Blood supply of brain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Now I have comprehensive information from Gray's Anatomy for Students, Neuroscience: Exploring the Brain, and Neuroanatomy through Clinical Cases. Here is the full answer:
Blood Supply of the Brain
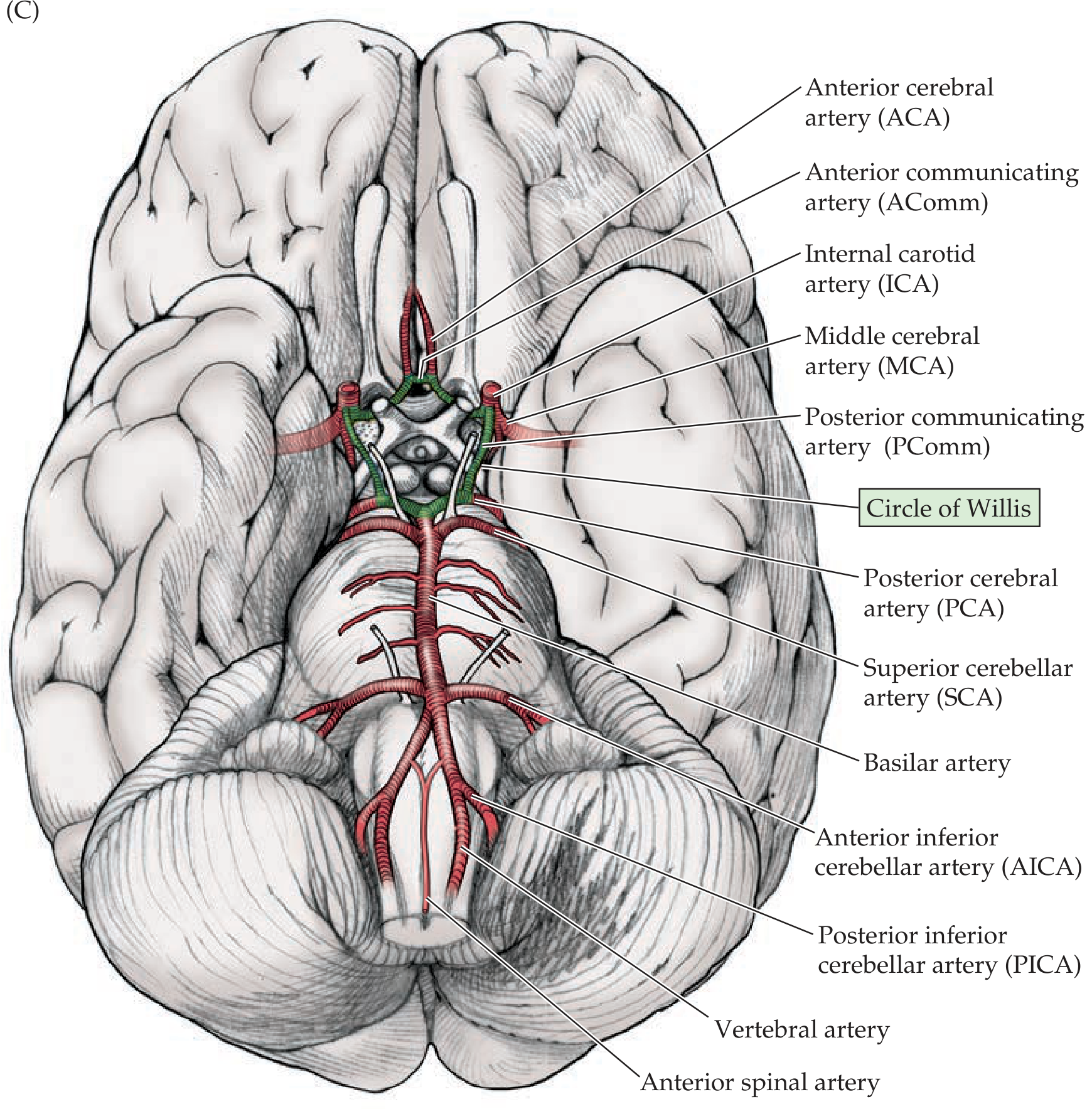
The brain receives its entire arterial supply from two pairs of vessels: the internal carotid arteries (anterior circulation) and the vertebral arteries (posterior circulation). These interconnect at the base of the brain to form the cerebral arterial circle (Circle of Willis).
