HIV/AIDS
Reading File
Finding Sources
Finding Sources
Searching PubMed
"HIV" AND "antiretroviral therapy"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, image-rich answer. Let me compile it.
HIV / AIDS
Overview
Human Immunodeficiency Virus (HIV) is a lentivirus (family Retroviridae) that selectively destroys CD4+ T lymphocytes, progressively dismantling cell-mediated immunity until the host can no longer defend against organisms that are harmless to immunocompetent individuals. This end stage is Acquired Immune Deficiency Syndrome (AIDS).
As of 2022, approximately 39 million people worldwide live with HIV, and it caused ~630,000 deaths that year. About 67% of all cases are in Sub-Saharan Africa. With modern antiretroviral therapy (ART), life expectancy in treated patients now approaches that of the general population.
- Harrison's Principles of Internal Medicine 22E, p. 1015
The Virus
HIV-1 (the predominant global strain) and HIV-2 (largely confined to West Africa) are enveloped RNA retroviruses. Key structural components:
| Component | Function |
|---|---|
| gp120 | Binds CD4 receptor + CCR5/CXCR4 co-receptor on target cells |
| gp41 | Mediates membrane fusion |
| Reverse transcriptase (RT) | Converts viral RNA → DNA (error-prone, generating mutations) |
| Integrase | Inserts viral DNA into host genome (provirus) |
| Protease | Cleaves viral polyproteins for maturation |
| Capsid (p24) | Core structural protein; key antigen for early diagnosis |
HIV targets cells expressing CD4: predominantly CD4+ helper T cells, macrophages, dendritic cells, and microglial cells of the brain.
Pathogenesis
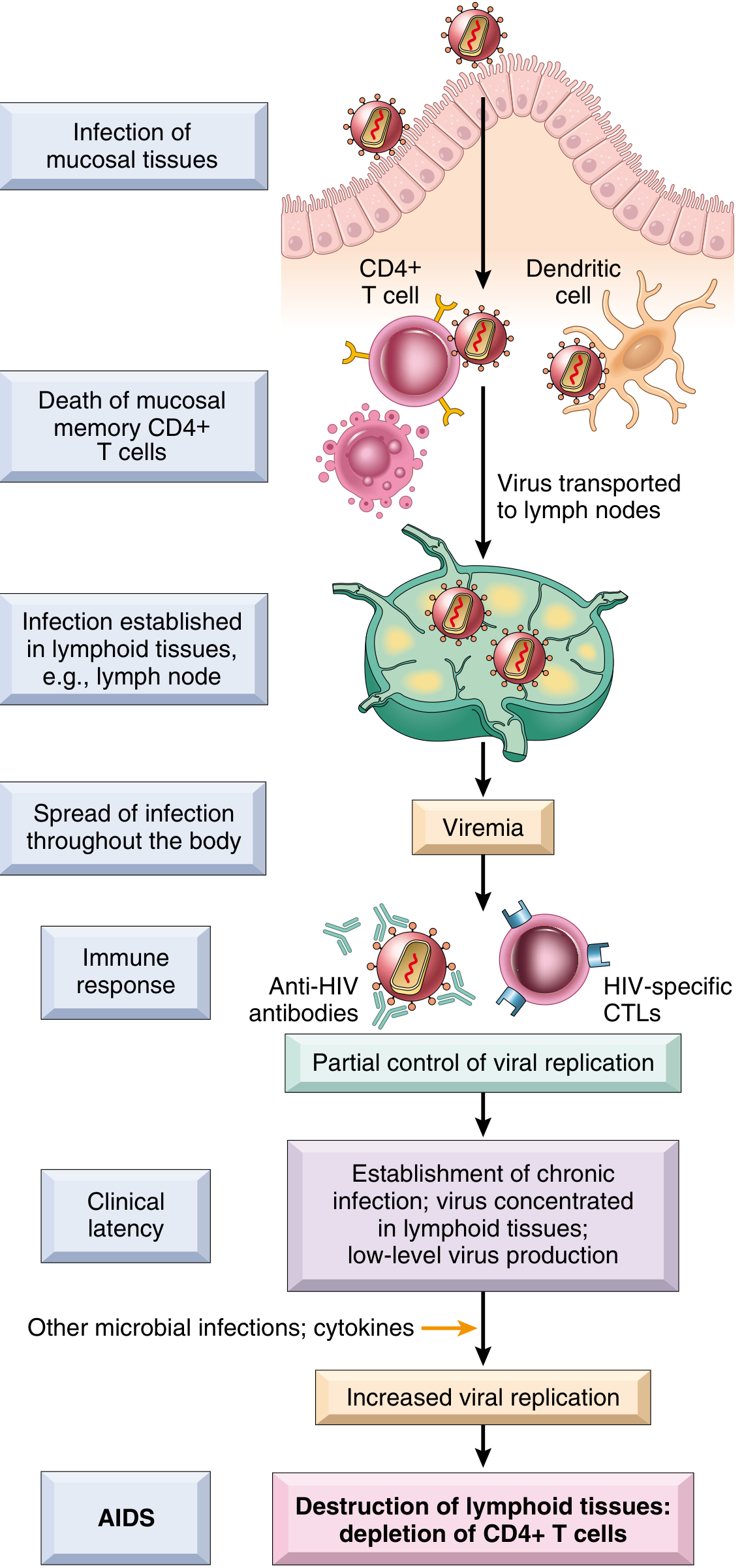
Entry and early infection:
- HIV gains entry via mucosal surfaces (genital, rectal, oral) or direct bloodstream inoculation
- gp120 binds CD4 and a co-receptor (CCR5 on macrophages/memory T cells; CXCR4 on naive T cells)
- Dendritic cells at the mucosa capture virus and transport it to regional lymph nodes
- Massive destruction of memory CD4+ T cells occurs in mucosal lymphoid tissue within days - this is the largest reservoir of memory T cells in the body
Mechanisms of CD4+ T cell depletion:
