Platellar tendonitis treatment
"patellar tendinopathy" AND treatment
patellar tendonitis treatment guidelines 2024 2025
PMID: 40421598
PMID: 40666246
PMID: 40215473
Patellar Tendonitis (Patellar Tendinopathy) - Treatment
1. Diagnosis Essentials
- Pain at the inferior pole of the patella, worsened by activity (stairs, squatting, jumping)
- Tenderness on direct palpation of the tendon
- Plain X-rays: rule out avulsion fracture or patella alta
- MRI or ultrasound: confirm diagnosis in uncertain cases
- Red flags - palpable defect, inability to straight-leg raise - suggest rupture, not tendinopathy
2. Conservative Management (First-Line)
Relative Rest
- Reduce aggravating activity (not complete immobilization)
- Offload the tendon during the acute/painful phase
NSAIDs
- Short-term use to reduce pain and inflammation
- Useful in the early, symptomatic phase
Physical Therapy - Exercise Rehabilitation (Cornerstone)
| Exercise Type | Role | Evidence |
|---|---|---|
| Eccentric loading (e.g., decline squat, single-leg squat lowering) | Best for long-term pain reduction and functional improvement | Grade A (multiple RCTs) |
| Isometric loading (e.g., wall sits, leg press holds) | Best for short-term/in-season pain relief, especially during sport | Grade A |
| Concentric-eccentric | Progressive strengthening for later rehab phases | Moderate evidence |
- Decline squat: 3 sets x 15 reps, twice daily, 12 weeks
- Progress by adding load (holding dumbbells) once pain-free
Stretching
- Quadriceps and hamstring flexibility work - adjunct to strengthening
3. Adjunct / Intermediate Therapies
| Therapy | Notes |
|---|---|
| Patellar tendon strap/brace | Offloads the tendon insertion; symptom relief during sport |
| Dry needling | Promising for pain reduction; high-quality trials show benefit (Grade A, 1B evidence) |
| PRP (Platelet-Rich Plasma) | Increasingly used; evidence emerging but not yet definitive |
| Shockwave therapy (ESWT) | Moderate evidence for refractory cases; stimulates tendon remodeling |
| Pulsed ultrasound / Transverse friction massage | Evidence is weak vs. exercise |
Steroid (glucocorticoid) injection: NOT recommended. Rosen's Emergency Medicine explicitly states there is no role for steroid injection in patellar tendinopathy. Cochrane data also shows it is not superior to exercise.
4. Surgical Treatment (Refractory Cases)
- Arthroscopic or open debridement of the tendon (removal of degenerative tissue)
- Percutaneous needle tenotomy (ultrasound-guided)
- Tendon scraping / longitudinal tenotomy
- VISA-P scores improved by ~40 points post-surgery
- VAS pain scores dropped by 6.1 points
- Return-to-play rate: 87%
5. Return to Sport - Timeline (General Guide)
| Phase | Timeframe | Goals |
|---|---|---|
| Acute | Weeks 1-2 | Pain control, relative rest, isometrics |
| Sub-acute | Weeks 2-6 | Progressive eccentric loading, flexibility |
| Strengthening | Weeks 6-12 | Heavy slow resistance, sport-specific conditioning |
| Return to sport | 3-6 months | Full load tolerance, pain-free throughout |
Key Takeaways
- Eccentric strengthening is the backbone of treatment - start it early and do it consistently
- Isometric holds are especially useful for in-season athletes who cannot rest
- No steroids - they do not help and may worsen tendon structure
- Surgery works well when conservative care fails (~87% return to sport)
Give a image
Medical diagram of patellar tendonitis (jumper's knee) showing anatomy of the knee with the patellar tendon highlighted and inflamed, labels pointing to patella, patellar tendon, tibial tuberosity, site of pain and inflammation, and inset showing microscopic microtears in the tendon. Clean clinical illustration style.
