What is OSA - OHS overlap what are its complications how it is manage
Reading File
Finding Sources
Finding Sources
Searching PubMed
"obesity hypoventilation syndrome" AND "obstructive sleep apnea" AND overlap
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile the full response.
OSA - OHS Overlap: Definition, Complications, and Management
What is OSA-OHS Overlap?
The OSA-OHS overlap refers to the coexistence of Obstructive Sleep Apnea (OSA) and Obesity Hypoventilation Syndrome (OHS) in the same patient - which, importantly, is the rule rather than the exception.
OHS is defined by three criteria:
- Obesity (BMI ≥ 30 kg/m²)
- Daytime hypercapnia (awake PaCO₂ ≥ 45 mmHg)
- Sleep-disordered breathing, after excluding other causes of alveolar hypoventilation (COPD, kyphoscoliosis, neuromuscular disease, opioids, sedative-hypnotics)
The overlap is extremely common: ~90% of OHS patients have concurrent OSA, and nearly 70% have severe OSA (AHI >30 events/hour). Conversely, OHS is present in 10-20% of obese patients referred for OSA evaluation. - Fishman's Pulmonary Diseases and Disorders, p. 1786
Pathophysiology of the Overlap
The diagram below illustrates how morbid obesity drives hypercapnia through multiple interacting mechanisms:
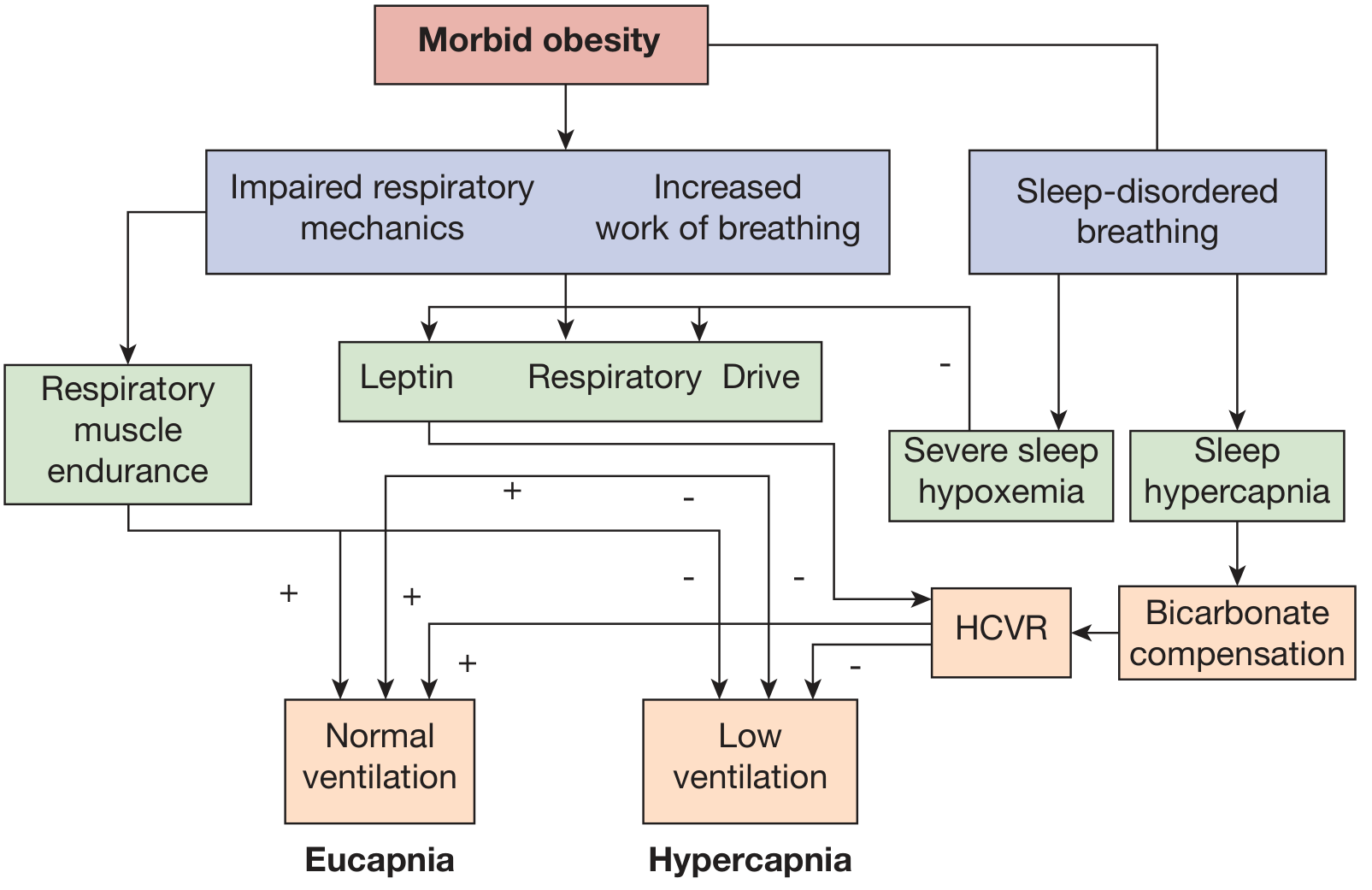
Interaction of pathophysiologic mechanisms in OHS. HCVR = hypercapnic ventilatory response. From Fishman's Pulmonary Diseases and Disorders.
Three key mechanisms interact:
-
Abnormal respiratory mechanics - Reduced chest wall and respiratory system compliance, increased airway resistance, expiratory flow limitation, intrinsic PEEP, and reduced respiratory muscle efficiency from abdominal fat load.
-
Sleep-disordered breathing (OSA) - During apneic and hypopneic events, CO₂ loads accumulate. If the inter-event compensatory hyperventilation is inadequate, kidneys retain bicarbonate to buffer the transient pH drop. This retained bicarbonate progressively blunts the central hypercapnic ventilatory response (HCVR), creating a vicious cycle of worsening hypercapnia.
-
Blunted central ventilatory drive - Central hypothalamic resistance to leptin (a respiratory stimulant produced by adipose tissue) further reduces the drive to breathe. - Fishman's Pulmonary Diseases and Disorders, p. 1787
Clinical Presentation
Patients with OSA-OHS overlap present with features of both conditions plus the distinctive hallmarks of chronic hypercapnia:
| Feature | Details |
|---|---|
| Excessive daytime sleepiness | Worse than in OSA alone; persists even after OSA is controlled |
| Morning headaches | From nocturnal CO₂ retention |
| Loud snoring, witnessed apneas | From concurrent OSA |