- Gray's Anatomy for Students, p. 1017
1. Anterior Circulation - Internal Carotid Arteries (ICA)
- Each ICA arises as a terminal branch of the common carotid artery in the neck
- Ascends to the skull base and enters via the carotid canal
- On entering the cranial cavity, each ICA gives off four main branches:
- Ophthalmic artery - supplies the orbit and eye
- Posterior communicating artery (PComm) - connects ICA to the posterior cerebral artery, completing the circle of Willis
- Middle cerebral artery (MCA) - the largest branch
- Anterior cerebral artery (ACA)
2. Posterior Circulation - Vertebral Arteries
- Each vertebral artery arises from the first part of the subclavian artery in the lower neck
- Ascends through the foramina transversaria of the upper six cervical vertebrae
- Enters the skull through the foramen magnum
Branches of each vertebral artery:
- Small meningeal branch
- Posterior inferior cerebellar artery (PICA) - supplies posterior/inferior cerebellum and lateral medulla
- Posterior spinal artery - descends along posterior spinal cord
- Contribution to the anterior spinal artery (formed by union of branches from both vertebral arteries)
Basilar artery:
- Formed by the union of both vertebral arteries just inferior to the pons
- Travels rostrally along the anterior surface of the pons
- Branches (caudal to rostral):
- Anterior inferior cerebellar arteries (AICA)
- Pontine arteries (several small branches to pons)
- Superior cerebellar arteries (SCA)
- Terminates by bifurcating into the two posterior cerebral arteries (PCA)
- Gray's Anatomy for Students, p. 1017-1018
3. Circle of Willis (Cerebral Arterial Circle)
The circle of Willis is an anastomotic ring at the base of the brain connecting the anterior and posterior circulations. It is formed by:
