indication of starting lasix in severe lvdef with aki
Reading File
Finding Sources
Finding Sources
Searching PubMed
furosemide "acute kidney injury" "heart failure" diuresis
Finding Sources
Finding Sources
Searching PubMed
diuretic "acute decompensated heart failure" "acute kidney injury" cardiorenal
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive information from authoritative sources. Let me compile the full answer.
Indications for Starting Furosemide (Lasix) in Severe LV Dysfunction (HFrEF) with AKI
This is one of the most challenging dilemmas in cardiology/nephrology - AKI in the context of severe LV dysfunction is often caused by venous congestion rather than reduced cardiac output, and diuresis is frequently the correct treatment rather than a contraindication.
The Central Principle: AKI Type Determines Whether to Diurese
Before deciding, you must classify the AKI:
| AKI Type | Mechanism | Response to Furosemide |
|---|---|---|
| Congestion-driven (Type 1 CRS) | Elevated venous pressure → ↑ renal venous pressure → ↓ GFR | Furosemide indicated |
| Low-output/forward failure | ↓ CO → ↓ renal arterial perfusion (prerenal) | Furosemide may worsen |
| Mixed | Both mechanisms | Careful diuresis with monitoring |
As Harrison's (22e) notes, "venous congestion in HF with increased backward pressure may be operative in determining the development of the cardiorenal syndrome, and relief of venous congestion is associated with significant improvement in renal function in HF." - Harrison's Principles of Internal Medicine 22E, p. 2025
Indications to Start/Continue Furosemide Despite AKI
1. Clear clinical evidence of volume overload/congestion:
- Elevated JVP, peripheral edema, ascites, orthopnea, PND
- Pulmonary rales, chest X-ray showing pulmonary vascular congestion, pleural effusions
- Elevated BNP/NT-proBNP
2. Cardiorenal Syndrome Type 1 (AKI caused by acute HF decompensation):
- The NKF Primer states: "The most evidence-based treatment of CRS is the relief of venous congestion. Numerous observations show a direct correlation between effective measures to reduce volume overload and improved outcomes in patients with CRS." - National Kidney Foundation Primer on Kidney Diseases, 8e, p. 331
- In this context, the AKI itself is an indication to decongestion, not a contraindication.
3. Rising creatinine does not automatically mean stop diuresis:
- A mild/moderate rise in creatinine during active decongestion (so-called "worsening renal function" or WRF) is often acceptable and even expected.
- Studies have shown that patients who achieve adequate decongestion - even if they develop transient WRF - have better long-term outcomes than those with preserved creatinine but inadequate decongestion.
4. Symptomatic relief requirement:
- Severe dyspnea, hypoxemia, or inability to maintain oxygen saturation - diuresis is urgently indicated regardless of creatinine.
Practical Decision Framework
Severe HFrEF + AKI
|
Is the patient volume overloaded (congested)?
|
YES NO (or low output state)
| |
Start IV furosemide Assess CO/hemodynamics
(double home oral dose Consider inotropes first
or 1-2.5x home dose IV) Cautious or no diuresis
|
Monitor response at 6-12h:
- Urine output target: ≥100-150 mL/h
- Urine sodium in first void (>50 mEq/L = adequate response)
- Daily weight, net fluid balance
|
Inadequate response?