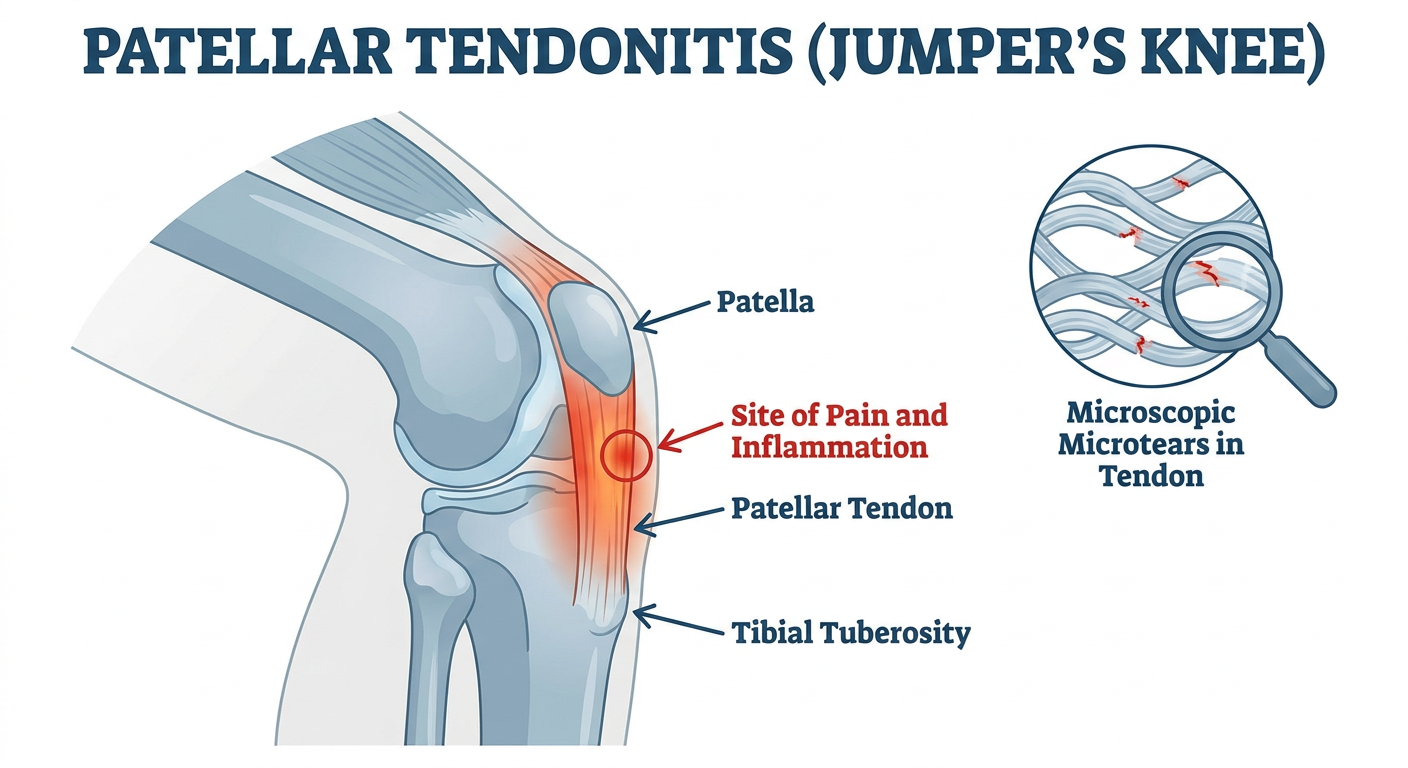
- Patella - the kneecap, sitting at the top of the tendon
- Patellar tendon - connects the patella to the tibial tuberosity; the site of injury
- Tibial tuberosity - the bony prominence on the shin where the tendon inserts
- Inflammation zone - typically at the inferior pole of the patella (where the tendon originates)
- Microtears - microscopic damage within the tendon from repetitive loading, which drives the chronic pain cycle
Image of physiotherapy
Physiotherapy session for patellar tendonitis treatment showing a physical therapist working with a patient on knee rehabilitation exercises, including eccentric squats on a decline board, isometric holds, and stretching. Clinical physiotherapy gym setting with exercise equipment. Professional medical illustration style.
