
photo-1783866434583.jpg
Answer the question
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material from the textbooks. Here is the full, detailed answer to the question:
Functional Divisions of the Cerebellum [2+3+3+4]
1. Functional Divisions [2 marks]
Functionally, the cerebellum is divided into 3 parts based on its input/output connections:
| Functional Division | Anatomical Basis | Other Name |
|---|---|---|
| Vestibulocerebellum | Flocculonodular lobe | Archicerebellum |
| Spinocerebellum | Vermis + Intermediate hemispheres | Paleocerebellum |
| Cerebrocerebellum (Pontocerebellum) | Lateral hemispheres | Neocerebellum |
2. Connections (Afferent and Efferent) [3 marks]
Connections are carried via the three cerebellar peduncles:
Afferent (Input) Pathways
| Peduncle | Afferent Pathway | Fiber Type |
|---|---|---|
| Superior | Ventral spinocerebellar tract; tectocerebellar tract | Mossy fibers |
| Middle (Brachium pontis) | Pontocerebellar fibers (from cerebral cortex via pons) | Mossy fibers |
| Inferior (Restiform body) | Dorsal spinocerebellar + cuneospinocerebellar tracts; vestibular fibers; climbing fibers from contralateral inferior olive | Mossy + Climbing fibers |
Summary by division:
- Vestibulocerebellum: Receives input from vestibular nuclei (via inferior peduncle)
- Spinocerebellum: Receives input from spinal cord (spinocerebellar tracts)
- Cerebrocerebellum: Receives input from cerebral cortex via corticopontine fibers (via middle peduncle)
Efferent (Output) Pathways
All outputs leave via the superior cerebellar peduncle (except fastigial nucleus outputs):
| Division | Deep Nucleus | Efferent Pathway |
|---|---|---|
| Vestibulocerebellum | Lateral vestibular nucleus (Deiters) | Vestibulospinal tract |
| Spinocerebellum (vermis) | Fastigial nucleus | Vestibulospinal + reticulospinal tracts |
| Spinocerebellum (intermediate) | Interposed (globose + emboliform) | Contralateral red nucleus → rubrospinal tract |
| Cerebrocerebellum | Dentate nucleus | Contralateral VL/VA thalamus → motor cortex |
Key circuit: Cerebellar nuclei → superior cerebellar peduncle → decussates at level of inferior colliculus → ventrolateral thalamus → motor cortex. Since this pathway crosses twice (cerebellar output and corticospinal), a cerebellar lesion causes ipsilateral signs.
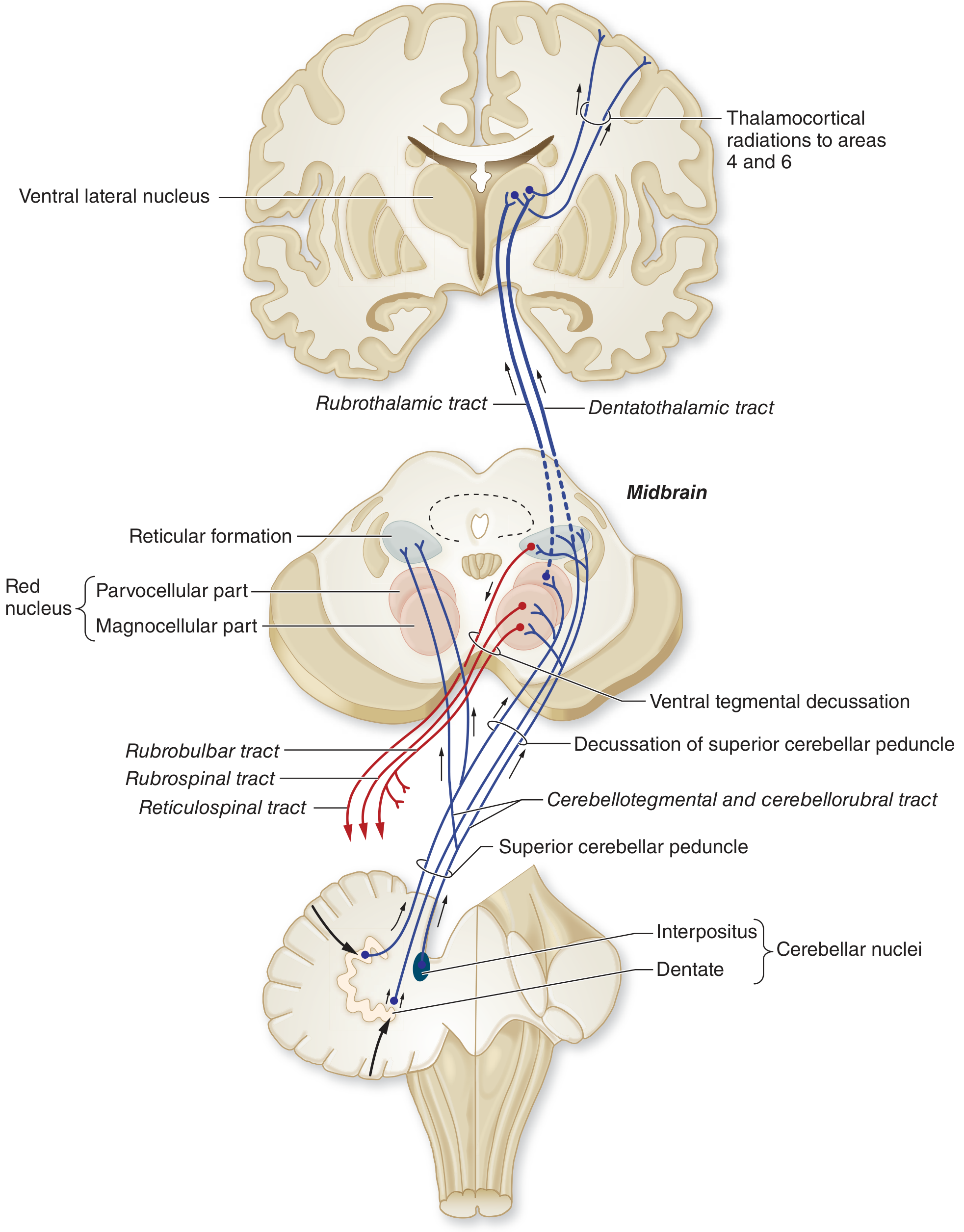
Cerebellar efferent connections - ascending tracts in blue, descending in red. All efferent fibers exit via the superior cerebellar peduncle.
3. Functions of the Cerebellum [3 marks]
- Coordination of voluntary movements - smoothing and fine-tuning of motor activity; prevents errors in range, force, and direction of movement
- Maintenance of equilibrium and posture - via vestibulocerebellum; regulates muscle tone against gravity