|
Add thiazide (metolazone) - "dual nephron blockade"
Dosing Guidance
From the NKF Primer (p. 331):
- IV route is mandatory in acute decompensation (oral furosemide has variable bioavailability of 10-90%, mean 50%)
- Starting dose: Double the patient's home oral dose and give intravenously
- Equivalency: furosemide 80 mg oral = furosemide 40 mg IV = torsemide 20 mg oral = bumetanide 1 mg oral/IV
- Bolus vs. continuous infusion: The DOSE trial showed no significant efficacy difference - either is acceptable
- GFR <30 mL/min: Consider bumetanide over furosemide as its excretion is minimally affected by reduced kidney function, and it has lower risk of ototoxicity
When NOT to Diurese (Relative Contraindications)
- Cardiogenic shock / systolic BP <90 mmHg without vasopressors
- Clinically volume-depleted (dry patient - elevated urea:creatinine ratio, flat JVP, dry mucous membranes)
- AKI clearly from a non-congestion cause (e.g., nephrotoxin, obstruction, intrinsic renal disease)
- Severe hypokalemia or hyponatremia requiring correction first
If Furosemide Resistance Develops
- Add metolazone 2.5-5 mg oral 30 min before IV furosemide (dual nephron blockade) - watch for hypokalemia and hypomagnesemia
- Increase furosemide dose before switching strategies
- Consider ultrafiltration as a last resort (note: CARESS-HF trial showed no benefit over aggressive pharmacologic diuresis)
- Dopamine low-dose may be tried in refractory CRS not responding to first-line decongestion - but routine use is not recommended (ROSE and DAD-HF trials were negative)
- Inotropes (dobutamine, milrinone) if co-existing low-output state is confirmed
Key Take-Home Points
- The AKI of congested HFrEF is often the indication FOR furosemide, not against it.
- The pathophysiology is backward pressure (renal venous hypertension) → ↓GFR; decongesting the venous circuit relieves this.
- Accept a small rise in creatinine if the patient is decongesting effectively (weight coming down, urine output adequate).
- Use IV furosemide, dose adequately (do not under-dose out of fear of creatinine), and monitor response at 6-12 hours.
- Stop or reduce only if: hemodynamic compromise appears, patient becomes clinically volume-depleted, or severe electrolyte derangement occurs.
Sources:
- National Kidney Foundation Primer on Kidney Diseases, 8e, pp. 331-332 (Therapeutic Strategies for Cardiorenal Syndrome)
- Harrison's Principles of Internal Medicine 22E, pp. 2025, 2036 (Cardiorenal interactions; ADHF management)
How do you assess response to furosemide and know when to uptitrate dose?
Finding Sources
Finding Sources
Searching PubMed
furosemide response assessment "urine sodium" "heart failure" uptitration
Finding Sources
Finding Sources
Searching PubMed
"urine sodium" diuretic "heart failure" decongestion natriuresis guided
Reading File
Reading Article
PMID: 39128947
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Excellent. I now have everything needed for a thorough answer.
Assessing Response to Furosemide and When to Uptitrate
There are two broad categories of assessment: traditional markers (output, weight) that take 24 hours to interpret, and emerging early markers (urine sodium, urine chemistry) that guide decisions within 2-6 hours.
1. Traditional Markers (24-Hour Assessment)
Daily Weight
- Target weight loss: 0.5-1.0 kg/day (up to 1.5 kg/day in severe congestion)
- Weighed at the same time each day (morning, after voiding, before eating)
- Limitation: Requires 24 hours before a dose-adjustment decision can be made, delaying decongestion therapy. Also an imperfect surrogate because venous capacitance can shift without actual weight change.
Net Fluid Balance (Ins and Outs)
- Strict hourly urine output measurement
- Target: negative net balance of 500-1000 mL/day in most patients
- Minimum urine output threshold: If output is <0.5 mL/kg/h or <30 mL/h several hours after the dose, this suggests inadequate response
- Same limitation as weight: decisions often delayed until end-of-day review
Clinical Decongestion Signs (Serial Examination)
- Falling JVP
- Reduction in peripheral edema, ascites
- Improvement in dyspnea, orthopnea
- Improving oxygen saturation / reduction in supplemental O2 requirement
- Clearing of pulmonary rales (less reliable than JVP)
2. Urine Chemistry - The Early Decision Tool (2-6 Hour Window)
This is the most important advance in monitoring and is now the preferred approach in expert centres. As the NKF Primer states: "Emerging data support the use of cumulative urine sodium output and sodium concentration in the first several hours following a diuretic dose as an effective means to more rapidly determine if a dose titration is warranted." - NKF Primer on Kidney Diseases, 8e, p. 331
Spot Urine Sodium at 2 Hours Post-Dose
| Result | Interpretation | Action |
|---|---|---|
| Spot uNa >50-70 mEq/L | Adequate natriuretic response | Continue current dose |
| Spot uNa <50 mEq/L | Inadequate response / diuretic resistance | Uptitrate or add agent |
| Spot uNa <30 mEq/L | Severe resistance | Double dose + consider adding metolazone |
- The Siddiqi et al. 2024 review summarises observational data linking low urine sodium excretion after IV furosemide to worse outcomes in ADHF, and multiple RCTs (ESCALATE, DECONGEST) have been designed around urine sodium-guided titration.
