Bitton battery ingestion as foreign body. Where are the possible location that it can get lodged? How long does it take to pass through each part of gastrointestinal tract, give me the time duration? When does the intervention is needed? When does the intervention is not required? And all other clinically important details that i need to know about foreign body ingestion especially botton battery
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
button battery ingestion management guidelines lodgment sites GI tract transit time intervention 2024
Reading File
Reading File
Reading File
Finding Sources
Reading Web Page
https://www.poison.org/battery/guideline
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive, authoritative answer. Let me compile it:
Button Battery Ingestion - Complete Clinical Guide
Button battery (BB) ingestion is one of the most dangerous foreign body emergencies in pediatrics. Unlike coins, these batteries cause injury through multiple simultaneous mechanisms and can be lethal within hours if not recognized and managed correctly.
1. Mechanism of Injury
Batteries cause tissue damage through four simultaneous mechanisms:
- Electrolysis / electrical current - When both poles contact moist mucosa, an external electrical circuit forms, hydrolyzing tissue fluid and generating hydroxide at the negative terminal, rapidly raising local pH (liquefactive alkaline necrosis)
- Pressure necrosis - Direct mechanical compression at the lodgment site
- Alkaline leakage - Battery electrolyte leaks in a saline environment, causing chemical burns
- Release of toxic compounds - Mercury and other heavy metals cause systemic toxicity
Tissue injury begins within 15 minutes. Serious burns occur within 2-2.5 hours. Perforation can occur within 6 hours.
The 20 mm lithium coin cell (CR2032) causes disproportionately severe injury due to its higher voltage (3V vs 1.5V) and larger diameter. The highest-risk scenario is a 20 mm battery in a child under 4 years old.
- Rosen's Emergency Medicine, p. 1221
- Scott-Brown's Otorhinolaryngology (Vol 2), p. 434
- Tintinalli's Emergency Medicine, Chapter 77
2. Sites Where Button Batteries Get Lodged
Esophagus (Most dangerous - majority of severe injuries)
There are four natural areas of narrowing in the esophagus where foreign bodies get trapped:
| Site | Details |
|---|---|
| Cricopharyngeus muscle / Upper Esophageal Sphincter (UES) | At the level of the cricoid cartilage (~C6). Most common site in children due to their anatomical narrowing |
| Aortic arch level | At the level of T4, where the aorta crosses the esophagus |
| Left mainstem bronchus | Immediately below the aortic arch |
| Lower Esophageal Sphincter (LES) / Diaphragmatic hiatus | Most common site in adults |
When lodged in the esophagus, both poles make full mucosal contact - this is the anatomical key to why esophageal lodgment is so dangerous. Complications in the esophagus account for the vast majority of serious injuries; only 7% of significant injuries occur in the stomach and 1.3% in the small intestine.
Specific esophageal complication by location:
- Upper esophagus (posterior wall) - Tracheoesophageal fistula, tracheal necrosis, vertebral osteomyelitis/spondylodiscitis
- Mid esophagus (aortic arch level) - Aortoesophageal fistula (catastrophic, often fatal hemorrhage)
- In general - Esophageal perforation, mediastinitis, vocal cord palsy, stricture formation
Stomach
- Battery usually passes through but can be retained if large diameter (≥15-20 mm) in young children
- Less mucosal contact with both poles simultaneously, so injury risk is lower
- Can still cause ulceration and bleeding
Small Intestine
- Rare lodgment site (1.3% of serious injuries)
- Ileocecal valve is an anatomical narrowing where large batteries may arrest
Pylorus
- Functional narrowing where batteries ≥20 mm may not pass, especially in children under 6 years
Beyond the Colon
- Once past the ileocecal valve, passage is usually uneventful
Note: Button batteries also lodge in the nose and external auditory canal (not GI tract) causing septal ulceration/perforation, turbinate necrosis, and tympanic membrane perforation respectively.
