Holenstein lewis syndrome what's it mechanism signs and symptoms investigation and treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Searching the Web
Holenstein Lewis syndrome mechanism signs symptoms treatment
Searching PubMed
Holenstein Lewis syndrome
Reading Web Page
https://litfl.com/holstein-lewis-fracture
Finding Sources
Searching PubMed
Holstein Lewis humeral fracture radial nerve palsy
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
I now have comprehensive information and all diagrams. Here is the detailed, illustrated answer:
Holstein-Lewis Fracture
Note on terminology: "Holenstein-Lewis syndrome" is not a recognised entity in the medical literature. The correct eponym is the Holstein-Lewis fracture (named after Arthur Holstein and Gwilym B. Lewis), first described in their landmark 1963 paper in the Journal of Bone and Joint Surgery (JBJS 1963). The term "syndrome" is sometimes informally used because the fracture consistently comes with a characteristic nerve injury pattern.
Definition
The Holstein-Lewis fracture is a simple spiral fracture of the distal third of the humeral shaft, where the distal fragment displaces proximally and deviates toward the radial side. It is classically associated with a high rate of radial nerve palsy due to the nerve's anatomical vulnerability at precisely this point.
- Represents approximately 7% of all humeral shaft fractures
- Radial nerve palsy incidence: ~22% (vs. ~8-12% for humeral shaft fractures in general)
Anatomy - Why This Fracture Is Unique
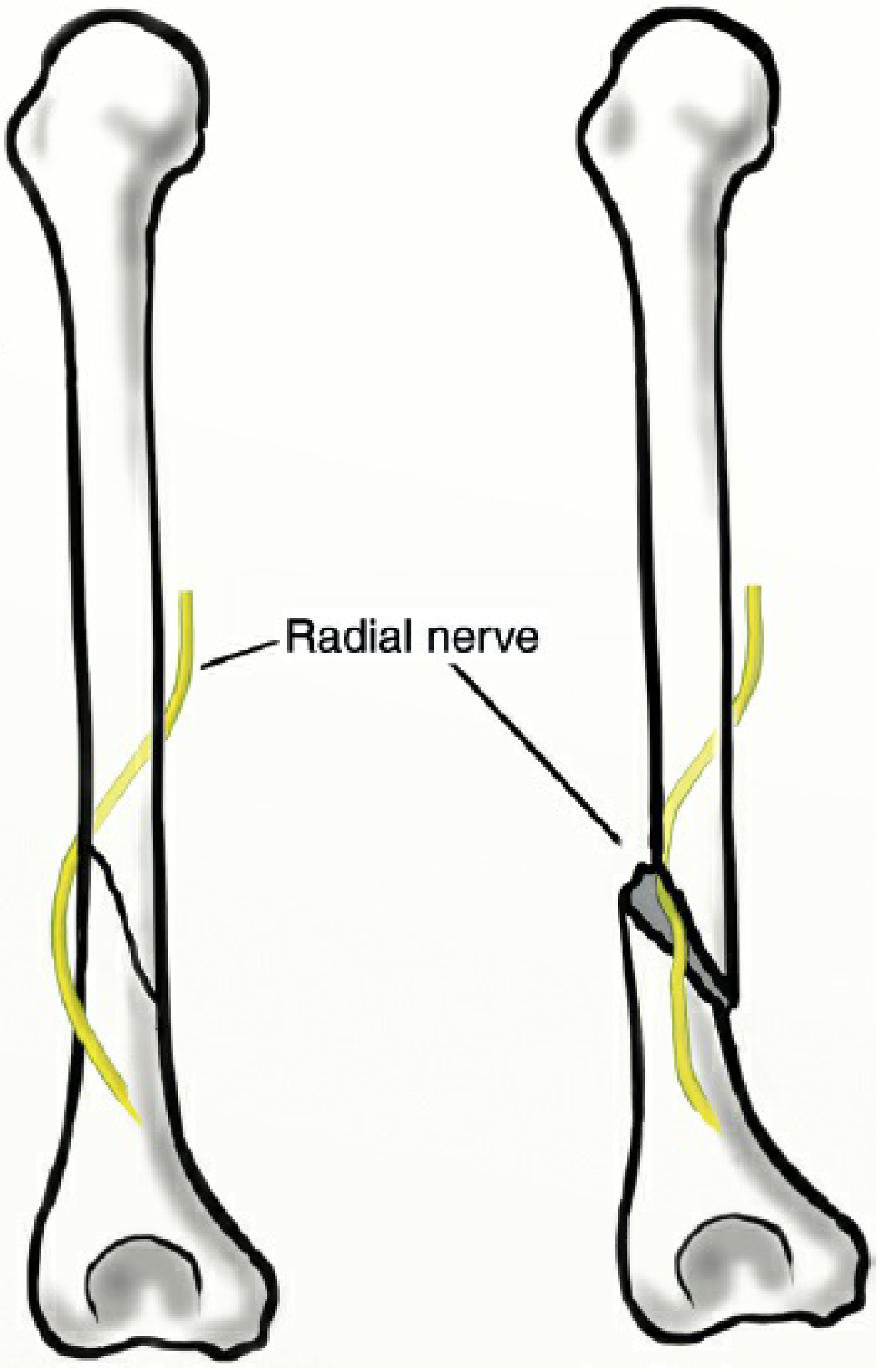
The radial nerve (C5-T1) travels in the spiral groove (radial groove) of the posterior humerus in the mid-shaft. As it reaches the distal third, it pierces the lateral intermuscular septum to transition from the posterior to the anterior compartment. At this precise point:
- The nerve lies directly against the periosteum of the bone
- It has minimal mobility - it is tethered by the lateral intermuscular septum
- It has no muscular protection
