Explain the mechanism of acute respiratory distress syndrome
Reading File
Finding Sources
Searching PubMed
"acute respiratory distress syndrome"[MeSH Terms] AND pathogenesis
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a thorough, well-sourced answer. Here is the complete explanation:
Mechanism of Acute Respiratory Distress Syndrome (ARDS)
ARDS is a syndrome of non-cardiogenic pulmonary edema caused by diffuse alveolar damage (DAD) from an overwhelming, dysregulated inflammatory response. It follows the Berlin definition: bilateral infiltrates on imaging, PaO2/FiO2 ratio <300 mmHg, onset within 7 days of a known insult, and edema not fully explained by cardiac failure or fluid overload. - Sabiston Textbook of Surgery, p. 940
1. Precipitating Causes (Direct vs. Indirect Lung Injury)
| Direct (pulmonary) | Indirect (extrapulmonary) |
|---|---|
| Pneumonia (most common) | Sepsis |
| Aspiration of gastric contents | Major trauma / hemorrhage |
| Inhalation injury | Severe pancreatitis |
| Pulmonary contusion | Massive transfusion (TRALI) |
| Near-drowning | Burns |
The common endpoint across all these triggers is excessive and dysregulated inflammation at the alveolar-capillary interface. - Murray & Nadel's Textbook of Respiratory Medicine, p. 3144
2. Phases of ARDS

Figure 312-1 from Harrison's Principles of Internal Medicine, 22E: Time course of ARDS phases.
Phase 1: Exudative Phase (Days 0-7)
This is the acute inflammatory phase and is the mechanistic core of ARDS.
Step 1 - Initial insult and pattern recognition
Microbial products (in sepsis/pneumonia) or tissue damage signals are recognized by resident alveolar macrophages and epithelial cells via pattern-recognition receptors (e.g., Toll-like receptors). This triggers release of pro-inflammatory cytokines - TNF-α, IL-1β, IL-6, IL-8 - and lipid mediators such as leukotriene B2. - Harrison's, p. 2652
Step 2 - Neutrophil sequestration and transmigration
One of the earliest manifestations (preceding hypoxemia) is transient leukopenia from neutrophil sequestration in the pulmonary microvasculature. Pulmonary capillaries are physically narrower than neutrophil diameter, forcing them to deform during transit. Activated neutrophils become "stiff" due to actin cytoskeletal rearrangement and cannot negotiate narrow capillary segments, causing trapping. IL-8 and other chemoattractants then drive their transmigration across the alveolar-capillary membrane into the interstitium and alveoli. - Murray & Nadel, p. 3147
Step 3 - Neutrophil-mediated tissue destruction
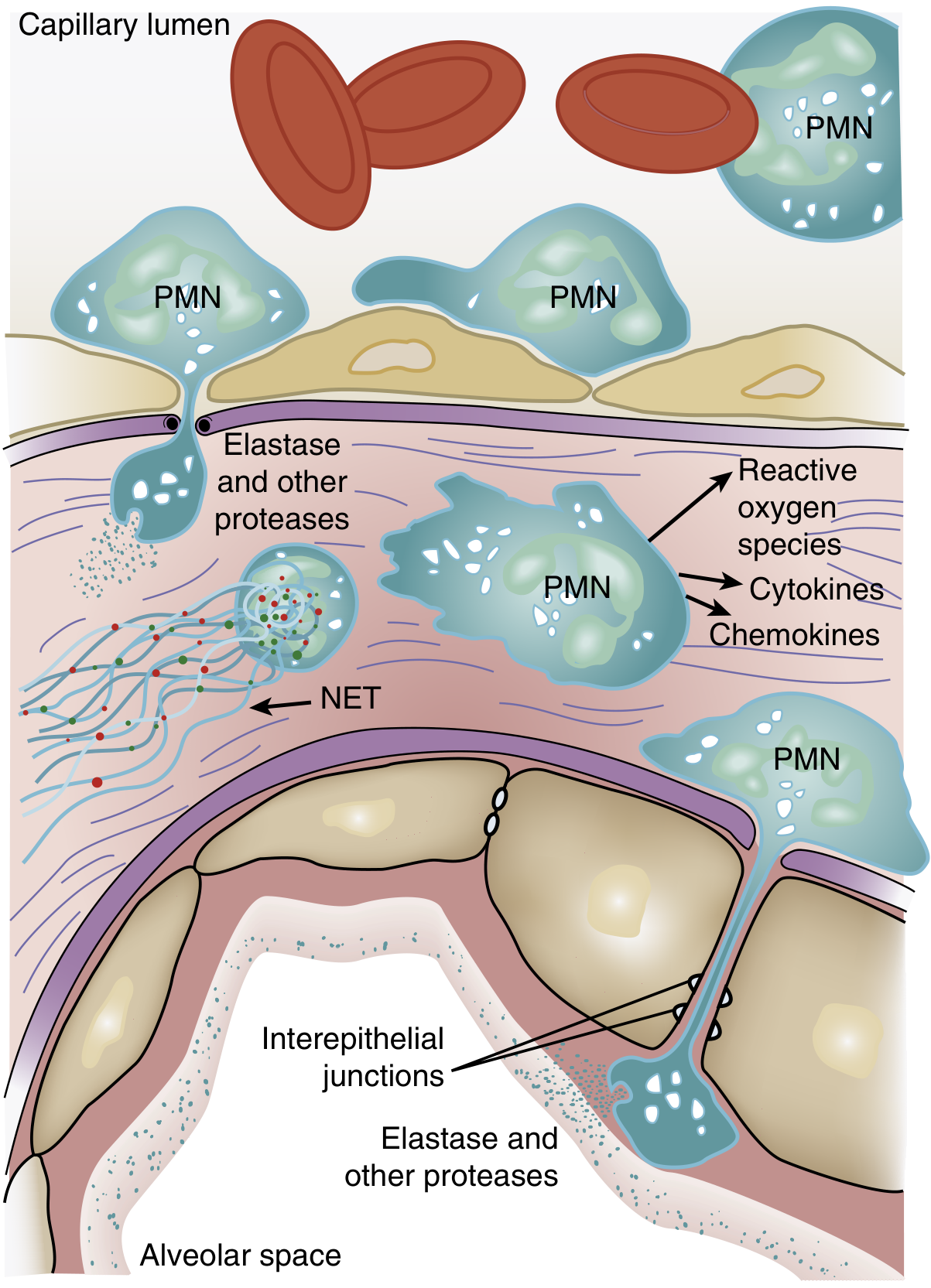
Figure 134.3 from Murray & Nadel: Neutrophil-mediated alveolar injury in ARDS.
During excessive and dysregulated inflammation, activated neutrophils release their microbicidal arsenal into the extracellular space:
