Show the step-by-step view of a laparoscopic cholecystectomy, identifying Calot's triangle and the critical view of safety.
Reading File
Finding Sources
Finding Sources
Searching Images
laparoscopic cholecystectomy Calot's triangle critical view of safety
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Searching Images
laparoscopic cholecystectomy trocar port placement anatomy
Loading Image
Loading Image
Loading Image
Searching Images
clipping cystic duct artery laparoscopic cholecystectomy clips
Loading Image
Loading Image
I now have rich textbook content and intraoperative images to construct a comprehensive step-by-step guide. Let me compile the full answer.
Laparoscopic Cholecystectomy: Step-by-Step with Calot's Triangle & Critical View of Safety
First described by Muhe (1985) and popularized by Mouret (1987), laparoscopic cholecystectomy is now the gold standard for symptomatic gallbladder disease. It carries 0.1–0.5% mortality and 2–3% morbidity. — Sabiston Textbook of Surgery, p. 1839
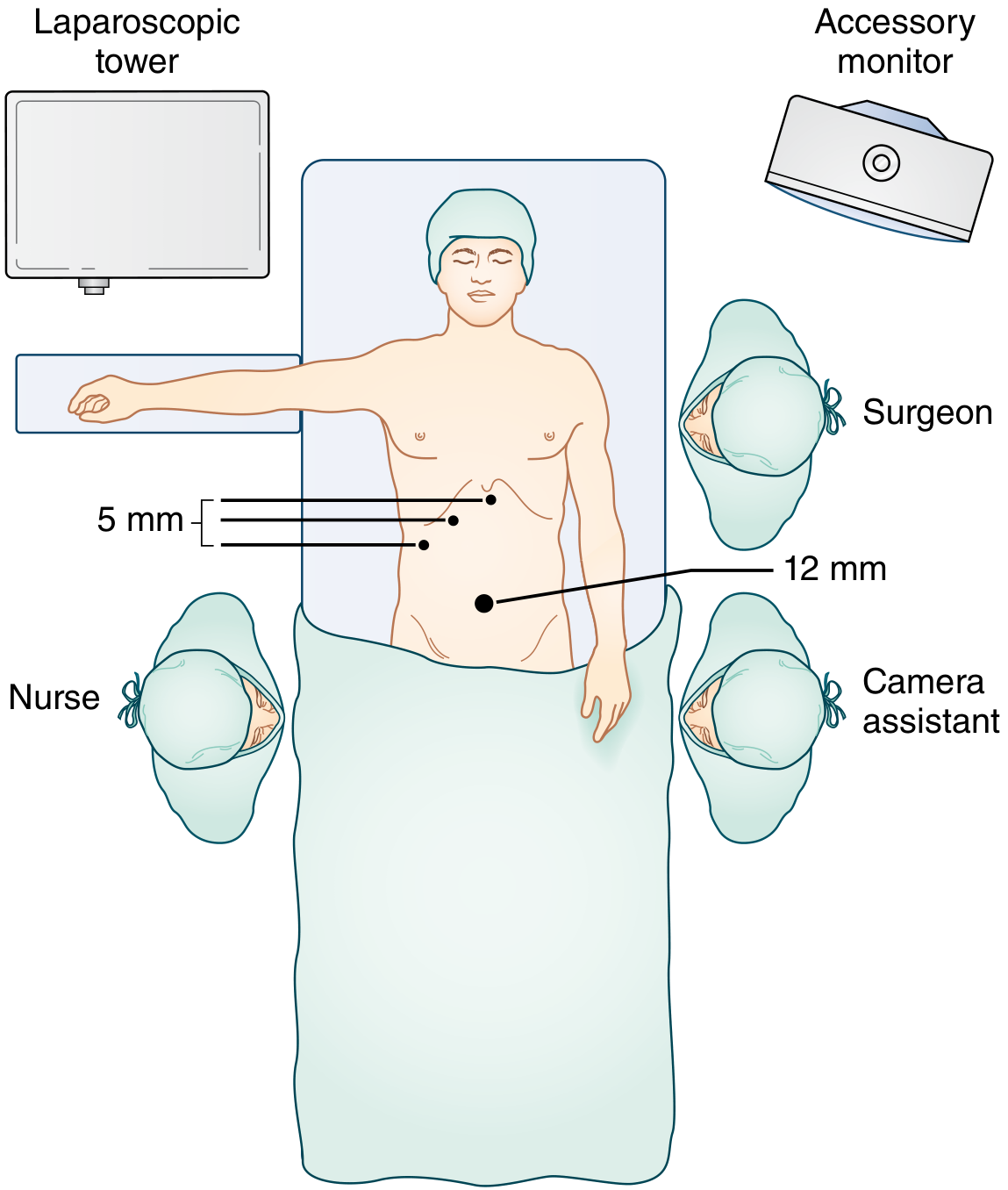
Step 1 — Patient Positioning & Setup
- Position: Supine, one arm tucked (to allow intraoperative cholangiogram access if needed)
- Bed: Patient well secured for steep reverse-Trendelenburg positioning — gravity drops bowel away from the operative field
- Prep/drape: Lower chest to abdomen, prepared to accommodate conversion to open if needed
- An orogastric tube decompresses the stomach for better upper-abdominal visualization