When a spiral fracture occurs at this level with lateral (radial) displacement of the distal fragment, the nerve cannot move away from the sharp fracture edge and is vulnerable to:
- Entrapment between fracture fragments
- Laceration by a sharp bone edge
- Stretch injury from fragment displacement
- Contusion/compression from haematoma
Mechanism of Injury

Common causes:
| Mechanism | Example |
|---|---|
| Direct blow | Fall onto the arm, road traffic accident |
| Torsional/indirect force | Arm-wrestling, throwing (sudden rotational force) |
| Fall on outstretched hand | Ground-level fall with torsion through the humerus |
| Pathological fracture | Underlying bone metastasis at the distal shaft |
The spiral pattern indicates a torsional force is the key biomechanical factor. The distal fragment spirals and displaces radially - the exact direction the radial nerve cannot escape.
Signs and Symptoms
1. Fracture Itself
- Acute pain in the upper arm, worst at the distal third
- Swelling and bruising over the lateral arm
- Deformity - arm appears shortened or angulated
- Crepitus on movement
- Inability to use the arm - arm held adducted, supported by the other hand
- Tenderness over the distal humeral shaft
2. Radial Nerve Palsy (the hallmark neurological complication)
The radial nerve supplies the extensors of the wrist, fingers, and thumb, plus sensation to the dorsoradial hand.
Motor signs:
| Finding | Muscle affected | Nerve branch |
|---|---|---|
| Wrist drop | Extensor carpi radialis longus/brevis | Radial nerve main |
| Finger drop | Extensor digitorum, extensor digiti minimi | Posterior interosseous nerve |
| Thumb drop | Extensor pollicis longus/brevis, abductor pollicis longus | Posterior interosseous nerve |
| Loss of elbow extension | Triceps (may be spared if injury distal) | Radial nerve (upper branch) |
Note: Triceps is often spared in Holstein-Lewis fractures because the branch to triceps arises proximal to the spiral groove. This is an important clinical pointer.