- Motor planning and procedural memory - lateral hemispheres involved in planning motor programs for extremities and learning motor sequences
- Regulation of muscle tone - via connections to gamma motor neurons; lesions cause hypotonia
- Coordination of eye movements - flocculonodular lobe controls vestibulo-ocular reflex and smooth pursuit
- Synergy of muscle groups - ensures appropriate co-contraction and sequencing of agonist/antagonist muscle groups
- Non-motor functions - some evidence for roles in cognitive processing and language via dentate-thalamo-cortical connections
4. Clinical Manifestations Following Cerebellar Lesion [4 marks]
The classic mnemonic DANISH covers the main signs:
A. Dysmetria
- Inability to accurately gauge distance/direction of movement
- Demonstrated by finger-nose test (past-pointing) and heel-knee-shin test
- Overshoot = hypermetria; undershoot = hypometria
B. Ataxia
- Gait ataxia: Wide-based, reeling, drunken gait; patient tends to fall toward the side of the lesion
- Truncal ataxia: With vermis lesions - inability to sit or stand steadily (titubation - tremor of the trunk/head)
- Appendicular ataxia: Incoordination of limb movements (lateral hemisphere lesions)
C. Nystagmus
- Gaze-evoked nystagmus is most common; may be multidirectional (unlike peripheral vestibular nystagmus)
- Ocular dysmetria - saccades overshoot/undershoot targets
- Flocculonodular lesions cause jerky saccadic intrusions during smooth pursuit
D. Intention Tremor (Action Tremor)
- Tremor that appears or worsens as the limb approaches its target
- Absent at rest; worsens on movement (opposite of Parkinson's resting tremor)
- Due to loss of smooth cerebellar braking of movement
E. Dysarthria (Scanning speech)
- Slurred, irregular, explosive speech
- Loss of coordination of muscles of articulation
- Speech has irregular cadence - "scanning" or "staccato" quality
F. Dysdiadochokinesis
- Inability to perform rapid alternating movements (e.g., pronation/supination of hand)
- Tested by rapid alternating hand tapping
Additional Signs:
- Hypotonia: Decreased resistance to passive movement; pendular reflexes on tendon testing
- Rebound phenomenon (loss of check): When resistance to a movement is suddenly released, the limb overshoots
- Decomposition of movement: Complex movements break down into component parts
- Romberg test: Negative (Romberg positive suggests sensory/proprioceptive ataxia, NOT cerebellar)
Lateralization Rule:
Cerebellar hemisphere lesions produce ipsilateral signs because of the double decussation in the pathway (cerebellar output crosses to contralateral thalamus/cortex, but corticospinal tract crosses again at medulla).