- Neutrophil elastase - disrupts intercellular tight junctions and kills endothelial and epithelial cells; levels in bronchoalveolar lavage (BAL) fluid correlate with injury severity
- Matrix metalloproteinases (MMPs) - derived from both neutrophils and macrophages, degrade junctional proteins in endothelia and epithelia
- Reactive oxygen species (ROS) - oxidative injury to cell membranes and surfactant
- Cationic peptides (defensins) and other serine proteases - further extracellular matrix destruction
- Neutrophil extracellular traps (NETs) - chromatin-based webs that trap pathogens but also amplify sterile inflammation
- Murray & Nadel, pp. 187, 3147
Step 4 - Alveolar-capillary barrier breakdown
Injury to both the type I alveolar epithelial cells (95% of the alveolar surface) and the microvascular endothelium destroys the normally tight alveolar barrier. The dual-sided injury is the key event:
- Loss of endothelial barrier integrity allows plasma proteins and fluid to leak from the capillary into the interstitium
- Loss of epithelial barrier integrity allows this protein-rich fluid to flood the alveolar space
- Impaired alveolar fluid clearance (loss of ion transport via Na/K-ATPase on type II pneumocytes) prevents removal of edema fluid
- Murray & Nadel, p. 3146; Harrison's, p. 2652
Step 5 - Surfactant dysfunction
Type II pneumocytes are injured or killed, reducing synthesis and secretion of surfactant. Additionally, phospholipase A2 (from inflammatory cells and, in pancreatitis, from the pancreas itself) enzymatically degrades surfactant. Plasma proteins leaking into the alveolus further inhibit surfactant function. This causes:
- Increased alveolar surface tension
- Alveolar collapse (atelectasis), particularly in dependent lung regions
- Decreased lung compliance
- Murray & Nadel, pp. 3146-3147; Murray & Nadel (pancreatitis chapter), p. 2961
Step 6 - Hyaline membrane formation
Condensed plasma proteins aggregate with cellular debris and dysfunctional surfactant to form hyaline membrane whorls lining denuded alveolar surfaces - the pathologic hallmark of diffuse alveolar damage. - Harrison's, p. 2652
Step 7 - Vascular injury and pulmonary hypertension
Simultaneously, pulmonary vascular injury occurs with:
- Microthrombi formation and fibrocellular proliferation obliterating small vessels
- Loss of ventilated alveoli increases intrapulmonary shunting → refractory hypoxemia
- Microvascular occlusion reduces blood flow to still-ventilated alveoli → increased dead space and hypercapnia
- Together these mechanisms cause pulmonary hypertension and increase right heart afterload
- Harrison's, p. 2654
Phase 2: Proliferative Phase (Days 7-14)
- Neutrophil influx decreases; monocytes/macrophages become the dominant inflammatory cell
- Hyaline membranes begin to be reorganized
- Type II pneumocytes (the progenitor cell of the alveolar epithelium) proliferate to repopulate denuded surfaces