- Rosen's Emergency Medicine, p. 1221
- Scott-Brown's Otorhinolaryngology (Vol 2), p. 434
3. GI Transit Times (Time Duration at Each Location)
| GI Segment | Normal Transit Time |
|---|---|
| Esophagus | Seconds (in healthy individuals) - but if lodged, it will NOT pass spontaneously without intervention |
| Stomach to pylorus | 30 minutes to several hours |
| Pylorus | May arrest here for batteries ≥15-20 mm; require 24h repeat imaging |
| Entire small intestine | ~3-6 hours (peristalsis-driven) |
| Overall intestinal transit (pylorus to rectum) | Average 3.8 days |
| Complete passage (mouth to stool) | Most batteries pass completely within 48-72 hours, though passage can take longer |
- Cummings Otolaryngology, Chapter on Esophagoscopy
- Tintinalli's Emergency Medicine, Chapter 77
Key caveat: If the battery has not passed the pylorus within 48 hours on repeat X-ray, this is clinically significant, especially in children under 6 years or with large (≥20 mm) batteries - intervention may be required.
4. Radiographic Identification
X-ray is the first-line imaging modality. The battery has a characteristic double contour / halo sign (step-off at the rim) on AP view that differentiates it from a coin.
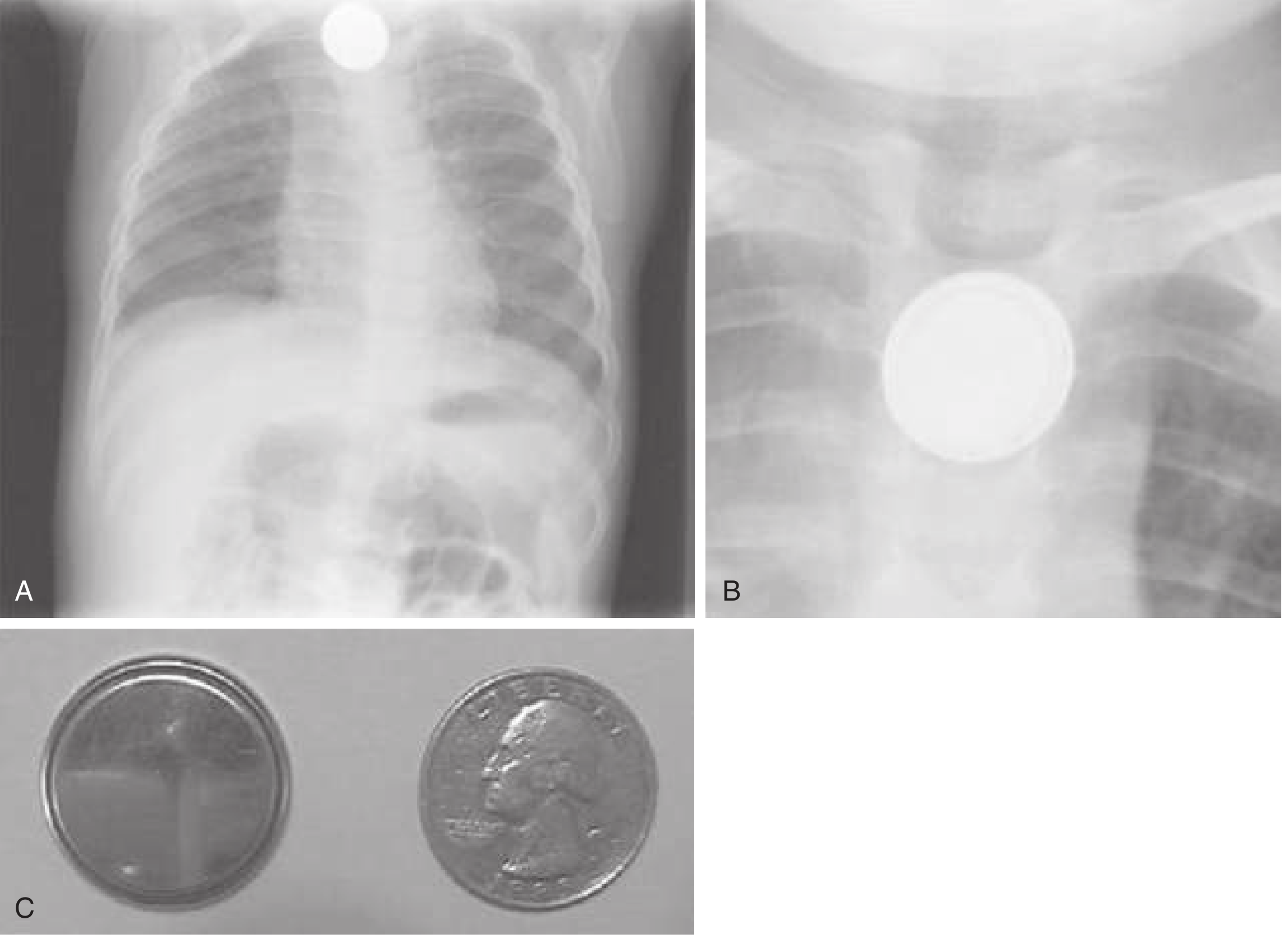
Fig. 75.2 - Coin vs Button Battery on Chest X-ray (Rosen's Emergency Medicine)
- The double contour/halo is the hallmark radiographic sign of a button battery
- On lateral view: the battery shows a step-off appearance
- CT (sensitivity 90-100%) is used when radiography is equivocal or when vascular complications are suspected
