Nutritional anemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
"nutritional anemia" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to write a comprehensive, well-structured response. Here it is:
Nutritional Anemia
Nutritional anemia refers to anemia caused by inadequate intake or absorption of one or more essential nutrients required for red blood cell (RBC) formation. The three main culprits are iron, folate (folic acid), and vitamin B12 (cobalamin). These anemias are classified by RBC size (mean corpuscular volume, MCV).
Classification by RBC Size
| Type | MCV | Cause |
|---|---|---|
| Microcytic hypochromic | Below normal (<80 fL) | Iron deficiency |
| Macrocytic (megaloblastic) | Above normal (>100 fL) | Folate or Vitamin B12 deficiency |
"Nutritional anemias can be classified according to the size of the red blood cells (RBCs), or mean corpuscular volume (MCV). Microcytic anemia, caused by lack of iron, is the most common form of nutritional anemia." - Lippincott Illustrated Reviews: Biochemistry, 8th ed.
1. Iron Deficiency Anemia (IDA)
Epidemiology
IDA affects approximately 1.2 billion individuals worldwide - roughly half of all anemic persons. Prevalence is highest in:
- Preschool children (~25%)
- Young women (37-40%)
- Pregnant women (>40% with severe forms in low-income countries)
- Harrison's Principles of Internal Medicine, 22nd ed.
Causes
- Chronic blood loss (most important in high-income countries): GI sources (peptic ulcer, colon cancer, hemorrhoids), gynecologic (menorrhagia, endometrial cancer)
- Low dietary intake / poor bioavailability: Common in low-income countries; predominantly vegetarian diets; exclusively milk-fed infants; food insecurity
- Increased demand: Pregnancy, infancy, rapid growth
- Malabsorption: Celiac disease, various gastritides, post-gastrectomy
Pathophysiology (Sequence of Events)
Iron depletion develops in stages:
- Iron stores depleted first - serum ferritin falls, bone marrow macrophages lose stainable iron
- Serum iron falls, transferrin rises (TIBC increases)
- Transferrin saturation <15-20% - iron supply to erythropoiesis becomes insufficient
- Microcytic, hypochromic anemia develops
Maturing RBCs continue to divide past their normal stopping point due to insufficient hemoglobin, resulting in small, pale cells. The molecular explanation involves hepcidin - in iron deficiency, hepcidin levels are low, which normally would upregulate ferroportin to release iron from stores; mutations in TMPRSS6 (negative regulator of hepcidin) cause hereditary iron-refractory IDA (IRIDA).
Clinical Features
- Mild/asymptomatic in most cases
- Weakness, listlessness, pallor in severe cases
- Koilonychia (spooning of nails), thinning and flattening of nails in long-standing cases
- Pica - compulsion to eat non-food substances (dirt, clay, ice [pagophagia])
- Impaired cognitive performance, reduced immunocompetence
- In chronic heart failure: iron deficiency causes symptoms even independent of anemia
Laboratory Findings
| Test | IDA Finding |
|---|---|
| MCV | Low (microcytic) |
| MCHC | Low (hypochromic) |
| Serum ferritin | Low (falls first) |
| Serum iron | Low |
| TIBC | High |
| Transferrin saturation | Low (<15%) |
| Platelet count | Often elevated |
| Reticulocyte count | Low/normal |
- Robbins & Kumar Basic Pathology; Harrison's 22nd ed.
"Persons often die with iron deficiency anemia but virtually never of it. Microcytic hypochromic anemia is not a disease but rather a symptom of another underlying disorder." - Robbins & Kumar Basic Pathology
Treatment
- Oral iron (ferrous sulfate/gluconate/fumarate) is first-line
- IV iron preparations for malabsorption, intolerance, or non-response
- Treat the underlying cause (e.g., stop GI bleeding)
- Dietary advice: increase heme-iron foods; vitamin C enhances absorption; avoid tea/calcium with iron supplements
2. Megaloblastic Anemias (Folate and Vitamin B12 Deficiency)
Both folate and B12 are required for DNA synthesis. Deficiency causes accumulation of large, immature RBC precursors (megaloblasts) in the bone marrow and hypersegmented neutrophils in peripheral blood.
