosis
- Overriding aorta (aortic valve overlies the VSD)
- Right ventricular hypertrophy
Pathophysiology: RVOT obstruction → RV pressure rises → right-to-left shunting across VSD → deoxygenated blood enters aorta → cyanosis. Severity depends on degree of pulmonary obstruction.
Clinical features:
- Cyanosis at birth or developing within first year
- "Tet spells" (hypercyanotic spells): Episodes of severe cyanosis with tachypnea, loss of consciousness, worsening with crying/feeding - due to spasm of RVOT
- Squatting in older children (increases SVR, reduces right-to-left shunt, improves pulmonary blood flow)
- Chest X-ray: "Boot-shaped heart" (coeur en sabot) - RV hypertrophy elevates cardiac apex, hypoplastic pulmonary trunk
- ECG: Right axis deviation, RVH
Management of tet spells: Knee-chest position, oxygen, IV morphine (decreases hyperpnea), phenylephrine (increases SVR), IV propranolol (relaxes RVOT spasm)
Surgical repair: Patch VSD closure + resection of obstructing infundibular septum. Done at 4-6 months when possible. Late survival ~95% at 5-10 years.
2. Transposition of the Great Arteries (TGA/TGV)
Most common cyanotic CHD presenting in the newborn period
- Defect: Aorta arises from the RV; pulmonary artery arises from the LV - completely reversed
- Result: Systemic and pulmonary circulations run in parallel rather than in series - incompatible with life without a mixing shunt
- Mixing occurs via PFO, PDA, or VSD (present in ~1/3 of cases)
Clinical features:
- Severe cyanosis within 48 hours of birth
- Chest X-ray: "Egg on a string" appearance - narrow superior mediastinum (aorta directly anterior to PA) with cardiomegaly; increased pulmonary vascular markings
- ECG: RAD, RVH
Management:
- Prostaglandin E1 (alprostadil) IV - keeps PDA open to maintain mixing
- Balloon atrial septostomy (Rashkind procedure) - creates ASD for mixing
- Definitive treatment: Arterial switch operation (Jatene procedure) - performed within first few weeks of life; excellent long-term outcomes
3. Total Anomalous Pulmonary Venous Connection (TAPVC)
- Defect: Pulmonary veins drain into systemic venous system (SVC, RA, coronary sinus, IVC) instead of the left atrium. An ASD or PFO must be present for survival.
- Types:
- Supracardiac (most common): drains into SVC
- Cardiac: drains into coronary sinus or RA
- Subdiaphragmatic (infradiaphragmatic): drains into IVC/portal vein - associated with obstruction
- Clinical: Moderate-to-mild cyanosis (mild if unobstructed), pulmonary congestion
- Chest X-ray: "Snowman" sign (figure-of-8) - only seen after age 4 months in supracardiac type
4. Tricuspid Atresia
- Defect: Absent tricuspid valve with hypoplastic RV; requires ASD + PDA or VSD to survive
- ECG hallmark: Superior QRS axis (left axis deviation) + LVH - distinguishes it from other cyanotic CHDs
- Treatment: Palliative staged procedures (Fontan circulation)
5. Truncus Arteriosus
- Single common arterial trunk arising from the heart, supplying systemic, pulmonary, and coronary circulations. Always associated with a large VSD.
- Associated with DiGeorge syndrome (22q11 deletion)
6. Ebstein Anomaly
- Defect: Downward displacement of a malformed tricuspid valve into the RV cavity, "atrialization" of the RV
- Variable severity; may present with cyanosis (right-to-left shunt through ASD/PFO), WPW syndrome (accessory pathway), arrhythmias
- Associated with maternal lithium use
Comparison Summary
| Feature | Acyanotic (L→R shunt) | Cyanotic (R→L shunt) |
|---|---|---|
| Oxygen saturation | Normal initially | Low (SpO2 <85%) |
| Cyanosis | Absent early; appears with Eisenmenger | Present at birth or soon after |
| Pulmonary blood flow | Increased | Decreased (TOF) or Mixed/Increased (TGA) |
| Common examples | VSD, ASD, PDA, CoA | TOF, TGA, TAPVC, Tricuspid atresia |
| % of CHDs | ~75% | ~25% |
| Presentation | Murmur, CHF | Blue baby, hypoxic spells |
| Clubbing/polycythemia | Not typically | Yes (chronic cyanosis) |
Eisenmenger Syndrome
This is the final common pathway for any large, uncorrected left-to-right shunt. Chronic pulmonary overcirculation causes pulmonary vascular remodeling and rising pulmonary hypertension. When pulmonary arterial pressure exceeds systemic pressure, the shunt reverses to right-to-left, and the patient becomes cyanotic. At this stage, repair of the underlying defect is contraindicated. Management is pulmonary vasodilator therapy (bosentan, sildenafil).
Sources:
- Robbins & Kumar Basic Pathology, Chapter 9 (Cardiovascular)
- Gray's Anatomy for Students, Chapter 3
- Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 59
- Harriet Lane Handbook, 23rd Ed., Chapter 7 (Cardiology)
- Fuster and Hurst's The Heart, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.