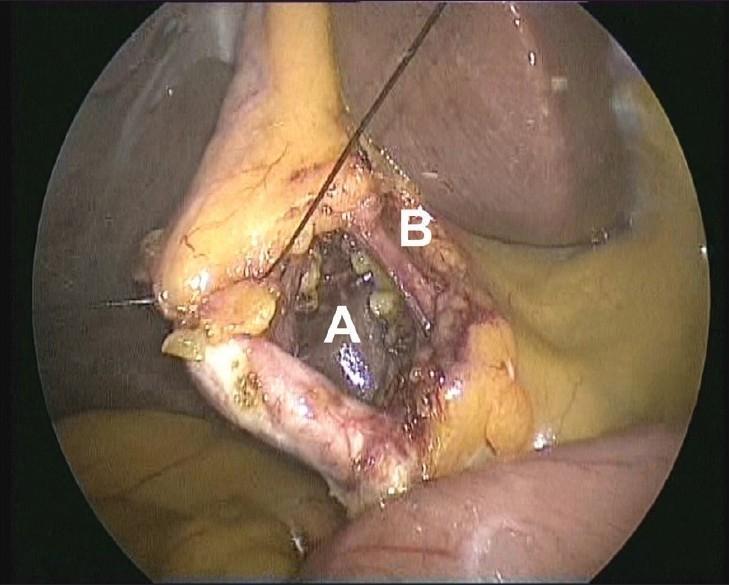
Step 2 — Port Placement (Standard 4-Port Configuration)
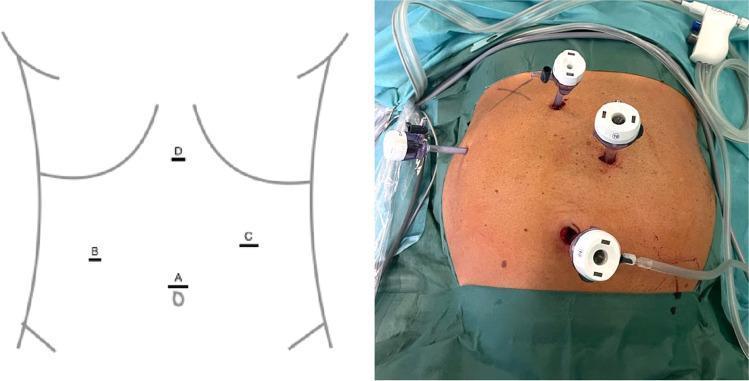
| Port | Size | Location | Role |
|---|---|---|---|
| A | 12 mm | Periumbilical | Camera + specimen extraction |
| B | 5 mm | Right midclavicular line | Grasps infundibulum (inferolateral retraction) |
| C | 5 mm | Right anterior axillary line | Elevates fundus cephalad |
| D | 5 mm | Subxiphoid | Surgeon's dissecting instrument |
Pneumoperitoneum is established (typically to 12–15 mmHg CO₂) before port insertion. The patient is placed in steep reverse-Trendelenburg to move the transverse colon and duodenum away from the operative field. — Sabiston Textbook of Surgery, p. 1839
Step 3 — Gallbladder Retraction & Exposure
- The lateral port grasper elevates the fundus cephalad toward the right shoulder — this opens the porta hepatis and stretches the cystic structures
- The midclavicular port grasper retracts the infundibulum/Hartmann's pouch inferolaterally — this is the key maneuver that unfolds the triangle of Calot and puts the cystic duct under tension
- If the gallbladder is tense/distended (acute cholecystitis), decompression via needle aspiration through the fundus is performed first
- Adjacent structures (omentum, duodenum, colon) that are adherent to the gallbladder are gently peeled off bluntly in a plane parallel to the gallbladder wall
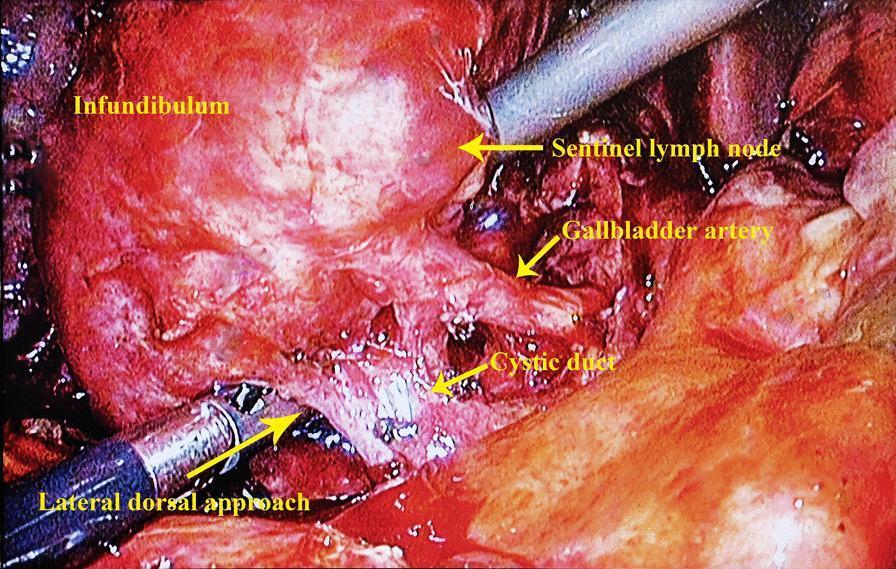