- Direct lytic infection - virus replication kills infected cells
- Activation-induced cell death (apoptosis) - chronic activation of uninfected bystander cells
- Pyroptosis - abortive HIV infection activates the inflammasome, triggering inflammatory cell death and recruiting more susceptible cells
- Syncytium formation - gp120 on infected cells binds CD4 on uninfected cells, causing fusion and death (T-tropic X4 HIV-1)
- Lymphoid tissue destruction - progressive damage to lymph node architecture
- Reduced thymic output - infection of progenitor cells reduces CD4+ T cell production
Robbins Pathologic Basis of Disease, pp. 961-975
Viral latency: Integrated provirus can persist silently for months to years in long-lived memory CD4+ T cells and follicular helper T cells in germinal centers (where CD8+ CTLs are excluded). Even with undetectable plasma viremia on ART, latent virus persists in ~0.05% of CD4+ cells in lymph nodes - the so-called "viral reservoir," the principal obstacle to cure.
Clinical Stages and Natural History
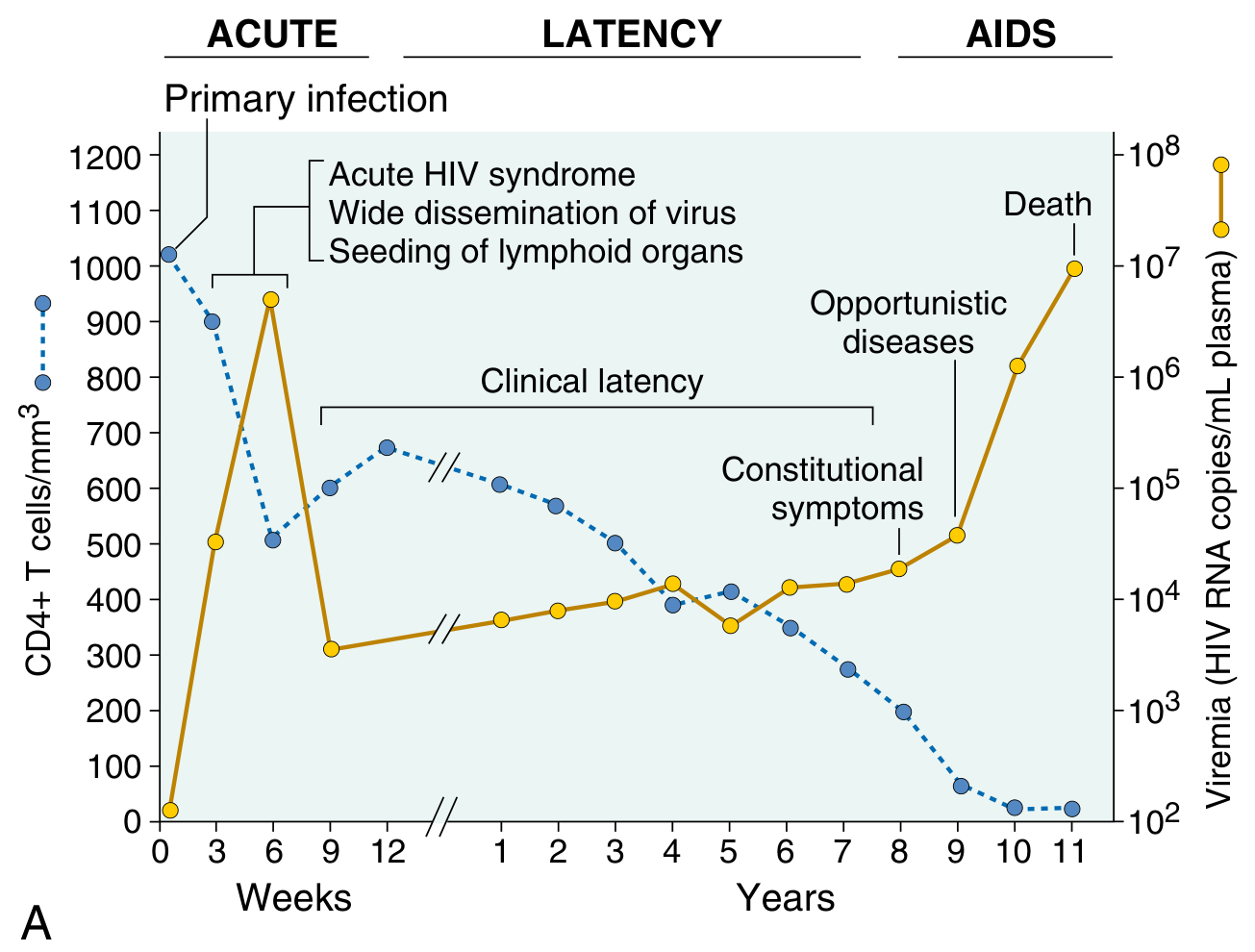
Stage 1 - Acute HIV Syndrome (weeks 2-4)
- Occurs in ~50-70% of newly infected individuals
- Resembles infectious mononucleosis: fever, lymphadenopathy, pharyngitis, rash, myalgias, headache
- Extremely high viremia (>10^6 copies/mL), with sharp transient drop in CD4 count
- Host mounts CTL and humoral response, partially controlling viremia
Stage 2 - Clinical Latency (months to ~10 years)
- Patient is often asymptomatic
- Viral replication continues at low level; CD4+ count falls gradually (~50-100 cells/μL per year)
- Generalized lymphadenopathy may occur
- Patient remains infectious throughout
Stage 3 - AIDS
Defined by the CDC as:
- CD4+ count <200 cells/μL (in adults/adolescents ≥6 years), OR
- Presence of an AIDS-defining opportunistic illness (Stage C)
Harrison's Principles of Internal Medicine 22E, p. 462
CDC Classification
| Stage | CD4 Count (cells/μL) | Clinical Category |
|---|---|---|
| 1 | ≥500 | A: Asymptomatic, acute HIV, persistent lymphadenopathy |
| 2 | 200-499 | B: Symptomatic, not A or C conditions |
| 3 (AIDS) | <200 | C: AIDS-defining illness (Table below) |
AIDS-Defining Opportunistic Illnesses