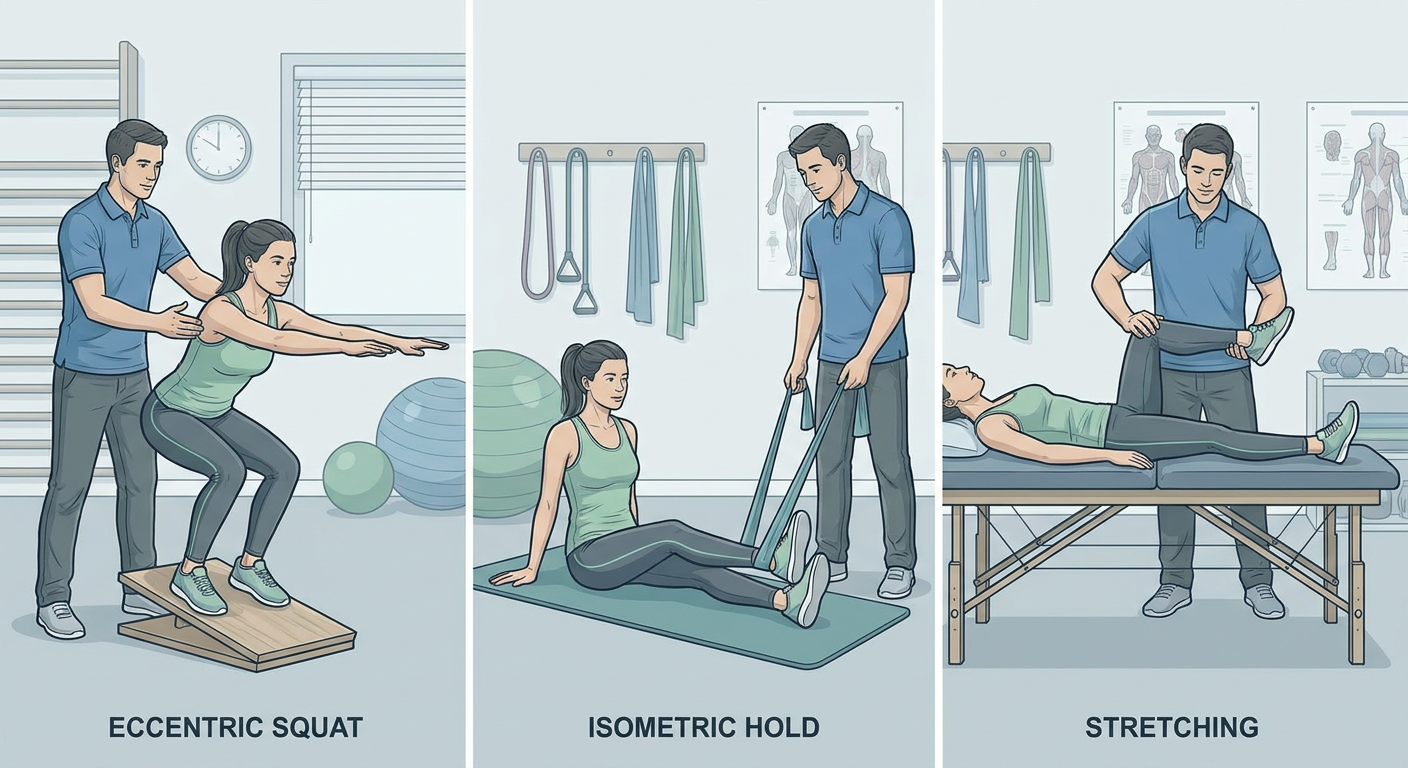
- Decline squat (eccentric loading) - the gold-standard exercise; performed on a slanted board to maximally load the patellar tendon during the lowering phase
- Isometric holds - static quad contractions (e.g., wall sits) for short-term pain relief, especially useful during the in-season period
- Therapist-guided manual therapy - soft tissue work and guided joint mobilization
- Progressive strengthening - advancing from bodyweight to weighted exercises over 6-12 weeks