Monteral sign
Reading File
Searching the Web
Montreal sign clinical medicine orthopedics
Finding Sources
Searching the Web
"Montreal sign" medical clinical examination coracoid
Finding Sources
Searching the Web
"Montreal sign" neurology dementia cognitive assessment MoCA
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information. You likely meant the Montreal Cognitive Assessment (MoCA), commonly called the "Montreal sign/test" in clinical shorthand. Here is a full overview:
Montreal Cognitive Assessment (MoCA)
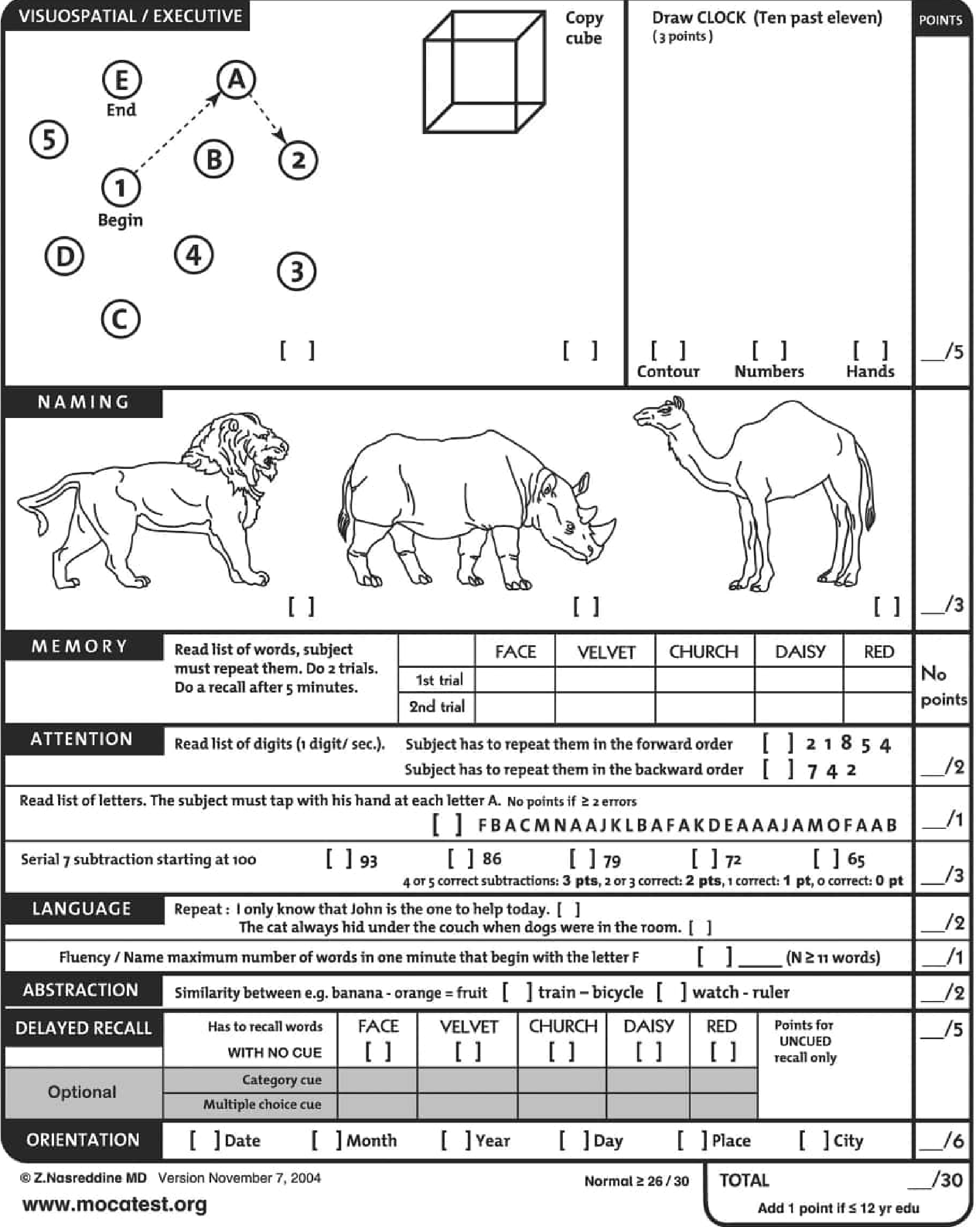
The Montreal Cognitive Assessment (MoCA) is a brief, standardized 30-point cognitive screening tool developed by Dr. Ziad Nasreddine in 1995 (published 2005) to detect mild cognitive impairment (MCI) and early dementia in clinical settings.