Sensory signs:
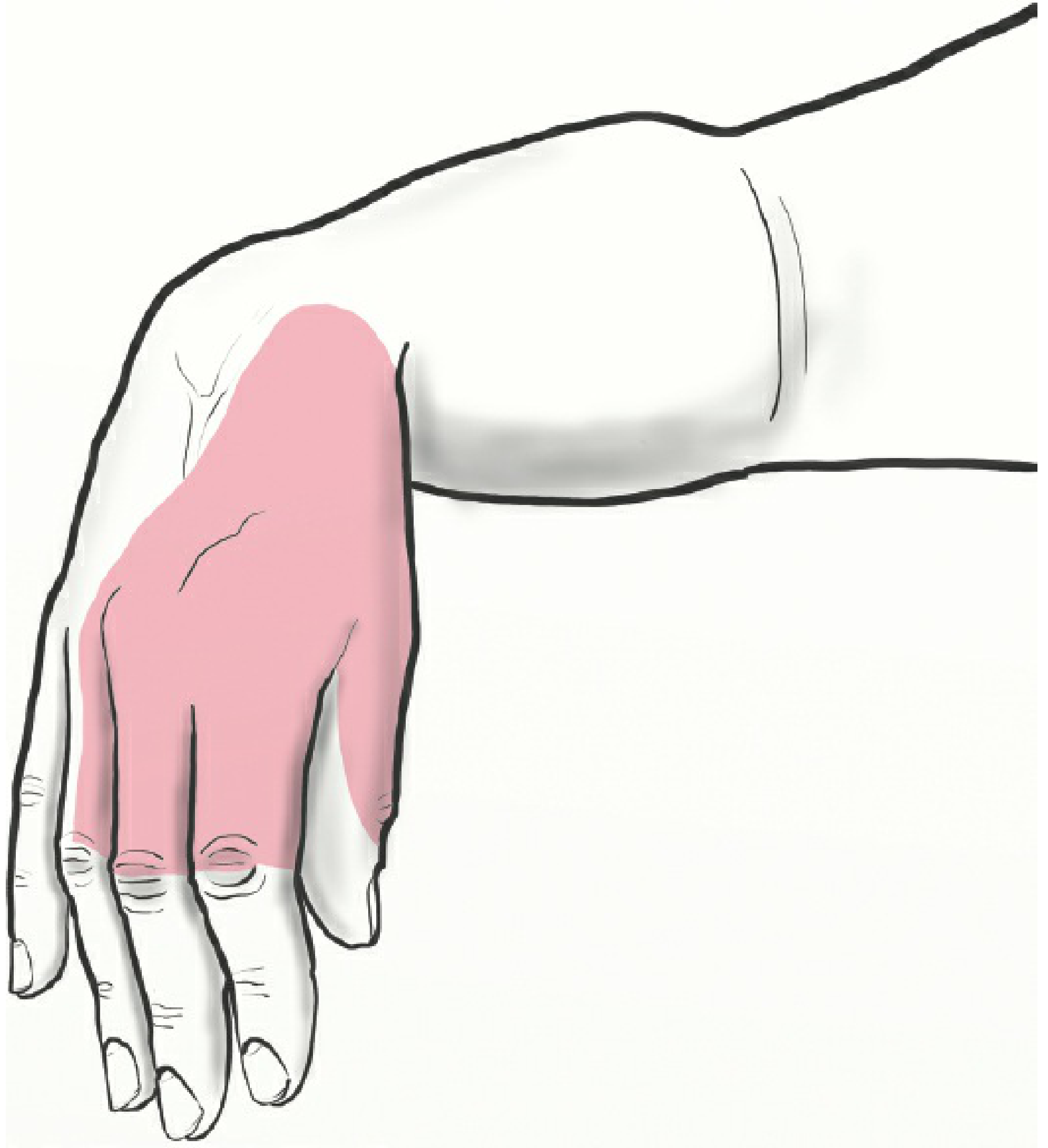
- Numbness / paraesthesia over the dorsum of the thumb, index, middle, and lateral half of the ring finger
- Dorsoradial wrist area sensory loss
- Sensory loss may be incomplete or subtle in neuropraxia
Types of Nerve Injury (Seddon Classification)
| Type | Description | Prognosis |
|---|---|---|
| Neuropraxia | Conduction block, axon intact | Full recovery in weeks-months |
| Axonotmesis | Axon disrupted, endoneurium intact | Recovery in months (most common type) |
| Neurotmesis | Complete nerve transection | Poor without surgery; requires repair/graft |
In Holstein-Lewis fractures, neuropraxia and axonotmesis account for the majority - spontaneous recovery occurs in 70-90% of cases with conservative management (Shao et al. 2005, Ekholm et al. 2008 [PMID 18978544]).