| Dyspnea | More frequent than in eucapnic OSA |
| Awake hypoxemia | PaO₂ typically <70 mmHg; SpO₂ <94% on room air |
| Facial plethora, injected sclera | From polycythemia |
| Signs of right heart failure | Peripheral edema, loud P2, elevated JVP |
A key differentiator: awake hypoxemia is uncommon in simple OSA - if a patient with OSA has SpO₂ <94% while awake, OHS must be actively excluded. - Fishman's Pulmonary Diseases and Disorders, p. 1787
Complications
OSA-OHS overlap carries substantially higher morbidity and mortality than either OSA or OHS alone:
Cardiovascular
- Pulmonary hypertension - More common and more severe than in either OSA or OHS alone; severe pulmonary hypertension is uncommon in pure OSA
- Cor pulmonale - Right heart failure resulting from pulmonary hypertension
- Systemic hypertension
- Congestive heart failure (biventricular)
- Angina / ischemic heart disease
Respiratory
- Acute-on-chronic hypercapnic respiratory failure - Patients often present to the ICU in decompensated state; this is frequently the first presentation that leads to diagnosis
- Polycythemia - From chronic nocturnal hypoxemia stimulating erythropoiesis
- Recurrent hospitalizations - Healthcare utilization is significantly elevated up to 5 years before OHS is even diagnosed
Metabolic
- Type 2 diabetes, metabolic syndrome - Obesity-driven comorbidities amplified by sleep fragmentation and hypoxemia
Mortality
- 2-year all-cause mortality of 23% in hospitalized patients with OHS (vs. 9% in simple obesity)
- 1-year mortality of 18% following acute hypercapnic respiratory failure admission
- One study of 600 OHS patients found 15% died on the index visit and another 16% died over 3 years of follow-up - Rosen's Emergency Medicine, p. 3501
- Untreated overlap syndrome has a relative mortality risk of 1.79 (95% CI 1.16-2.77) compared to COPD alone - Fishman's Pulmonary Diseases and Disorders, p. 1789
Diagnosis
Screening:
- Serum bicarbonate is the initial screening test for patients with low-moderate pretest probability of OHS
- Serum HCO₃ < 27 mEq/L dramatically decreases the probability of OHS (sensitivity 92%)
- HCO₃ ≥ 27 mEq/L or high clinical suspicion → proceed to arterial blood gas (ABG)
Confirmation:
- ABG showing PaCO₂ ≥ 45 mmHg while awake on room air, in the setting of BMI ≥ 30, with sleep-disordered breathing confirmed on polysomnography
Note: Chronic kidney disease and loop diuretics (common in this population) can independently elevate bicarbonate, limiting its specificity. - Fishman's Pulmonary Diseases and Disorders, p. 1787
Management
Treatment follows a stepwise, phenotype-based approach:
Step 1: Positive Airway Pressure (PAP) - First-Line