Step 4 — Anatomy of Calot's Triangle
Calot's triangle (hepatocystic triangle) is the key anatomical space targeted during dissection:
| Boundary | Structure |
|---|---|
| Superior | Inferior surface of the liver |
| Medial | Common hepatic duct |
| Lateral/inferior | Cystic duct |
Contents: Cystic artery, Calot's lymph node (sentinel node — lies directly on top of the cystic artery and serves as a landmark for it), lymphatics, and areolar/fibrofatty tissue.
The Calot node is the most reliable intraoperative landmark for the cystic artery. Limiting peritoneal division to the gallbladder side of this node minimizes CBD injury risk. — Sabiston Textbook of Surgery, p. 1839
Step 5 — Dissection of the Hepatocystic Triangle
- Using a Maryland dissector or hook, the peritoneum overlying both the anterior and posterior aspects of the hepatocystic triangle is scored and dissected
- The fibrofatty and areolar tissue within the triangle is cleared away
- Dissection is kept high on the gallbladder wall (at the infundibulum), not deep into the porta hepatis
- The goal is to skeletonize the two structures that enter the gallbladder: the cystic duct and cystic artery
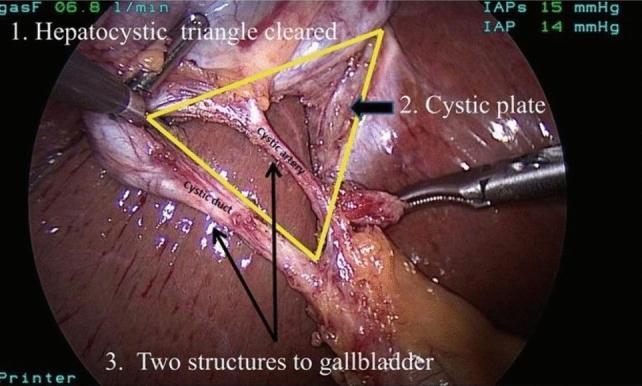
Step 6 — Critical View of Safety (CVS)
The Critical View of Safety (CVS) is the mandatory safety checkpoint before any structure is clipped or divided. It was formalized by Strasberg et al. to prevent bile duct injury (BDI).