5. When Intervention IS Required (Indications)
EMERGENT - Immediate Removal (Goal: within 2 hours)
- Battery lodged in the esophagus - this is always an emergency, regardless of symptom status
- Any symptoms (dysphagia, drooling, vomiting, chest pain, respiratory distress)
- Battery in the stomach/beyond with magnet co-ingestion (risk of entrapment across bowel walls = pressure necrosis + perforation)
- Battery in stomach with the patient symptomatic at any age
URGENT Removal (within 24 hours)
Battery is in the stomach AND any of the following:
- Child is ≤5-6 years old (pylorus too small to pass ≥15 mm batteries reliably)
- Battery diameter is ≥15 mm
- Multiple batteries ingested
- Battery has been in stomach for >4 days without passage
- Battery previously thought to be in esophagus for >2 hours before reaching stomach (consider diagnostic endoscopy to exclude esophageal injury)
Surgical Removal
-
Battery has passed beyond the pylorus (out of endoscopic reach) AND the patient has:
- Occult or visible GI bleeding
- Abdominal pain / acute abdomen signs
- Fever, vomiting, profoundly decreased appetite
-
Rosen's Emergency Medicine, p. 1221
-
Tintinalli's Emergency Medicine (Algorithm Fig 77-3 below)
-
National Capital Poison Center guideline (poison.org)
6. When Intervention is NOT Required (Expectant Management / Observation)
Expectant management is acceptable only when ALL of the following are met:
- Battery has passed beyond the esophagus (confirmed radiographically)
- Patient is entirely asymptomatic and has been since ingestion
