Radiology detailed overview
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Now I have thorough material from Grainger & Allison's Diagnostic Radiology to compose a detailed, well-structured overview.
Radiology: A Detailed Overview
Source: Grainger & Allison's Diagnostic Radiology - A Textbook of Medical Imaging
1. What is Radiology?
Radiology (diagnostic imaging) is the medical specialty that uses various forms of energy - primarily electromagnetic radiation, sound, and magnetic fields - to create images of the human body for the purpose of diagnosis, disease monitoring, and procedural guidance. It sits at the intersection of physics, anatomy, pathology, and clinical medicine.
2. The Major Imaging Modalities
2.1 Plain Radiography (X-Ray)
Chest radiography remains the single most commonly performed diagnostic radiographic procedure. The basic principle involves passing x-ray photons through the body and detecting differential attenuation by tissues of varying density.
Digital Imaging Systems:
| System | Mechanism | Notes |
|---|---|---|
| Computed Radiography (CR) | Photostimulable phosphor plate | Older; still used in some departments |
| Direct Radiography (DR) - Direct | Photoconductors (e.g., amorphous selenium) in flat-panel detectors | Most modern standard |
| Direct Radiography (DR) - Indirect | Scintillator + CCD or flat-panel detector | Thallium-doped caesium iodide or gadolinium-based |
Both CR and DR offer wider latitude (fewer retakes), reusable detectors, and seamless integration with PACS (Picture Archiving and Communication Systems).
Standard Projections:
- Posteroanterior (PA) and lateral views suffice for most purposes
- Portable/AP radiography used in critically ill patients (has technical limitations vs. PA - magnification, lack of inspiration control, overlying tubes/lines)
- Lateral decubitus - detects small pleural effusions (>10 mL)
- Lordotic view - visualises lung apices without rib overlap
Novel Techniques:
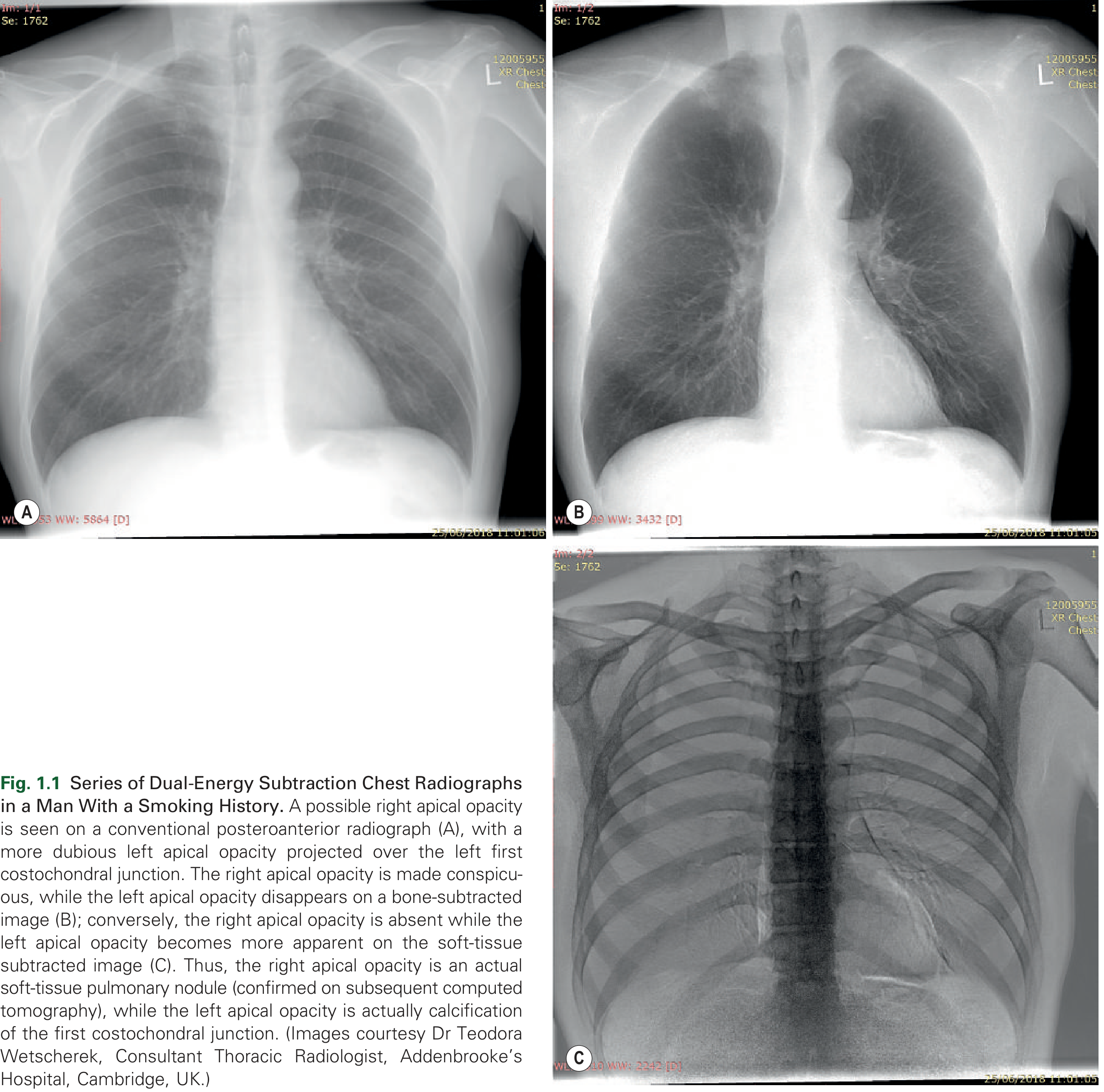
- Dual-energy subtraction (DES): Two acquisitions at different kV exposures, digitally subtracted to produce separate bone- and soft-tissue images, improving lesion conspicuity (see image below)
- Tomosynthesis: Multiple low-dose projections reconstructed as tomographic slices, improving lesion detection vs. conventional radiography