CPAP is the initial therapy for OSA-OHS overlap with severe OSA (AHI >30):
- Effective in 80% of patients with combined OSA-OHS - Murray & Nadel's Textbook of Respiratory Medicine
- Eliminates upper airway obstruction as the primary driver of CO₂ retention
- Improves daytime hypercapnia and hypoxemia in >50% of patients
- Use objectively monitored CPAP adherence to confirm response
How to assess CPAP response:
- Reassess serum bicarbonate or ABG after several weeks of CPAP with documented adherence
- Normalization of serum HCO₃ or PaCO₂ confirms adequate treatment
Step 2: BiPAP (Bilevel PAP) - If CPAP Fails
BiPAP-S (Spontaneous mode) is indicated when:
- Patient cannot tolerate high CPAP pressures required
- Residual obstructive events persist at maximum CPAP (20 cmH₂O)
- Ongoing hypercapnia despite adequate CPAP adherence after 3 months
BiPAP-S provides both expiratory PAP (to maintain airway patency) and inspiratory pressure support (to augment tidal volume and offload CO₂).
Step 3: BiPAP-ST or VAPS - Backup Rate Modes
BiPAP-ST (Spontaneous/Timed) or AVAPS/iVAPS (volume-assured pressure support) is indicated when:
- Reduced respiratory drive results in inadequate minute ventilation on BiPAP-S
- No improvement or worsening CO₂ on BiPAP-S monitoring
- Malignant OHS phenotype (low AHI but severe hypercapnia, >50 kg/m² BMI)
- OHS without significant OSA (these patients should start at BiPAP-ST directly)
- Acute decompensated OHS requiring hospital admission
Settings guidance for BiPAP-ST:
- Target Vt: 8-10 mL/kg ideal body weight
- Backup rate: ~2 breaths below the patient's spontaneous rate
- Prolong inspiratory time (Ti) to allow recruitment of atelectatic basilar segments
- EPAP set to abolish obstructive events; titrated to AHI severity - Murray & Nadel's Textbook of Respiratory Medicine, pp. 2831
Step 4: Weight Loss and Bariatric Surgery
- Substantial weight loss (20-25% of actual body weight) alone can normalize PaCO₂
- Bariatric surgery is recommended by the American Thoracic Society guideline for eligible patients
- Achieving this degree of weight loss without surgery is very challenging
Step 5: Supplemental Oxygen
- Supplemental O₂ alone is not appropriate as primary treatment for OSA-OHS - PAP therapy is needed
- Long-term oxygen therapy (LTOT) may be added adjunctively in patients with refractory hypoxemia but should not replace NIPPV - Fishman's Pulmonary Diseases and Disorders, p. 3706
Summary Treatment Algorithm
OSA-OHS overlap confirmed (AHI ≥ 30 + PaCO₂ ≥ 45)
│
▼
Start CPAP → Reassess in 3 months (adherence + ABG/HCO₃)
│
┌────┴────────────────────┐
Resolved Persistent hypercapnia
(80% of cases) │
Escalate to BiPAP-S
│
Still hypercapnic or low MV?