- Only one battery was ingested
- No magnet was co-ingested
- Battery diameter is < 12 mm (confirmed by imprint code or identical cell measurement)
- No prior esophageal surgery or anomaly
- Patient is >5-6 years old (adequate pyloric diameter)
Home management protocol for eligible patients:
- Regular diet, encourage activity
- Repeat X-rays at 48 hours to confirm pyloric passage
- Weekly repeat radiographs until confirmed passage in stool
- Return immediately if symptoms develop
- Stool inspection to confirm battery passage
7. Management Algorithm
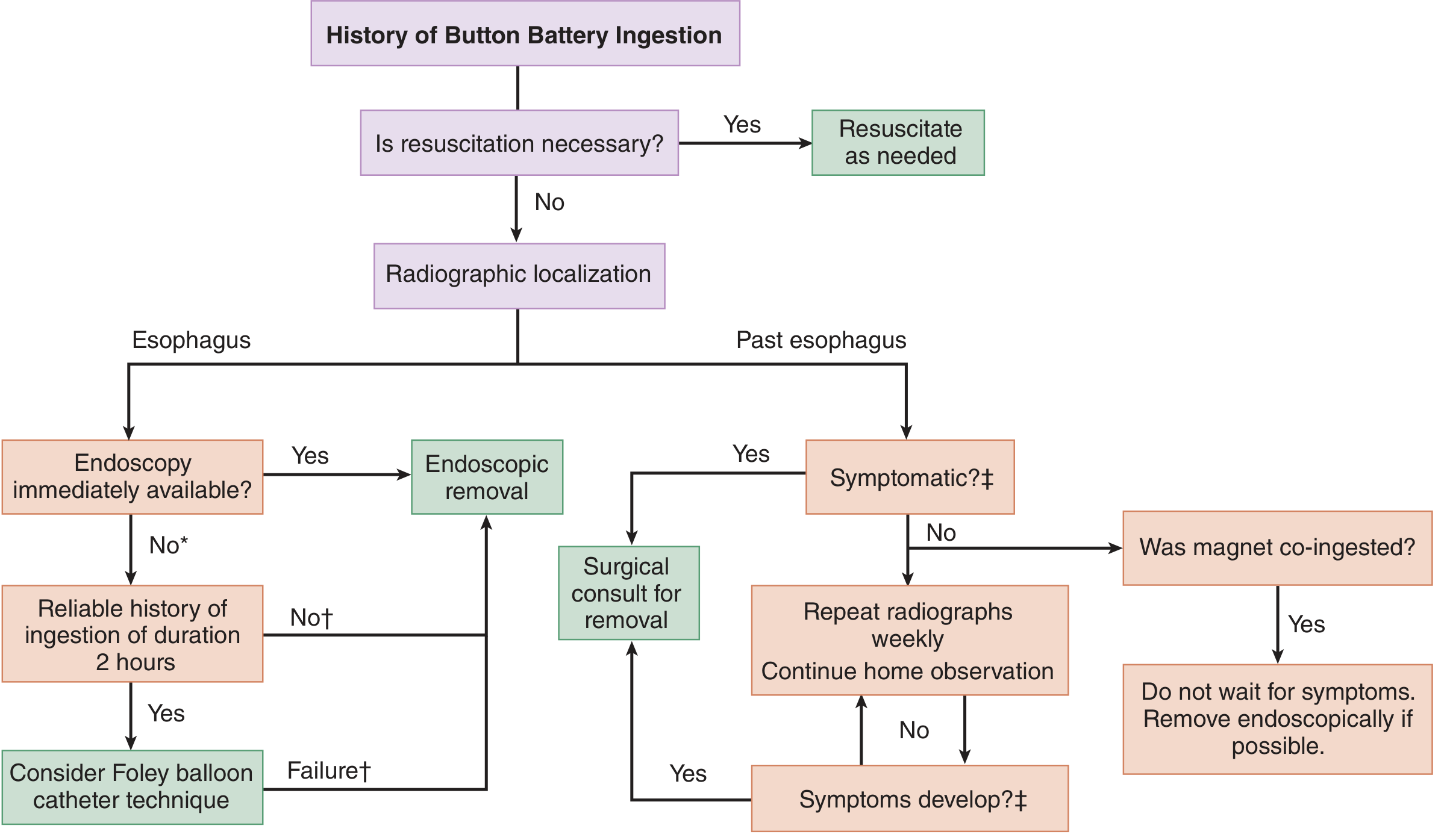
Figure 77-3 - Tintinalli's Emergency Medicine: Button Battery Ingestion Algorithm
8. First Aid / Pre-Endoscopy Measures
These apply to batteries confirmed or suspected in the esophagus, ingested within the last 12 hours:
- Honey: 10 mL every 10 minutes (up to 3 doses) for children ≥12 months - helps coat the battery and slow injury by coating the alkaline lesion
- Sucralfate suspension (1 g/10 mL): 10 mL PO every 10 minutes, up to 3 doses - similar protective mechanism to honey
- Do NOT give honey/sucralfate if ingestion was >12 hours ago (may mask perforation signs)
- These are adjuncts only - they do not replace emergent endoscopy
- Keep patient NPO otherwise
- Do NOT induce vomiting
- Do NOT give Ipecac, chelation, or perform blind bougienage
Post-removal irrigation: After endoscopic removal, if no perforation suspected, irrigate the injury site with 50-150 mL of 0.25% acetic acid to neutralize residual hydroxide ion accumulation.