Infections
| Category | Examples |
|---|---|
| Protozoal | Pneumocystis jirovecii pneumonia (PCP), Toxoplasmosis (CNS), Cryptosporidiosis (>1 month), Isosporiasis |
| Fungal | Esophageal/pulmonary Candidiasis, Cryptococcal meningitis, Disseminated Histoplasmosis, Coccidioidomycosis |
| Bacterial | Disseminated MAC (M. avium-intracellulare), M. tuberculosis (any site), Recurrent Salmonella septicemia |
| Viral | CMV retinitis/colitis/encephalitis, Chronic HSV ulcers (>1 month), Progressive multifocal leukoencephalopathy (PML, JC virus) |
Neoplasms
- Kaposi's sarcoma (HHV-8 driven; violaceous skin/mucosal lesions)
- Primary CNS lymphoma
- Burkitt's/immunoblastic lymphoma
- Invasive cervical cancer
Key clinical pearls:
- Oral candidiasis in an HIV+ patient signals immune decompensation and often heralds the transition to AIDS
- CMV retinitis occurs almost exclusively when CD4 <50 cells/μL
- MAC infection is a late complication (CD4 <50); TB can occur much earlier
- Worldwide, ~1/3 of AIDS deaths are attributable to tuberculosis
Robbins Pathologic Basis of Disease, pp. 1091-1097
Abnormalities of Immune Function in AIDS
| Domain | Defects |
|---|---|
| T cells | Lymphopenia; loss of activated/memory T cells; decreased DTH; reduced proliferative response; decreased cytotoxicity |
| B cells | Hypergammaglobulinemia (polyclonal); decreased antibody response to new antigens |
| NK cells | Decreased lytic activity |
| Monocytes/Macrophages | Decreased chemotaxis; decreased bacterial killing; impaired antigen presentation |
Robbins, Table 6.14
Diagnosis
| Test | Role |
|---|---|
| 4th-generation HIV Ag/Ab combo test | Initial screening; detects p24 antigen + anti-HIV antibodies (window ~18 days) |
| HIV-1/HIV-2 differentiation assay | Confirms reactive screen; distinguishes types |
| HIV RNA (viral load, PCR) | Quantifies replication; used for monitoring treatment |
| CD4+ T cell count | Gauges immune status; determines prophylaxis thresholds |
| Resistance genotyping | Before initiating or switching ART |
Blood turns positive for HIV antibodies within 2 to 18 months of infection. The "window period" for modern 4th-generation tests is approximately 18-45 days.