| Component | Contribution |
|---|---|
| Anterior cerebral arteries (L + R) | Anterior portion |
| Anterior communicating artery | Connects the two ACAs |
| Internal carotid arteries (L + R) | Lateral portions |
| Posterior communicating arteries (L + R) | Connect ICA to PCA on each side |
| Posterior cerebral arteries (L + R) | Posterior portion |
This ring provides collateral flow - if one vessel is blocked, blood can potentially reach the affected territory through alternative routes.
- Neuroanatomy through Clinical Cases 3rd Ed., p. 70-71
4. Regional Blood Supply of the Cerebral Hemispheres
Ventral view (base of brain):
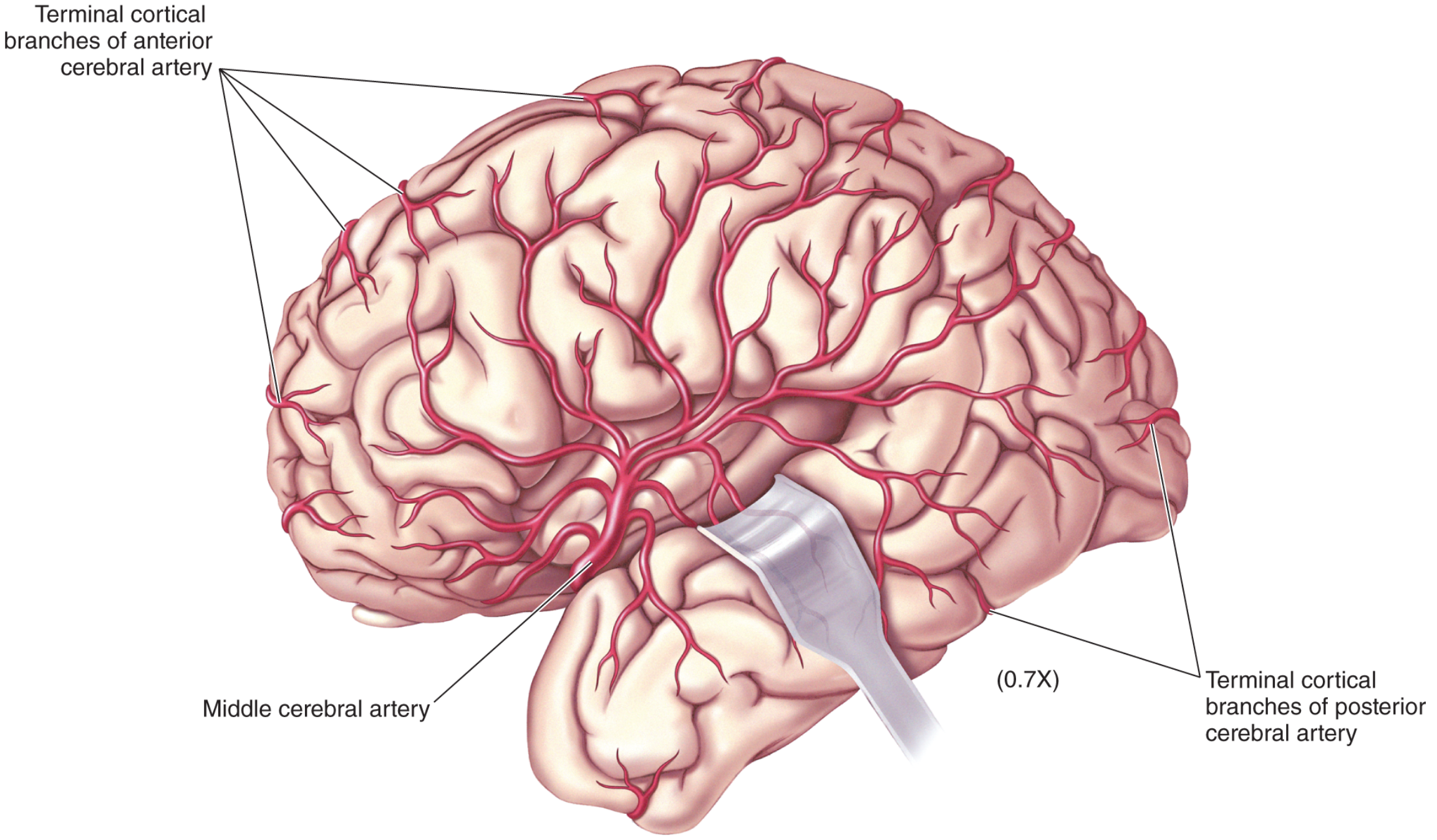
Lateral surface view:
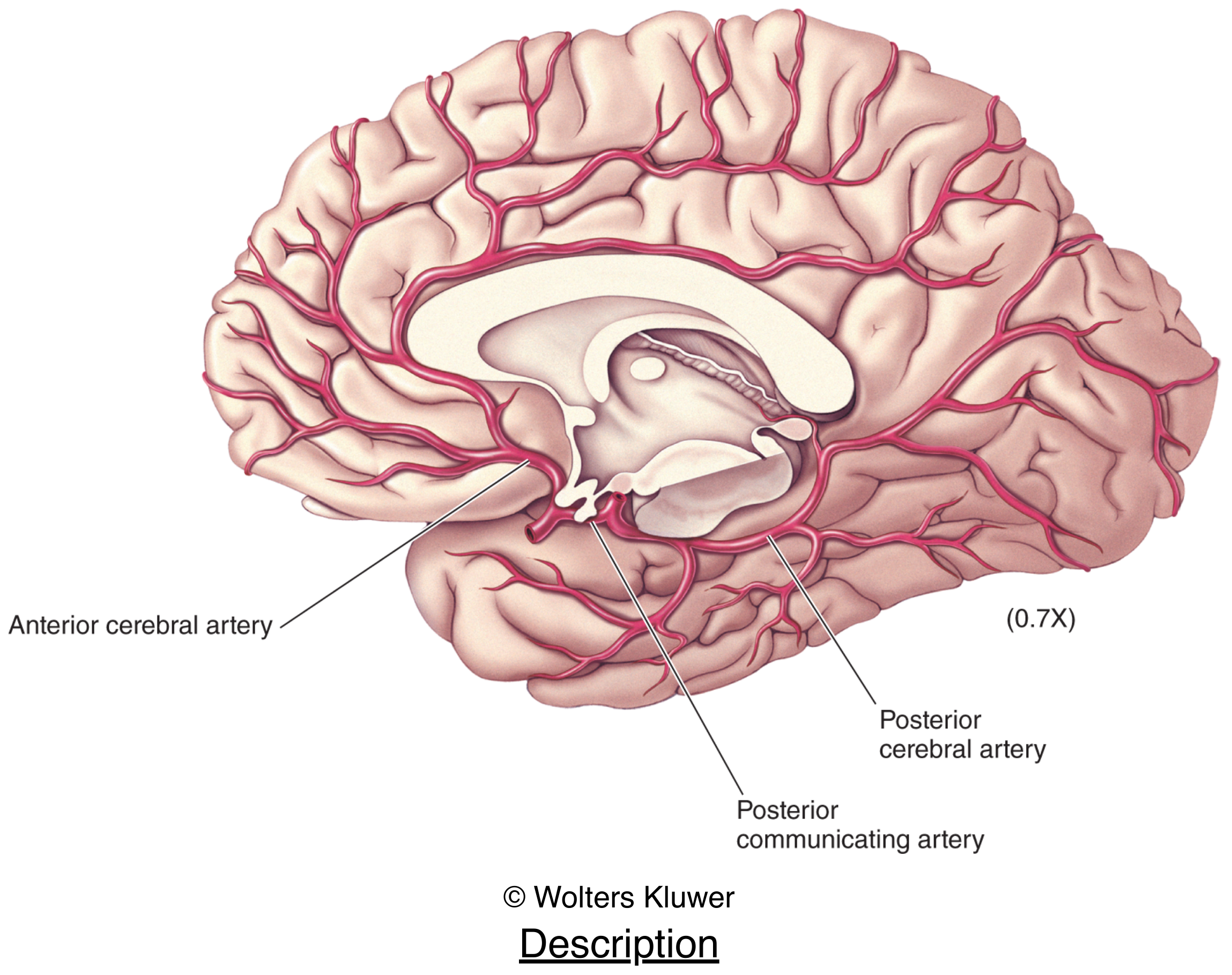
Medial surface view (brainstem removed):
| Artery | Region Supplied |
|---|---|
| ACA | Medial frontal and parietal lobes, anterior corpus callosum, leg/foot area of motor/sensory cortex |
| MCA | Most of the lateral surface of the cerebrum; deep structures of basal forebrain (lenticulostriate arteries); face, arm, trunk areas of cortex; Broca's and Wernicke's areas (dominant hemisphere) |
| PCA | Medial wall of occipital lobe, inferior temporal lobe, thalamus, posterior limb of internal capsule |
| SCA | Superior surface of cerebellum |
| AICA | Anterior inferior cerebellum, lateral pons (lower) |
| PICA | Posterior inferior cerebellum, lateral medulla |
- Neuroscience: Exploring the Brain 5th Ed., p. 705-707
5. Venous Drainage
Venous drainage of the brain is provided almost entirely by the internal jugular veins. Cortical veins drain into dural venous sinuses (superior sagittal, transverse, sigmoid sinuses), which ultimately empty into the internal jugular veins bilaterally.