9. Post-Removal Monitoring
Complications can progress even after battery removal due to ongoing necrosis:
- Repeat chest X-ray post-op to exclude pneumothorax (~0.8%) and pneumomediastinum
- Second-look endoscopy at 2-4 days post removal to assess mucosal injury grade and prognosis
- MRI chest on day 13-15 after removal for high-grade esophageal injuries to assess circumferential inflammation around the aorta/great vessels
- If MRI shows ≥50% circumferential inflammation around the aorta, CTA within 14-17 days post removal to assess aortoesophageal fistula risk
- Soft diet for a full 28 days after removal of esophageal battery
- Monitor for TE fistula: respiratory symptoms, especially with swallowing
- Serial contrast CT or MRI for patients at risk of vascular fistulization
10. Complications Summary
| Complication | Mechanism | Timing |
|---|---|---|
| Mucosal ulceration | Electrolysis + chemical burn | Within 15 min |
| Esophageal perforation | Deep necrosis | 2-6 hours |
| Aortoesophageal fistula | Necrosis eroding into aorta | Hours to weeks post-ingestion |
| Tracheoesophageal fistula | Anterior wall necrosis | Hours to weeks |
| Mediastinitis | Perforation with contamination | Hours to days |
| Vocal cord palsy | RLN compression/injury | Days |
| Spondylodiscitis | Posterior wall battery eroding to vertebra | Chronic / missed cases |
| Esophageal stricture | Fibrosis after healing | Weeks to months |
| Aspiration pneumonia | Tracheal involvement | Variable |
| Septal perforation (nasal) | Same mechanism in nasal FB | Hours to days |
11. Key Epidemiology and Risk Factors
- Children under 4 years are at highest risk (peak incidence 18-48 months)
- Males predominate (57%)
- The CR2032 (20 mm, 3V lithium coin cell) is the most dangerous and most commonly involved
- ~1/3 of patients present with dysphagia; ~1/5 are completely asymptomatic at presentation
- 54% of fatal cases were initially misdiagnosed - making early X-ray mandatory in any suspected ingestion
- 6.7-fold increase in battery ingestion incidents between 1985-2009 due to proliferation of small electronic devices
- National Button Battery Ingestion Hotline (USA): 1-202-625-3333 (poison.org)
12. Foreign Body Ingestion - General Clinical Principles
Four main patient groups at risk:
- Pediatric patients (>75% of cases)
- Psychiatric patients / prisoners (intentional)
- Patients with underlying esophageal disease (strictures, Schatzki ring, eosinophilic esophagitis)
- Edentulous adults (impaired oral sensation)
Objects that always require removal regardless of location:
- Button batteries (anywhere in GI tract if symptomatic or esophageal)
- Multiple magnets (attract across bowel loops - necrosis + fistula)
- Sharp/pointed objects in esophagus or symptomatic stomach
- Objects >6 cm in length or >2.5 cm in diameter (unable to pass pylorus)
- Any foreign body in esophagus >24 hours (high risk of complications including aorto-enteric fistula)
Objects that can generally be observed:
- Small smooth objects past the pylorus in asymptomatic patients
- Coins that have passed into the stomach in older children with normal anatomy
Contraindicated maneuvers:
- Blind finger sweeping (may lodge object in larynx)
- Proteolytic enzymes (Adolph's Meat Tenderizer) for food bolus - causes mucosal necrosis
- Chest physical therapy / bronchodilators for airway FB (may cause complete obstruction)
- Ipecac (no proven benefit, risk of esophageal injury)
Transit time reference for general foreign bodies (once past pylorus):
-
Small intestine: variable
-
Mean total intestinal transit: 3.8 days (Cummings Otolaryngology)
-
Most foreign bodies that reach the stomach will pass within 4-6 days
-
Rosen's Emergency Medicine, p. 1221
-
Cummings Otolaryngology, Chapter on Esophagoscopy
-
Tintinalli's Emergency Medicine, Chapter 77
-
Scott-Brown's Otorhinolaryngology Head and Neck Surgery (Vol 2), p. 434
This is a shared conversation. Sign in to Orris to start your own chat.