Investigations
1. Plain Radiography (First-line)
- AP and lateral X-ray of the humerus - gold standard for fracture diagnosis
- Shows: spiral fracture at distal 1/3 humerus with lateral/radial displacement of distal fragment
- Must also obtain: elbow and shoulder views to rule out associated fractures/dislocations
2. CT Scan
- Used when X-ray is inconclusive or to plan operative fixation
- Better delineates comminution, fragment position, and intra-articular extension
3. Neurological Assessment
- Thorough motor exam: wrist extension, finger extension, thumb extension, brachioradialis
- Sensory exam: dorsoradial hand, first web space
- Document neurological status before and after any manipulation
4. Electromyography (EMG) and Nerve Conduction Studies (NCS)
- Not done acutely - Wallerian degeneration takes 3 weeks to show on EMG
- Performed at ~3 months if no spontaneous recovery is occurring
- Assesses: site and severity of nerve injury, reinnervation potential
- Guides decision between continued observation vs. surgical exploration
5. Ultrasound of Radial Nerve
- Emerging role: can detect nerve entrapment within fracture gap
- Erra et al. used ultrasound in 35 patients to assess posterior interosseous nerve integrity
- Helps guide surgical decision-making in select cases
6. MRI (selective)
- If neurotmesis/laceration suspected and surgical planning needed
- Assesses nerve continuity and surrounding soft tissue injury
Treatment
Decision Framework
Holstein-Lewis Fracture
│
├─ Closed fracture?
│ │
│ ├─ YES: Conservative management preferred
│ │ + Expectant radial nerve management
│ │
│ └─ NO (open fracture, vascular injury,
│ polytrauma, failed conservative):
│ → ORIF + Nerve exploration
│
└─ Radial nerve palsy present?
│
├─ Closed injury → Expectant management
│ (70-90% spontaneous recovery)
│
└─ Open/sharp injury, progressive palsy,
no recovery at 3-6 months → Surgery
A. Non-Operative (Conservative) Treatment
Indications: Closed fracture, acceptable alignment, absent/expected-to-recover radial nerve palsy
Method:
- Coaptation splint / sugar-tong splint initially (first 1-2 weeks for pain/swelling)
- Functional brace (Sarmiento brace) applied at 1-2 weeks - the workhorse of treatment
- Prefabricated or custom-molded polyethylene brace
- Allows shoulder and elbow motion
- Brace maintained for average of 10 weeks
- Sarmiento (1990): 96% union rate in 85 distal 1/3 fractures
Acceptable alignment (functional bracing criteria):
- Varus/valgus angulation: <20°
- Anterior/posterior angulation: <20°
- Shortening: <3 cm
- Rotation: <15°
Radial nerve palsy - expectant management:
- Physiotherapy: maintain passive joint range of motion
- Dynamic wrist extension splint (cock-up splint) - prevents contracture, restores functional grip
- Serial clinical assessments every 4-6 weeks
- EMG at 3 months if no signs of recovery
- At 6 months without recovery: refer for nerve grafting ± tendon transfer consideration
B. Operative Treatment
Absolute indications for surgery:
- Open fracture
- Vascular injury requiring repair
- Ipsilateral forearm fracture ("floating elbow")
- Polytrauma / multiple injuries
- Inability to maintain fracture alignment conservatively
- Progressive radial nerve palsy (nerve being trapped by ongoing displacement)