- Neuroanatomy through Clinical Cases 3rd Ed., p. 71
Clinical Correlates
- MCA stroke (most common): contralateral hemiparesis/hemisensory loss (face and arm > leg), aphasia (dominant hemisphere), hemineglect (non-dominant)
- ACA stroke: contralateral leg weakness > arm; personality changes (frontal lobe)
- PCA stroke: contralateral homonymous hemianopia, thalamic pain syndrome
- Vertebrobasilar stroke: diplopia, dysphagia, ataxia, ipsilateral facial + contralateral limb sensory loss (lateral medullary/Wallenberg syndrome from PICA)
- Berry aneurysms arise most commonly at branching points of the Circle of Willis - classically at the anterior communicating artery, posterior communicating artery, MCA bifurcation, and basilar tip
- Watershed infarcts occur at the border zones between ACA/MCA and MCA/PCA territories during hypoperfusion states
- Gray's Anatomy for Students, p. 1019-1020
Brain hemorrhages
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Excellent - I now have comprehensive material from multiple textbooks with CT images. Here is the full structured answer:
Brain Hemorrhages
Brain hemorrhages are classified by their anatomical location - which space or compartment the blood collects in. There are four main types:
Classification Overview
| Type | Space | Source Vessel | Cause |
|---|---|---|---|
| Extradural (Epidural) | Between skull & dura | Middle meningeal artery | Trauma (arterial) |
| Subdural | Between dura & arachnoid | Bridging veins | Trauma (venous) |
| Subarachnoid | Between arachnoid & pia | Circle of Willis aneurysm | Spontaneous/trauma |
| Intracerebral (Intraparenchymal) | Within brain tissue | Perforating arteries | Hypertension, CAA |
1. Extradural (Epidural) Hematoma (EDH)
Source: Arterial - tearing of branches of the middle meningeal artery, typically at the pterion (the thinnest point of the skull, where the four cranial bones meet at the temple).
Mechanism: A blow to the temporal region fractures the thin bone and tears the middle meningeal artery. Blood collects between the periosteal layer of the dura and the calvaria under arterial pressure.
Classic presentation:
- Blow to the head with brief loss of consciousness
- Lucid interval (hours) - the patient regains consciousness
- Then rapid drowsiness, deterioration, and coma
- Contralateral hemiplegia + ipsilateral dilated pupil (uncal herniation from CN III compression)
CT appearance: Biconvex (lenticular/lens-shaped) hyperdense collection - does not cross suture lines (dura is firmly attached at sutures).
CT scan - Extradural hematoma with midline shift:
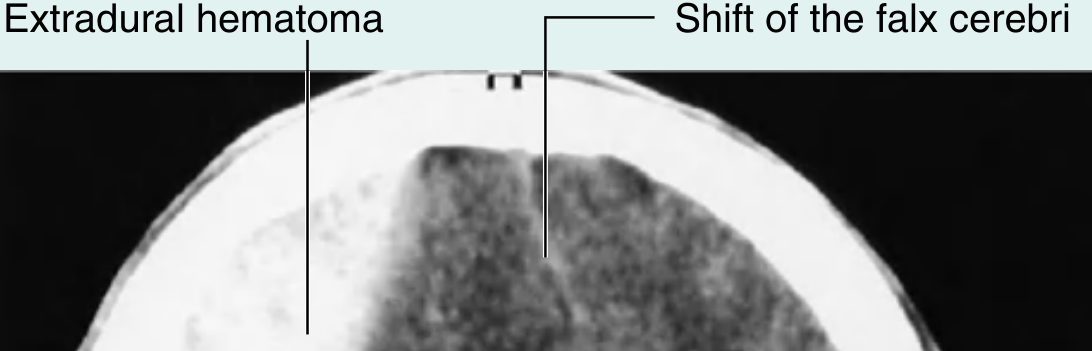
Management: Neurosurgical emergency - craniotomy and evacuation. Without prompt drainage, fatal brain herniation can occur within hours.