Key Features
| Feature | Detail |
|---|---|
| Total score | 30 points |
| Administration time | ~10 minutes |
| Normal cutoff | ≥ 26/30 (original); education-adjusted norms now preferred |
| Education adjustment | +1 point if ≤ 12 years of formal education |
| Languages available | 30+ languages and dialects |
Domains Tested (7 domains)
- Visuospatial/Executive (5 pts) - Trail-making (alternating numbers/letters), cube copy, clock drawing (time: ten past eleven)
- Naming (3 pts) - Identify drawings of a lion, rhinoceros, and camel
- Memory (no immediate points) - Read 5 words (FACE, VELVET, CHURCH, DAISY, RED); two learning trials; delayed recall tested later
- Attention (6 pts) - Forward and backward digit span, letter tapping (tap at letter "A"), serial 7 subtractions from 100
- Language (3 pts) - Sentence repetition x2, verbal fluency (words beginning with "F" in 1 minute, ≥11 = 1 pt)
- Abstraction (2 pts) - Similarities (train-bicycle, watch-ruler)
- Delayed Recall (5 pts) - Free recall of 5 words after 5 minutes; optional category/multiple choice cues (no points for cued recall)
- Orientation (6 pts) - Date, month, year, day, place, city
Scoring Interpretation
- 26-30: Normal
- 18-25: Mild cognitive impairment (MCI)
- 10-17: Moderate impairment
- < 10: Severe impairment
Scores are influenced by age and education, so population-adjusted normative tables (Table 44.5 in Bradley & Daroff) should be used rather than a single universal cutoff.
Clinical Uses
The MoCA has been validated as a sensitive screener in:
- Alzheimer disease and other dementias
- Vascular dementia after acute stroke
- Parkinson disease (more sensitive than MMSE for executive/frontal dysfunction)
- Huntington disease
- Post-stroke cognitive impairment
- Brain metastases
It is more sensitive than the MMSE for detecting executive dysfunction (frontal lobe) and MCI, because it includes harder tasks (trail-making, abstraction, serial 7s).
MoCA vs. MMSE
| Feature | MoCA | MMSE |
|---|---|---|
| Executive function | Yes (Trail-making, abstraction) | Minimal |
| Sensitivity for MCI | Higher (~94% for dementia) | Lower |
| False positives | ~40% of healthy individuals score <26 | Less |
| Cost | Free (mocatest.org) | Now copyrighted/fee |
| Difficulty | More difficult | Easier |
Important Caveats
- The MoCA should not be used as a standalone diagnostic tool. It is a screening instrument to flag the need for formal neuropsychological testing.
- Reliability is lower in non-clinical (healthy) populations - it should primarily be used in patients with suspected cognitive impairment.
- The original cut score of 26 was developed without fully accounting for age, education, or cultural variables.
- As per the U.S. Affordable Care Act (2010), an annual cognitive assessment is suggested for all Medicare patients.
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, p. 893-895 (Section: Montreal Cognitive Assessment)
- Nasreddine et al., J Am Geriatr Soc. 2005;53:695-699 (original validation paper)
- mocatest.org - official resource with all language versions
This is a shared conversation. Sign in to Orris to start your own chat.