Relative indications:
- Bilateral humeral fractures
- Pathological fracture
- Morbid obesity
Indications to explore radial nerve:
- Open fracture (sharp mechanism)
- Secondary radial nerve palsy (palsy developing after initial normal exam - suggests entrapment)
- No recovery at 3-6 months
- Operative fixation being performed anyway
Surgical options:
| Option | Approach | Notes |
|---|---|---|
| Plate fixation (ORIF) | Anterolateral or posterior | Gold standard; 4.5mm dynamic compression plate |
| Intramedullary nail (IMN) | Antegrade or retrograde | Minimally invasive; avoids nerve exploration |
| External fixation | Percutaneous | Temporary in polytrauma |
- Posterior approach: humerus is flat posteriorly; plate reaches further distally; direct radial nerve visualisation
- Anterolateral approach: allows nerve exploration; modified approach described specifically for Holstein-Lewis fractures
Nerve repair:
- If nerve in continuity during surgery: leave in anatomical position, protect, document relation to hardware
- If transected: primary repair (end-to-end neurorrhaphy) if tension-free; otherwise nerve grafting (sural nerve graft most common)
- At 6 months without recovery despite conservative care: nerve grafting ± tendon transfer (e.g., pronator teres to ECRB for wrist extension)
C. Adjuncts and Rehabilitation
- Pain management: NSAIDs, opioids short-term, neuropathic pain agents (pregabalin, gabapentin) for nerve pain
- Physiotherapy: Early shoulder mobilisation to prevent stiffness; progressive strengthening
- Smoking cessation: Optimises nerve and bone healing
- Glycaemic control in diabetics: Poor glycaemia impairs nerve regeneration
- Hand therapy: Dynamic splinting, oedema control, sensory re-education
Prognosis
| Outcome | Data |
|---|---|
| Fracture union (conservative) | ~96% (Sarmiento, 1990) |
| Radial nerve recovery (conservative) | 70-90% spontaneous |
| Average recovery time | 3-4 months (neuropraxia/axonotmesis) |
| High-energy injury nerve outcome | Poorer; high risk of neurotmesis |
Summary Table
| Feature | Detail |
|---|---|
| Type | Spiral fracture, distal 1/3 humerus |
| Key association | Radial nerve palsy (~22%) |
| Mechanism | Torsional force; nerve trapped at lateral intermuscular septum |
| Classic sign | Wrist drop + finger drop, spared triceps |
| Sensory loss | Dorsoradial hand, dorsal lateral 3.5 digits |
| First-line imaging | AP + lateral X-ray humerus |
| Nerve investigation | EMG/NCS at 3 months if no recovery |
| Conservative Rx | Functional brace (Sarmiento) 10 weeks + expectant nerve management |
| Surgical Rx | ORIF (plate) or IMN ± nerve exploration |
| Prognosis | Excellent in closed injuries; 70-90% nerve recovery |
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed. (2025) - Chapter 37, Nerve Injury
- Campbell's Operative Orthopaedics, 15th Ed. (2026) - Humeral Shaft section
- Holstein A, Lewis GB. Fractures of the humerus with radial nerve paralysis. J Bone Joint Surg Am. 1963;45:1382-1388 (PMID 14069777)
- Ekholm R et al. The Holstein-Lewis humeral shaft fracture. J Orthop Trauma. 2008 [PMID 18978544]
- LITFL Eponymictionary - Holstein-Lewis fracture
- AO Foundation - Radial Nerve Palsy Following Humeral Fractures
This is a shared conversation. Sign in to Orris to start your own chat.