- Gray's Anatomy for Students, p. 1029; Robbins Pathologic Basis of Disease, p. 1162
2. Subdural Hematoma (SDH)
Source: Venous - tearing of parasagittal bridging veins that drain from the cerebral cortex surface into the dural venous sinuses (superior sagittal sinus). The extravasated blood dissects through the dural border cell layer.
Mechanism: Acceleration-deceleration of the brain relative to the fixed dural sinuses stretches and tears the bridging veins. The brain is suspended in CSF; the sinuses are fixed in the dura - any displacement tears these veins at the dura entry point.
High-risk groups:
- Elderly (brain atrophy stretches the bridging veins and creates more movement space)
- Infants (thin-walled bridging veins; shaken baby syndrome)
- Alcoholics (brain atrophy + coagulopathy)
- Patients on anticoagulation
Subtypes by timing:
- Acute SDH (< 3 days): Rapid hematoma development, brainstem compression, high mortality. Blood is from bridging veins, cortical arteries, or cerebral lacerations.
- Subacute SDH (3 days to 3 weeks): Symptoms develop gradually; clot contains dark fluid with peripheral membrane formation.
- Chronic SDH (> 3 weeks): Often from trivial trauma; insidious personality change or altered consciousness. The hematoma liquefies; fibroblasts grow in from the dura forming a membrane. Thin-walled vessels in the granulation tissue can rebleed, creating "acute on chronic" SDH.
CT appearance: Crescent-shaped hyperdense (acute) or hypodense (chronic) collection that conforms to the brain surface and can cross suture lines. Midline shift is prominent.
Chronic subdural hematoma CT (low-density crescent, midline shift):

Gross pathology - organizing subdural hematoma:
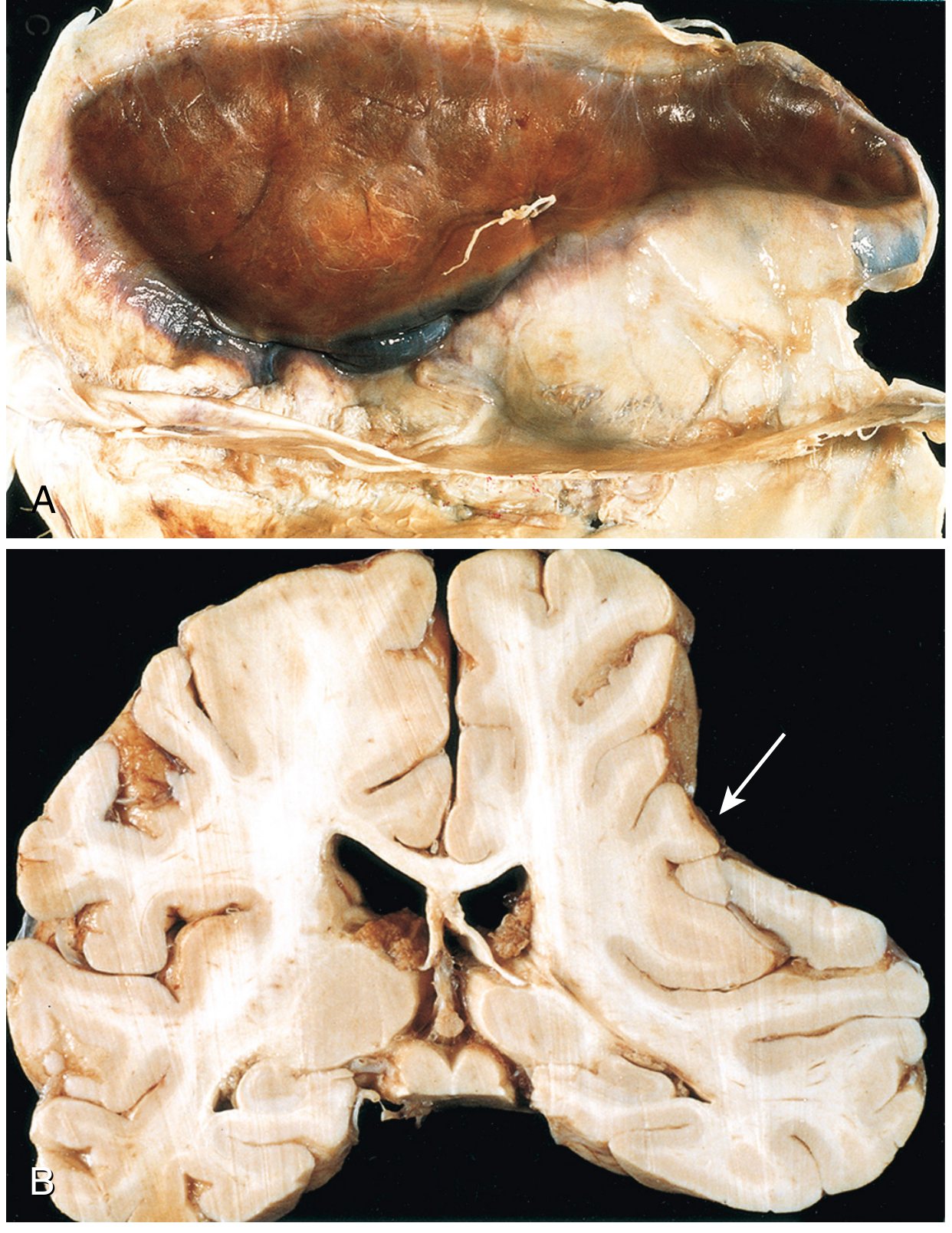
Organization sequence (Robbins):
- Lysis of clot (~1 week)
- Fibroblast ingrowth from dura (2 weeks)
- Early hyalinized connective tissue (1-3 months)
- Final "subdural membrane" or rebleeding from fragile granulation vessels
Management: Monitoring (small), burr-hole drainage (chronic liquefied), or open craniotomy (large acute SDH).