Fractional Excretion of Sodium (FENa) / Urine Creatinine Ratio
- FENa >0.2-0.3% after a furosemide dose suggests adequate tubular response
- Urine Na:Cr ratio (spot) also used in some protocols
3. When to Uptitrate the Dose
The dose-response curve for loop diuretics is logarithmic - doubling the dose is the correct stepwise strategy until response is achieved or maximal dose is reached. Comprehensive Clinical Nephrology, 7e, p. 1031
Uptitrate if ANY of the following at 6 hours:
- Urine output <100-150 mL/h
- Net fluid balance still positive
- Spot urine Na <50 mEq/L at 2 hours
- No appreciable symptomatic improvement
- Weight not falling
Practical uptitration algorithm:
Step 1: IV furosemide at 2.5x home oral dose (or 40-80 mg IV if diuretic-naive)
↓
Check urine Na at 2h, urine output at 6h
↓
Not responding? → Double the dose (logarithmic curve)
↓
Still not responding? (diuretic resistance)
↓
Step 2: Add metolazone 2.5-5 mg PO 30 min before next furosemide dose
("dual nephron blockade" - distal tubule blockade)
→ Monitor electrolytes closely (K, Mg)
↓
Still inadequate?
↓
Step 3: Add MRA (spironolactone) for proximal aldosterone-driven sodium retention
↓
Step 4: Consider SGLT2 inhibitor (emerging data for proximal nephron blockade in acute CRS)
↓
Step 5: Consider low-dose dopamine in refractory CRS (inconsistent evidence)
↓
Step 6: Ultrafiltration (last resort - no superiority shown over pharmacologic diuresis in CARESS-HF)
4. Biomarkers to Track During Diuresis
| Parameter | Frequency | What to Look For |
|---|---|---|
| Serum creatinine / eGFR | Daily | Acceptable: mild rise with active decongestion ("pseudoworsening"); Stop: creatinine rising >50% without decongestion or with clinical depletion |