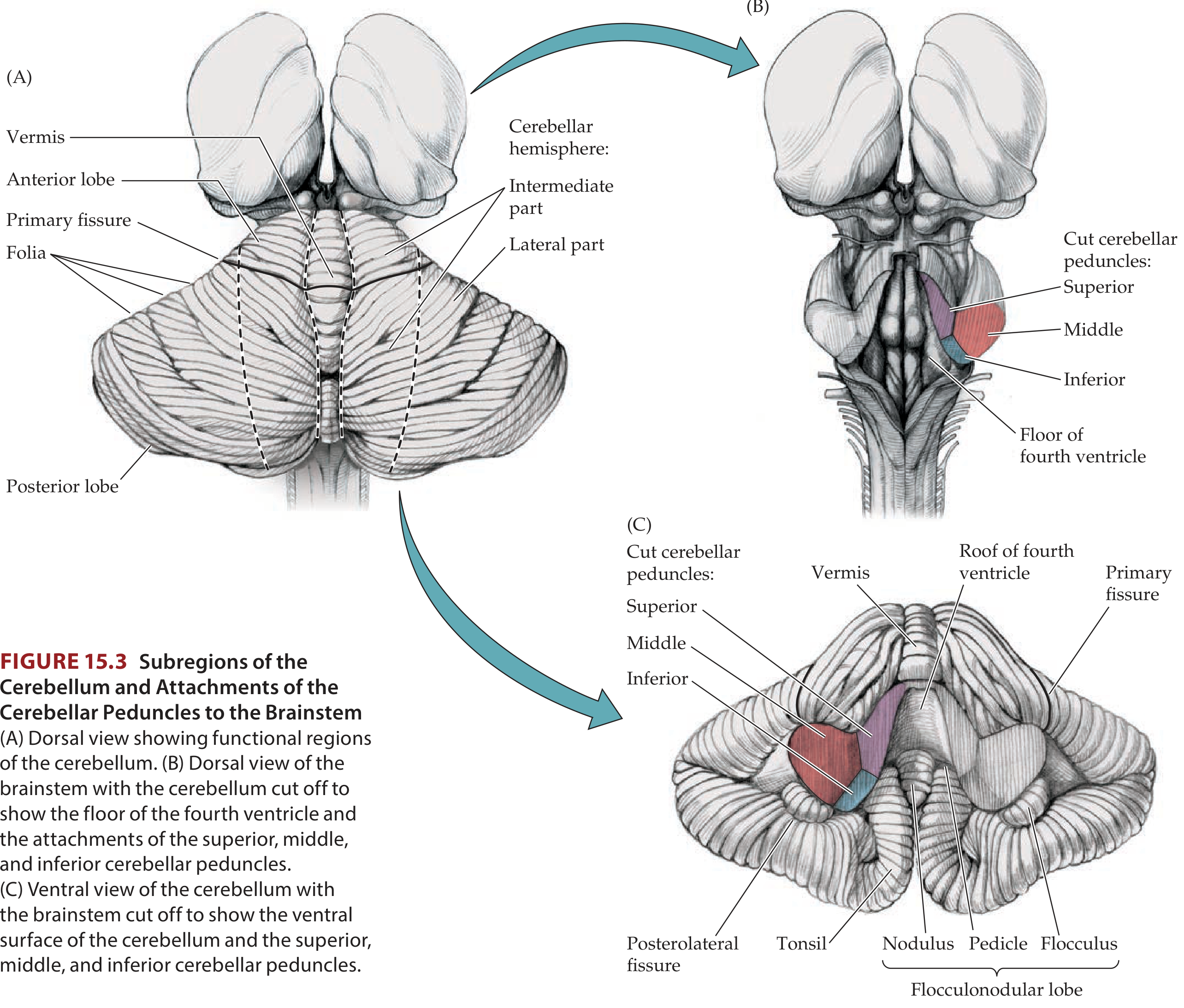
Subregions of the cerebellum. (A) Dorsal view showing functional regions. (C) Ventral view showing the flocculonodular lobe (vestibulocerebellum).
Sources: Adams and Victor's Principles of Neurology, 12th Ed., p. 122-126; Neuroanatomy through Clinical Cases, 3rd Ed., p. 728
This is a shared conversation. Sign in to Orris to start your own chat.