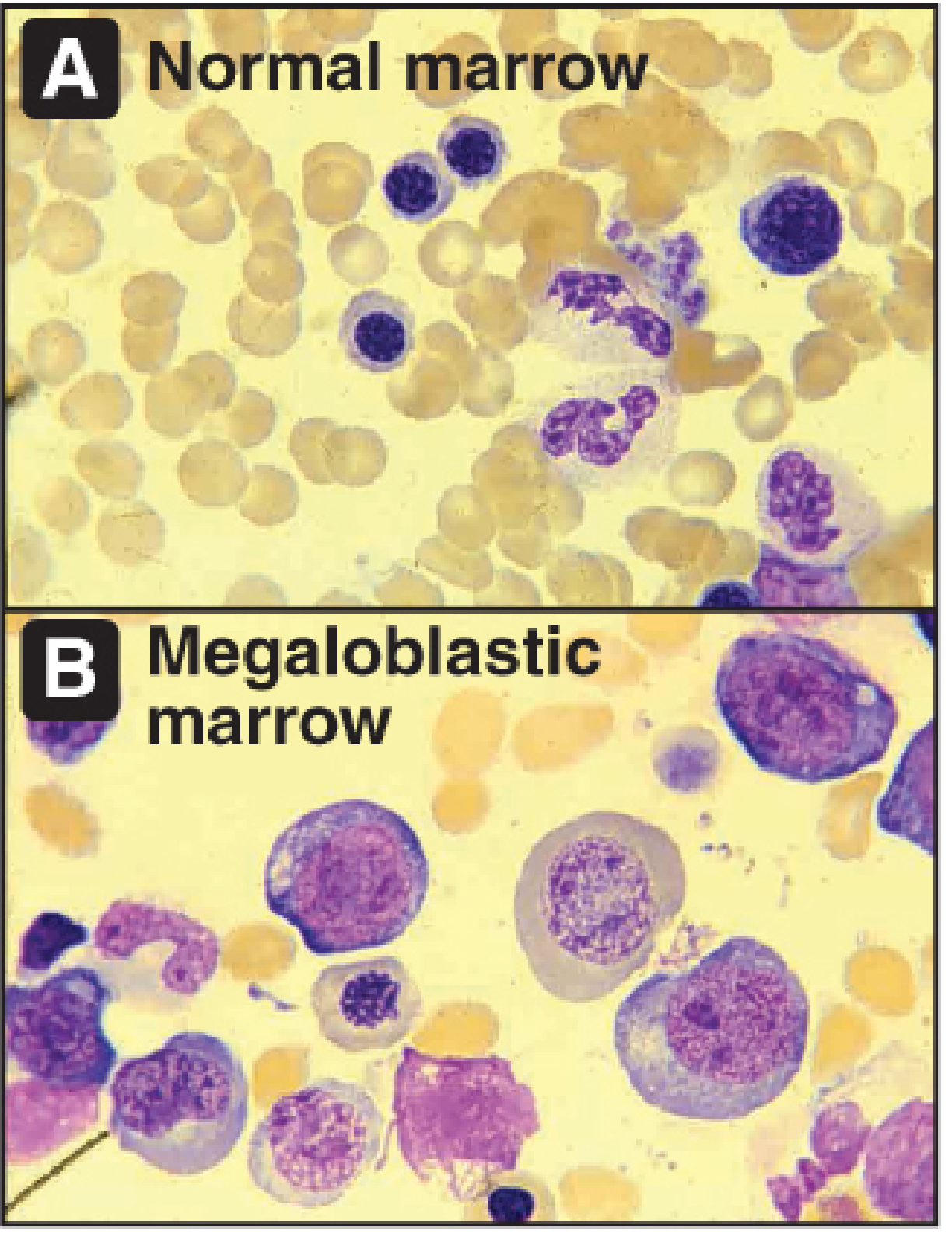
Bone marrow histology: Normal (A) vs. Megaloblastic (B) - Lippincott Illustrated Reviews: Biochemistry, 8th ed.