| Serum K, Mg | Daily or BD | Hypokalemia/hypomagnesemia especially if adding thiazide |
| Serum Na | Daily | Hyponatremia may worsen with diuresis (dilutional or depletion) |
| BNP / NT-proBNP | Every 48-72h | Falling levels = successful decongestion |
| BP and HR | Continuous | Hypotension / tachycardia = volume depletion or haemodynamic deterioration |
5. Assessing Adequacy of Overall Decongestion (Discharge Target)
Decongestion should be the goal, not just "improved from baseline." Signs of adequate decongestion before stopping or de-escalating:
- JVP normalised (<4 cm above sternal angle)
- No orthopnoea, no peripheral oedema (or minimal)
- Target weight achieved (often 2-4 kg below admission weight)
- Spot urine Na improving
- BNP/NT-proBNP trending down (though not a hard cut-off)
- Stable or improving creatinine
The CRS Pathophysiology Context
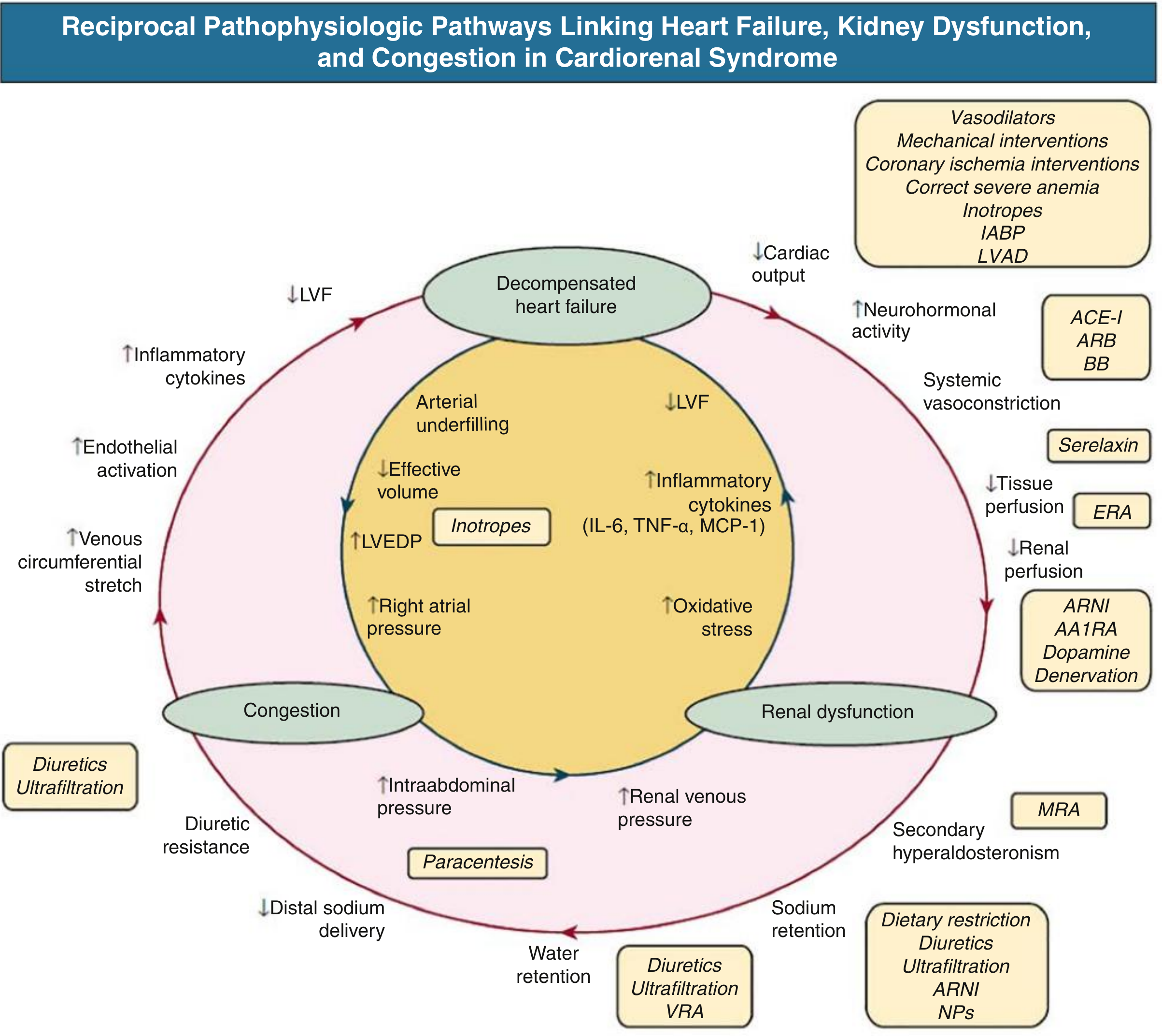
This diagram reinforces why adequate diuresis breaks the CRS cycle: it relieves renal venous pressure, reduces secondary hyperaldosteronism, lowers intraabdominal pressure, and ultimately improves GFR - which is why monitoring natriuresis (not just urine volume) is the most meaningful endpoint.
Bottom line: Check spot urine Na at 2 hours after the dose - it's the fastest and most reliable indicator of whether furosemide is working. If uNa <50 mEq/L, uptitrate by doubling the dose. If still inadequate after doubling, add metolazone. Use daily weight and net fluid balance as supporting 24-hour checkpoints.
This is a shared conversation. Sign in to Orris to start your own chat.