│
BiPAP-ST or VAPS (backup rate)
│
All patients: weight loss counseling
+ bariatric surgery evaluation
Pharmacologic Agents
Agents such as medroxyprogesterone (a respiratory stimulant) and acetazolamide have been poorly studied and should not replace PAP therapy. They are not recommended as substitutes for definitive treatment. - Harrison's Principles of Internal Medicine 22E, p. (OHS section)
Key Takeaways
| Aspect | Detail |
|---|---|
| OSA in OHS | 90% have OSA; 70% have severe OSA |
| CPAP efficacy in overlap | Effective in 80% |
| Screening test | Serum HCO₃ (<27 = OHS unlikely) |
| Diagnostic gold standard | ABG: awake PaCO₂ ≥45 mmHg |
| 2-year mortality (untreated OHS) | ~23% in hospitalized patients |
| First-line therapy | CPAP for AHI ≥30; BiPAP-ST for low AHI/malignant phenotype |
| Target of therapy | Normalization of PaCO₂ and serum HCO₃ |
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Harrison's Principles of Internal Medicine 22E (2025); Rosen's Emergency Medicine
What is AHI events
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation of AHI events.
AHI (Apnea-Hypopnea Index)
Definition
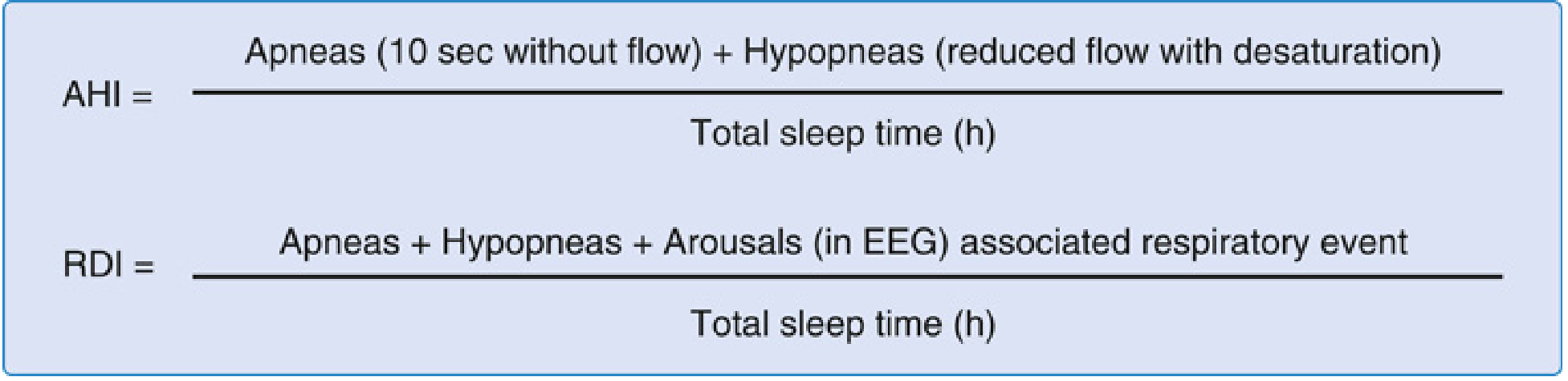
The AHI is the total number of apneas and hypopneas divided by total sleep time in hours. It is the standard metric used to diagnose and grade the severity of sleep-disordered breathing (SDB). - Fishman's Pulmonary Diseases and Disorders
What Counts as an AHI Event?
AHI counts two types of respiratory events:
1. Apnea
A near-total or complete cessation of airflow during sleep.