Mechanism
- Folate (as tetrahydrofolate, THF) transfers one-carbon units for synthesis of purine nucleotides and thymidine monophosphate (TMP) for DNA
- B12 is required to recycle THF - B12 deficiency "traps" folate as 5-methylTHF (the "methyl-folate trap"), making it metabolically unavailable for DNA synthesis
- Without DNA synthesis, nuclear division lags behind cytoplasmic maturation - cells become large and immature
A. Folate Deficiency
Causes:
- Increased demand: pregnancy and lactation (2nd most common nutritional anemia in pregnancy)
- Poor dietary intake (folate is found in leafy vegetables; cooking destroys it)
- Malabsorption: small intestine pathology
- Alcoholism (impairs absorption and increases demand)
- Drug-induced: methotrexate (dihydrofolate reductase inhibitor), trimethoprim, phenytoin
- Body stores are limited - a folate-free diet can cause deficiency within a few weeks
Key distinction from B12: Folate deficiency causes ONLY hematologic abnormalities, NOT neurologic damage.
Treatment: Oral folic acid (nontoxic, excreted in urine). Give before conception and during the first trimester to significantly reduce neural tube defects (spina bifida, anencephaly). The CDC recommends 400 mcg/day for reproductive-age women.
B. Vitamin B12 (Cobalamin) Deficiency
Absorption pathway (unlike folate, very complex):
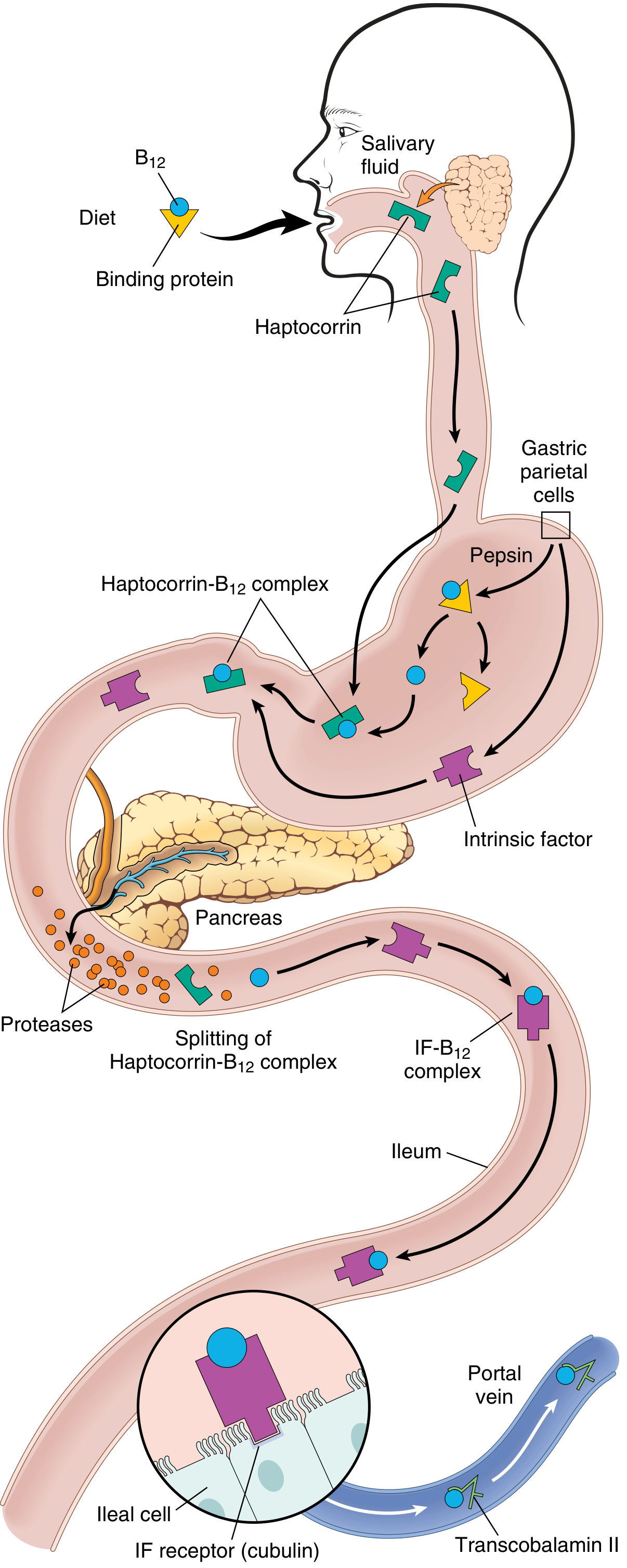
Vitamin B12 absorption - Robbins & Kumar Basic Pathology
- B12 freed from food by pepsin in stomach
- Binds haptocorrin (salivary protein)
- In duodenum, pancreatic proteases release B12 from haptocorrin
- B12 binds intrinsic factor (IF) - secreted by gastric parietal cells
- IF-B12 complex absorbed in terminal ileum via cubilin receptor
- Within ileal cells, B12 binds transcobalamin II for transport to liver and bone marrow
- Stored in liver - reserves last 5-20 years
Causes (almost always malabsorption, not dietary):
- Pernicious anemia (most frequent cause): autoimmune atrophic gastritis destroying parietal cells; autoantibodies block IF or IF-B12 binding to cubilin
- Gastrectomy (loss of IF-producing cells)
- Ileal resection or disease (Crohn disease, Whipple disease)
- Gastric atrophy/achlorhydria (elderly)
- Strict veganism (no animal products including milk/eggs) - the rare dietary cause
Clinical Features - unique to B12 deficiency:
- All the hematologic features of megaloblastic anemia PLUS
- Subacute combined degeneration of the spinal cord: demyelination of dorsal columns and lateral corticospinal tracts