- Robbins Pathologic Basis of Disease, p. 1162; Gray's Anatomy for Students, p. 1029; Forensic Medicine & Toxicology 36th Ed.
3. Subarachnoid Hemorrhage (SAH)
Source: Rupture of a saccular (berry) aneurysm at branch points of the Circle of Willis. Less commonly from superficial AVM rupture or trauma.
Common aneurysm locations:
- Anterior communicating artery (AComm) - most common
- Posterior communicating artery (PComm) - causes CN III palsy when expanding
- Middle cerebral artery bifurcation
- Basilar artery tip
- Posterior cerebral artery origin
Pathophysiology: Saccular aneurysms arise from a defect in the tunica media at vessel bifurcations. They enlarge over time and are silent until rupture. About 25% have a "sentinel headache" (sudden severe headache from minor leakage) days before major rupture.
Classic presentation:
- Sudden "thunderclap headache" - worst headache of life
- Neck stiffness (meningism from blood in CSF)
- Photophobia, nausea/vomiting
- Loss of consciousness at onset (ICP spikes to near arterial pressure)
- New-onset anisocoria = posterior communicating artery aneurysm until proven otherwise
Prognosis: About 20% die before reaching hospital. Overall mortality 40-50%. Even grades I/II deteriorate in ~50% from vasospasm, rebleeding, or hydrocephalus.
Grading (Hunt & Hess / WFNS): Based on GCS and neurological deficits. Grade V (GCS 3) still has ~22% good outcome possibility.
Complications:
- Rebleeding (highest risk 24-48 hrs) - 50% mortality if re-rupture causes coma
- Vasospasm (days 4-14) - causes delayed cerebral ischemia; treated with nimodipine
- Hydrocephalus - blood in CSF obstructs arachnoid granulations
- Hyponatremia (cerebral salt wasting)
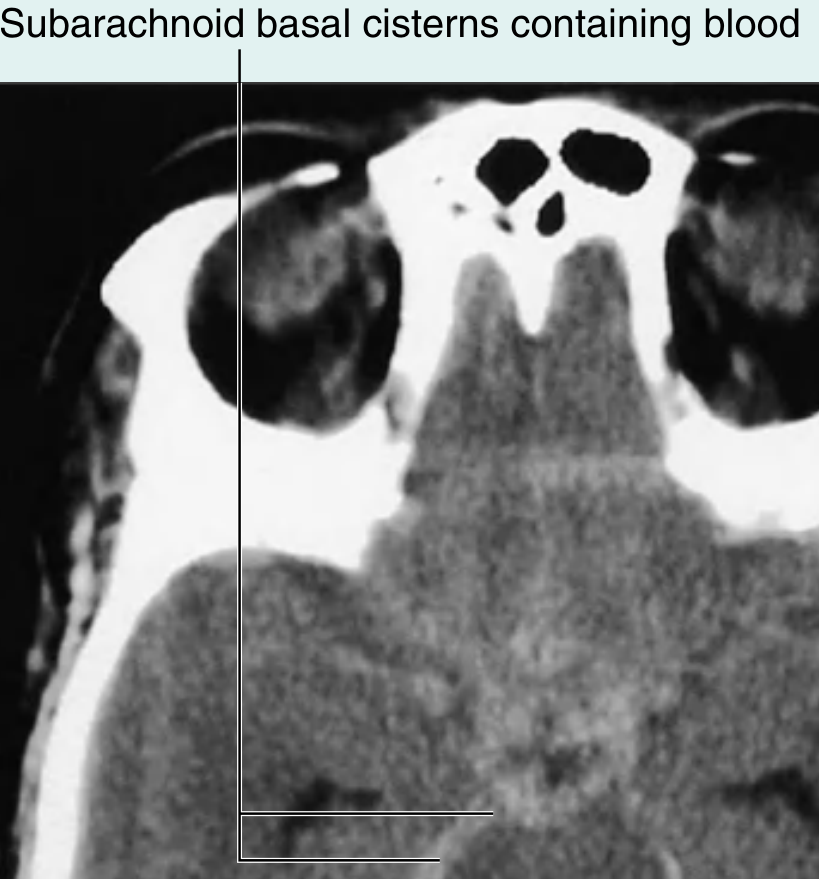
CT appearance: Hyperdense blood filling the basal cisterns and sulci ("star pattern" at base of brain). If CT is negative and SAH suspected, LP must be done (xanthochromia).