- Early interstitial inflammation and fibrosis begins; elevated N-terminal procollagen peptide III (a marker of collagen synthesis) is detectable in BAL fluid as early as 24 hours after onset - indicating that fibroproliferation may start simultaneously with the acute injury, not after it
- Pulmonary edema diminishes
- Most patients who recover do so during this phase
- Murray & Nadel, p. 3145; Harrison's, p. 2657
Phase 3: Fibrotic Phase (Day 21+)
- Occurs in a subset of patients with persistent ARDS (>2 weeks)
- Obliteration of pulmonary capillaries, deposition of interstitial and alveolar collagen
- Bullae formation, cystic changes
- Progressive respiratory failure from fibrosis, not edema
- Carries a substantially worse prognosis
- Murray & Nadel, pp. 3074-3075; Harrison's, Figure 312-1
3. Pathophysiologic Consequences
| Mechanism | Consequence |
|---|---|
| Flooded, collapsed alveoli (shunt) | Refractory hypoxemia (PaO2 does not respond to supplemental O2) |
| Increased alveolar dead space | Hypercapnia, increased work of breathing |
| Reduced surfactant, edematous lung | Decreased compliance, small functional residual capacity |
| Pulmonary vascular obliteration | Pulmonary hypertension, right heart strain |
| Dependent atelectasis | Heterogeneous injury - "baby lung" physiology |
The heavy, edematous ARDS lung behaves like a sponge: lesions are gravity-dependent, with a fluid-filled/consolidated dependent zone and a relatively spared non-dependent zone - this is the basis of prone positioning as therapy. - Goldman-Cecil Medicine, p. 1067
4. Why ARDS Can Occur Without Neutrophils
Importantly, ARDS can develop in profoundly neutropenic patients, confirming that neutrophils, while central, are not the only effectors. Monocytes, macrophages, platelets, complement activation, coagulation cascades, and endothelial cell apoptosis all contribute independently. - Murray & Nadel, p. 187
5. Summary Diagram of Pathogenesis
Precipitating insult (pulmonary or systemic)
↓
Alveolar macrophage + epithelial activation
↓
Cytokines (TNF-α, IL-1β, IL-6, IL-8), LTB2
↓
Neutrophil sequestration → transmigration
↓
Release of elastase, MMPs, ROS, NETs, defensins
↓
Type I pneumocyte + endothelial cell death
↓
Alveolar-capillary barrier breakdown
↓
Protein-rich edema floods alveoli → hyaline membranes
Surfactant dysfunction → alveolar collapse
Microvascular thrombosis → pulmonary hypertension
↓
Intrapulmonary shunt + dead space
↓
Refractory hypoxemia + hypercapnia = ARDS
Key sources:
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter 134 (ARDS) and Chapter 8 (Lung Injury)
- Harrison's Principles of Internal Medicine, 22E, Chapter 312
- Goldman-Cecil Medicine, Chapter 91 (Mechanical Ventilation in ARDS)
- Sabiston Textbook of Surgery, 11E
This is a shared conversation. Sign in to Orris to start your own chat.