- Tingling/paresthesias in hands and feet
- Difficulty walking, gait ataxia
- Dementia, cognitive impairment
- In extreme cases: hallucinations, paranoia, schizophrenic presentation
- Neurologic damage is IRREVERSIBLE if untreated
Treatment:
- Intramuscular hydroxocobalamin (preferred - rapid response, highly protein-bound, longer plasma levels)
- Oral/sublingual cyanocobalamin for dietary deficiency
- In pernicious anemia: therapy must be continued for life
- In bariatric surgery patients: daily sublingual or monthly parenteral B12
Critical Clinical Warning: Folate vs. B12
"If folate is given alone, it may reverse the hematologic abnormalities; however, the subsequent vitamin B12 deficiency could go on to cause neurologic complications." - Lippincott Illustrated Reviews: Pharmacology, 16th ed.
Rule: When megaloblastic anemia is suspected, empirical treatment should use both folate AND B12 until a full workup is complete.
Distinguishing B12 from Folate Deficiency
| Test | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Serum B12 | Low | Normal |
| Serum folate | Normal | Low |
| Methylmalonic acid (MMA) | High | Normal |
| Homocysteine | High | High |
| Neurologic signs | Present | Absent |
- MMA elevated + Homocysteine elevated = B12 deficiency
- MMA normal + Homocysteine elevated = Folate deficiency only
- Methylmalonic acid is the most sensitive and specific marker of B12 deficiency
- Goldman-Cecil Medicine; Lippincott Illustrated Reviews: Pharmacology
Summary Comparison Table
| Feature | Iron Deficiency | Folate Deficiency | Vitamin B12 Deficiency |
|---|---|---|---|
| MCV | Low (microcytic) | High (macrocytic) | High (macrocytic) |
| Peripheral smear | Hypochromic, microcytic | Megaloblasts, hyperseg. neutrophils | Megaloblasts, hyperseg. neutrophils |
| Neurologic signs | No | No | Yes |
| Ferritin | Low | Normal | Normal |
| MMA | Normal | Normal | Elevated |
| Homocysteine | Normal | Elevated | Elevated |
| Body stores | Months | Weeks | 5-20 years |
| Common in | Women of reproductive age, infants | Pregnancy, alcoholics | Elderly, strict vegans, pernicious anemia |
| Treatment | Oral/IV iron | Oral folic acid | IM hydroxocobalamin |
Sources: Lippincott Illustrated Reviews: Biochemistry 8th ed. | Basic Medical Biochemistry 6th ed. | Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine 22nd ed. | Lippincott Illustrated Reviews: Pharmacology 16th ed. | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.