- Plum & Posner's Diagnosis and Treatment of Stupor and Coma, p. 260-261
4. Intracerebral Hemorrhage (ICH) / Intraparenchymal Hemorrhage
Source: Rupture of small perforating arteries deep within the brain parenchyma.
Causes:
| Cause | Details |
|---|---|
| Hypertension (most common) | Charcot-Bouchard microaneurysms in lenticulostriate, thalamic, basilar perforating arteries |
| Cerebral amyloid angiopathy (CAA) | Elderly patients; lobar hemorrhages; amyloid deposits weaken vessel walls |
| Anticoagulation / thrombolytics | |
| AVM / cavernous malformation | |
| Hemorrhagic transformation of ischemic stroke | |
| Cocaine/stimulant use |
Typical hypertensive ICH locations (perforating artery territories):
- Putamen/basal ganglia (most common - 35-50%) - lenticulostriate arteries
- Thalamus - thalamic perforators
- Pons - basilar perforating arteries (pinpoint pupils, quadriplegia)
- Cerebellum - superior cerebellar artery branches (headache, ataxia, vomiting)
- Lobar - often CAA in elderly
CT appearance: Round or oval hyperdense lesion (40-80+ HU acutely) - surrounded by hypodense edema halo.
Intracerebral hemorrhage CT (right temporal lobe hyperdensity):
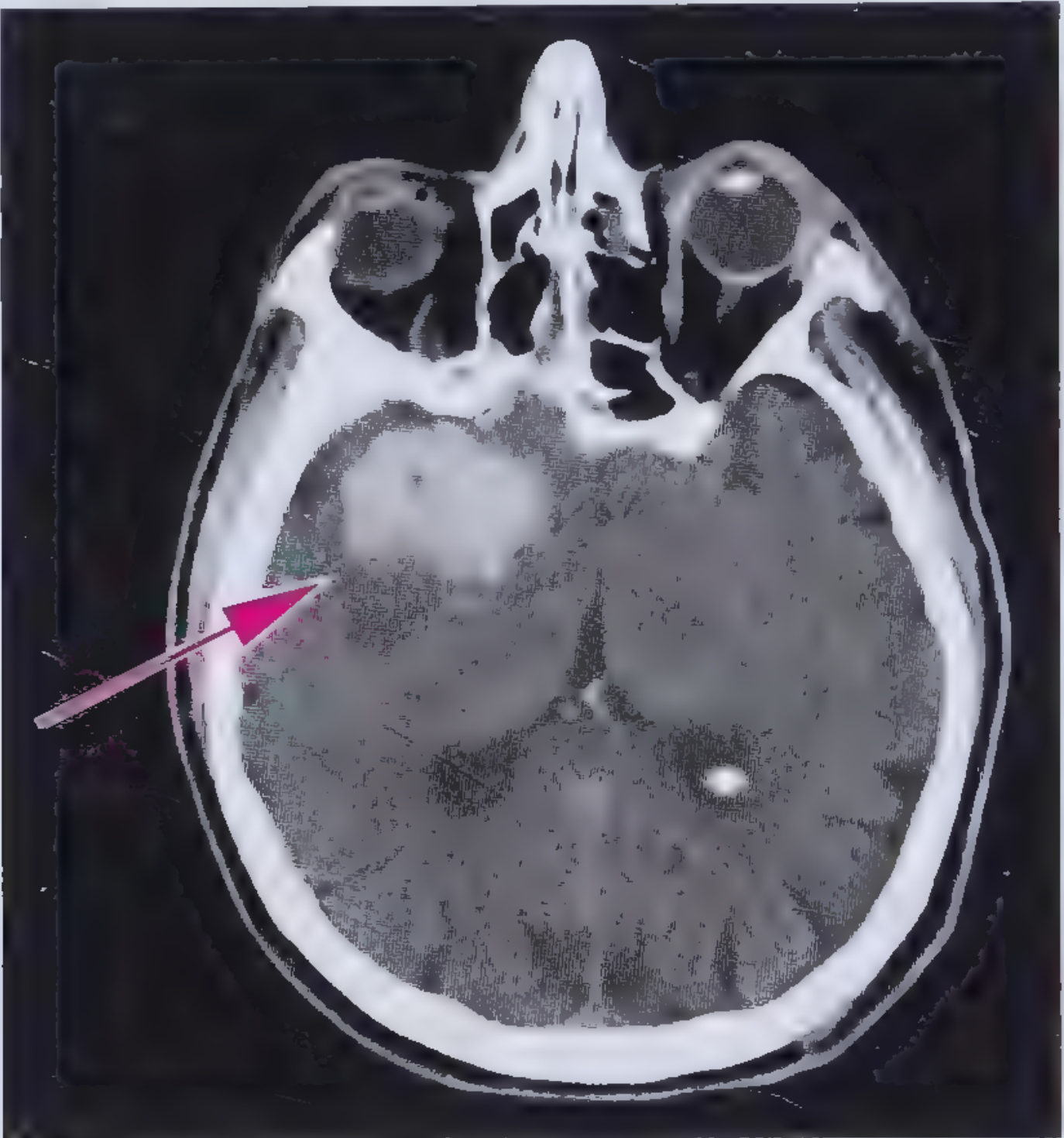
30-day mortality: ~50%.