Criteria (AASM):
- Drop in peak respiratory signal ≥ 90% from baseline
- Duration ≥ 10 seconds
- No oxygen desaturation or arousal is required to score an apnea
Three subtypes:
| Type | Airflow | Respiratory Effort |
|---|---|---|
| Obstructive apnea | Absent | Present (continued chest/abdominal effort) |
| Central apnea | Absent | Absent (no effort at all) |
| Mixed apnea | Absent | Starts central, then effort resumes later in the event |
2. Hypopnea
A partial reduction in airflow - less severe than a full apnea but still clinically significant.
Criteria:
- Airflow reduction ≥ 30% from baseline lasting ≥ 10 seconds
- PLUS either:
- ≥ 3-4% drop in SpO₂ (oxygen desaturation), OR
- An arousal from sleep on EEG
Note: The AASM accepts a 3% SpO₂ drop or an arousal; some bodies (e.g., Medicare) use 4%. This difference in definition significantly affects reported disease prevalence. - Fishman's Pulmonary Diseases and Disorders, p. 1731
Related Index - RDI (Respiratory Disturbance Index)
The RDI goes one step further than AHI:
RDI = (Apneas + Hypopneas + RERAs) ÷ Total Sleep Time
RERA (Respiratory Effort-Related Arousal): A series of breaths with increasing respiratory effort that leads to an arousal from sleep - but does not meet the full criteria for apnea or hypopnea. RERAs represent a milder form of sleep-disordered breathing and are included in RDI but not in AHI.
Since RDI includes RERAs, RDI ≥ AHI in any given patient.
AHI Severity Classification
| AHI (events/hour) | Severity |
|---|---|
| < 5 | Normal (up to 5 events/hour can occur in healthy adults) |
| 5 - 14 | Mild OSA |
| 15 - 30 | Moderate OSA |
| > 30 | Severe OSA |
- Miller's Anesthesia, 10e; Fishman's Pulmonary Diseases and Disorders
Diagnosis of OSA requires:
- AHI ≥ 5 events/hour on polysomnography (PSG), with obstructive or mixed events >50% of total
- PLUS symptoms (excessive daytime sleepiness, unrefreshing sleep, fatigue), OR
- AHI ≥ 15 events/hour regardless of symptoms
Treatment is recommended for moderate to severe disease (AHI ≥ 15), primarily with CPAP. - Miller's Anesthesia, 10e
REI - Home Sleep Testing Variant
When OSA is diagnosed with a Home Sleep Apnea Test (HSAT) rather than in-lab polysomnography, the index is called the REI (Respiratory Event Index):
REI = Apneas + Hypopneas ÷ Total monitoring time (not just sleep time)
Since HSAT cannot measure exact sleep time, the denominator is total recording time, so REI tends to underestimate true AHI - leading to possible under-diagnosis of severe OSA. - Fishman's Pulmonary Diseases and Disorders, p. 1732
Why AHI Has Limitations
While AHI is the gold-standard metric, it has recognized shortcomings:
- It does not capture the depth or duration of hypoxemia per event
- A patient with 20 short apneas with mild desaturation may have a higher AHI than a patient with 10 long apneas with severe desaturation - yet the latter may have greater cardiovascular risk
- Recent evidence shows "hypoxic burden" (area under the desaturation curve during respiratory events) is a stronger predictor of cardiovascular mortality than AHI alone - Fishman's Pulmonary Diseases and Disorders, p. 1732
Quick Summary
| Term | Full Name | Includes |
|---|---|---|
| AHI | Apnea-Hypopnea Index | Apneas + Hypopneas ÷ sleep hours |
| RDI | Respiratory Disturbance Index | Apneas + Hypopneas + RERAs ÷ sleep hours |
| REI | Respiratory Event Index | Apneas + Hypopneas ÷ monitoring hours (home testing) |
In the context of OSA-OHS overlap discussed earlier: AHI > 30 = severe OSA, which is present in ~70% of OHS patients and is the threshold above which CPAP is the preferred first-line treatment.
This is a shared conversation. Sign in to Orris to start your own chat.