Antiretroviral Therapy (ART)
ART is the cornerstone of management and should be initiated as soon as possible after diagnosis. ART transformed HIV from a fatal disease into a manageable chronic condition. By 2022, 76% of people living with HIV globally were receiving ART.
Drug Classes
| Class | Mechanism | Examples |
|---|---|---|
| NRTIs (nucleoside/nucleotide reverse transcriptase inhibitors) | Competitive inhibition + chain termination of RT | Tenofovir (TDF/TAF), Emtricitabine (FTC), Lamivudine (3TC), Abacavir (ABC) |
| NNRTIs (non-nucleoside RT inhibitors) | Non-competitive binding to RT, allosteric inhibition | Efavirenz, Rilpivirine, Doravirine |
| PIs (protease inhibitors) | Block viral protease, preventing polyprotein cleavage | Darunavir, Atazanavir (boosted with ritonavir or cobicistat) |
| INSTIs (integrase strand transfer inhibitors) | Block insertion of viral DNA into host genome | Dolutegravir, Bictegravir, Raltegravir, Cabotegravir |
| Entry inhibitors | Block CCR5 (maraviroc), gp41 fusion (enfuvirtide), CD4 attachment (ibalizumab) | |
| Capsid inhibitor | Lenacapavir (long-acting injectable, every 6 months) |
Standard Regimen
A typical regimen = 2 NRTIs + 1 INSTI (preferred), or + 1 NNRTI, or + 1 boosted PI.
Preferred backbone: Tenofovir (TDF or TAF) + Emtricitabine (FTC) or Abacavir + 3TC.
A two-drug regimen of dolutegravir + 3TC is now supported for treatment-naive patients who are hepatitis B-negative with baseline HIV RNA <500,000 copies/mL.
Long-acting options include cabotegravir + rilpivirine (monthly or every-2-month injections) and lenacapavir (every 6 months).
One exception to immediate ART: in cryptococcal meningitis or TB, a few weeks of specific antimicrobial treatment first reduces the risk of severe immune reconstitution inflammatory syndrome (IRIS).
Harrison's Principles of Internal Medicine 22E, pp. 2043-2048
Opportunistic Infection Prophylaxis (CD4-based thresholds)
| CD4 Threshold | Prophylaxis |
|---|---|
| <200 cells/μL | TMP-SMX for PCP |
| <100 cells/μL | TMP-SMX also covers Toxoplasma |
| <50 cells/μL | Azithromycin for MAC; referral for CMV screening |
Prevention
- Pre-exposure prophylaxis (PrEP): Daily oral tenofovir/emtricitabine or long-acting injectable cabotegravir (every 2 months) for HIV-negative high-risk individuals. Highly effective (>99% when taken consistently).
- Post-exposure prophylaxis (PEP): 3-drug ART started within 72 hours of exposure, continued for 28 days.
- Undetectable = Untransmittable (U=U): People with sustained undetectable viral load cannot sexually transmit HIV.
- PMTCT: Prevention of mother-to-child transmission via maternal ART + infant prophylaxis reduces transmission to <1%.
Ethical and Legal Dimensions
- HIV testing requires pre-test and post-test counselling; results must be delivered face-to-face, not by phone or third party
- Mandatory testing (without individual consent) is permitted only for screening blood/organ/tissue donors
- HIV-positive healthcare workers cannot be removed from service if physically capable of performing duties (with appropriate precautions for exposure-prone procedures)
- WHO states there is no public health rationale for isolation, quarantine, or discrimination based on HIV status
Essentials of Forensic Medicine and Toxicology 36th edition, pp. 4836-4880
Current Evidence (2024-2026)
Recent systematic reviews highlight:
- Low-level viraemia (detectable but <200 copies/mL) is associated with increased risk of virological failure and warrants close monitoring - Zaçe et al., 2024 (PMID 39288983)
- Prevalence of low-level viraemia and its link to virological failure is well-characterized - Zhao et al., 2025 (PMID 39727007)
- Maternal viral load is the dominant driver of perinatal HIV transmission - Dugdale et al., 2025 Lancet (PMID 40652949)
Summary at a Glance
HIV (RNA retrovirus)
↓ binds CD4 + CCR5/CXCR4
↓ integrates as provirus
↓ progressive CD4+ T cell loss
↓ CD4 <200 OR AIDS-defining illness
= AIDS
↓
Opportunistic infections + Malignancies
↓ (without ART)
Death
ART interrupts this cascade. With sustained viral suppression, people living with HIV can expect near-normal lifespans and cannot sexually transmit the virus.
This is a shared conversation. Sign in to Orris to start your own chat.