Management of acute spontaneous ICH:
- Reverse coagulopathy (e.g., vitamin K + FFP for warfarin)
- Lower SBP to 140 mmHg if SBP 150-220 mmHg
- Control blood sugar (avoid hypo- and hyperglycemia)
- Treat seizures with antiepileptics
- ICP management: HOB elevation 30°, hyperosmolar therapy, intubation/sedation
- Cerebellar hematoma > 3 cm or causing hydrocephalus: surgical evacuation
- Frameworks for Internal Medicine, p. 438-480; Gray's Anatomy for Students, p. 1028
Quick Comparison at a Glance
| Feature | EDH | SDH | SAH | ICH |
|---|---|---|---|---|
| Space | Epidural | Subdural | Subarachnoid | Parenchymal |
| Vessel | Middle meningeal a. | Bridging veins | Berry aneurysm | Perforating aa. |
| Blood type | Arterial | Venous | Arterial | Arterial |
| CT shape | Biconvex | Crescent | Basal cisterns | Round/oval |
| CT density | Hyperdense | Hyperdense (acute) | Hyperdense | Hyperdense |
| Crosses sutures? | No | Yes | N/A | N/A |
| Key history | Lucid interval | Trivial/no trauma (chronic) | Thunderclap HA | Hypertension |
| Classic age | Young adult | Elderly/infant | 40-60 yrs | 50-70 yrs |
Brain hemorrhages
I just covered this topic in detail in my previous response. Here's a quick summary of what was covered:
Brain Hemorrhages - Summary
Brain hemorrhages are classified by the anatomical compartment where blood collects:
1. Extradural (Epidural) Hematoma
- Vessel: Middle meningeal artery (arterial)
- Shape on CT: Biconvex/lenticular, does NOT cross suture lines
- Classic sign: Lucid interval after head trauma, then rapid deterioration
- Cause: Pterion fracture
2. Subdural Hematoma
- Vessel: Bridging veins (venous)
- Shape on CT: Crescent-shaped, DOES cross suture lines
- Classic sign: Trivial trauma in elderly; insidious onset
- Types: Acute (<3 days), Subacute (3 days-3 weeks), Chronic (>3 weeks)
3. Subarachnoid Hemorrhage
- Vessel: Berry aneurysm at Circle of Willis branches
- CT: Blood in basal cisterns
- Classic sign: "Worst headache of life" (thunderclap)
- Complications: Vasospasm, rebleeding, hydrocephalus
4. Intracerebral (Intraparenchymal) Hemorrhage
- Vessel: Perforating arteries (hypertensive Charcot-Bouchard microaneurysms)
- CT: Round hyperdense lesion with surrounding edema
- Common sites: Putamen, thalamus, pons, cerebellum
- Main cause: Hypertension; also cerebral amyloid angiopathy (CAA) in elderly
If you'd like me to go deeper on any specific type - mechanisms, management, grading scales, complications, or imaging findings - just ask.
Provide images
Loading Image
Loading Image
Subarachnoid Hemorrhage
CT scan - hyperdense blood filling the subarachnoid basal cisterns around the brainstem:
Summary - CT Appearance at a Glance
| Type | CT Shape | Density | Key Feature |
|---|---|---|---|
| EDH | Biconvex (lens) | Hyperdense | Does NOT cross sutures |
| SDH | Crescent | Hyperdense (acute) / Hypodense (chronic) | Crosses sutures, midline shift |
| SAH | Fills cisterns/sulci | Hyperdense | Basal cistern "star" pattern |
| ICH | Round/oval | Hyperdense | Deep brain, edema halo |
All images sourced from Gray's Anatomy for Students and Robbins Pathologic Basis of Disease.
This is a shared conversation. Sign in to Orris to start your own chat.