Three criteria — ALL must be met simultaneously:
| # | Criterion |
|---|---|
| 1 | Hepatocystic triangle is completely cleared of fibrofatty and areolar tissue |
| 2 | Lower one-third of the gallbladder is dissected free from the liver (cystic plate exposed) |
| 3 | Only two structures are seen entering the gallbladder |
"Critical view of safety is defined as two and only two structures entering the gallbladder, the lower third of the gallbladder dissected from the liver to expose cystic plate, and a cleared hepatocystic triangle." — Sabiston Textbook of Surgery, p. 1839
Why CVS matters: Bile duct injury is the most feared complication of cholecystectomy (~0.3–0.5%). The most common mechanism is misidentification of the CBD as the cystic duct. CVS ensures no structure is clipped until it is unambiguously confirmed to connect only to the gallbladder — not to the biliary confluence.
Step 7 — Clipping and Division
Once CVS is confirmed:
- A clip applier places 2 clips proximally (toward the patient — away from gallbladder) and 1 clip distally on the cystic duct, then transects between
- Similarly, 2 proximal + 1 distal clip on the cystic artery, then transected
- Key technical tip: ensure both jaws of the clip applier are fully visible before closing — prevents incomplete occlusion
Step 8 — Gallbladder Dissection from Liver Bed
- The gallbladder is dissected off the cystic plate (liver bed) using electrocautery (hook or spatula)
- Dissection proceeds from infundibulum toward fundus in a "top-down" (retrograde) manner
- Venous drainage from the gallbladder goes directly into the liver bed through venules — meticulous hemostasis is required
- Just before completing fundic dissection, the clip sites on the cystic duct and artery are re-inspected (the superior traction of the fundus at this stage provides an excellent final view of the porta hepatis)
Step 9 — Specimen Retrieval & Closure
- The gallbladder is placed into a specimen retrieval bag inside the abdomen
- Extracted through the umbilical (12-mm) port, enlarged if needed
- Any spilled stones must be retrieved — left-behind stones can cause late perihepatic abscess
- Ports are removed under vision, pneumoperitoneum deflated, fascia closed at the 12-mm site, skin closed
Adjuncts: When Anatomy Is Uncertain
| Adjunct | Indication |
|---|---|
| Intraoperative cholangiogram (IOC) | Unclear anatomy, suspected CBD stones, anomalous biliary tree |
| Fluorescent cholangiography (ICG) | Real-time biliary anatomy — ICG IV 30–60 min preop; fluoresces green under near-infrared light; may be limited by inflammation/obesity |
| Conversion to open | Cannot achieve CVS safely; uncontrolled hemorrhage; CBD injury identified |
Bailout Strategies When CVS Cannot Be Achieved
When dense inflammation (e.g., gangrenous cholecystitis, Mirizzi syndrome) prevents safe dissection:
- Subtotal cholecystectomy — partial resection leaving the posterior wall adherent to the liver; cystic duct orifice closed from within
- Fundus-first (dome-down) approach — dissect from fundus toward infundibulum when the neck is too inflamed
- Cholecystostomy tube — drain first, operate electively 6–8 weeks later
Sources: Sabiston Textbook of Surgery, 21st ed., p. 1839 | Current Surgical Therapy, 14th ed., p. 506–507 | Intraoperative images from PMC clinical surgical literature.
This is a shared conversation. Sign in to Orris to start your own chat.