2.2 Computed Tomography (CT)
CT uses rotating x-ray beams and multiple detector arrays to reconstruct cross-sectional images. It is the dominant tool for thoracic, abdominal, and vascular imaging.
From Single-Slice to Multidetector CT (MDCT)
- Spiral (helical) CT was introduced in the early 1990s - replaced sequential single-slice acquisition with volumetric data
- 1998: First multidetector (MDCT) systems launched
- Modern systems: up to 320 active detector rows, rotation times as low as 0.33 seconds/rotation
- Enables single breath-hold whole-thorax imaging, reduces motion artefacts (particularly important in paediatrics), and produces isotropic voxel data for 3D reconstruction
Reconstruction Algorithms (Kernels/Filters)
| Algorithm Type | Properties | Use |
|---|---|---|
| Low spatial resolution | Reduces noise, improves contrast | Soft tissue, vascular imaging |
| High spatial resolution ("lung"/"sharp") | Enhances fine detail, increases noise | Airway, interstitial lung disease, pulmonary nodules |
Window Settings
- Lung windows: Wide windows, low centre - visualise lung parenchyma
- Mediastinal windows: Narrow windows, higher centre - soft tissue/vessel detail
- Manual window adjustment is needed (e.g., when contrast appears too dense and may obscure a pulmonary embolus)
Slice Thickness and Clinical Use
- Narrow sections (0.6-1.25 mm): High-resolution; for nodule characterisation, interstitial lung disease, pulmonary embolism
- Wide sections (2.5-5 mm): Better contrast; mediastinal masses, quick review, lung cancer staging
CT Postprocessing Techniques
| Technique | Principle | Clinical Application |
|---|---|---|
| MPR / CMPR | 2D alternate viewing planes | Large airway evaluation, pulmonary embolism |
| Maximum Intensity Projection (MIP) | Only highest-density voxels displayed | Perivascular and micronodular disease assessment |
| Minimum Intensity Projection (MiniP) | Lowest-density voxels displayed | Emphysema, air trapping |
| Shaded Surface Display (SSD) | Threshold-based surface rendering | Airway abnormalities |
| Volume Rendering | Full histogram-based 3D | Angiography, large airway evaluation |
| Virtual Bronchoscopy | Endoscopic simulation | View airway distal to obstructing lesion |
| Computer-Aided Detection (CAD) | Automated pattern recognition | Pulmonary nodule detection and volumetry |
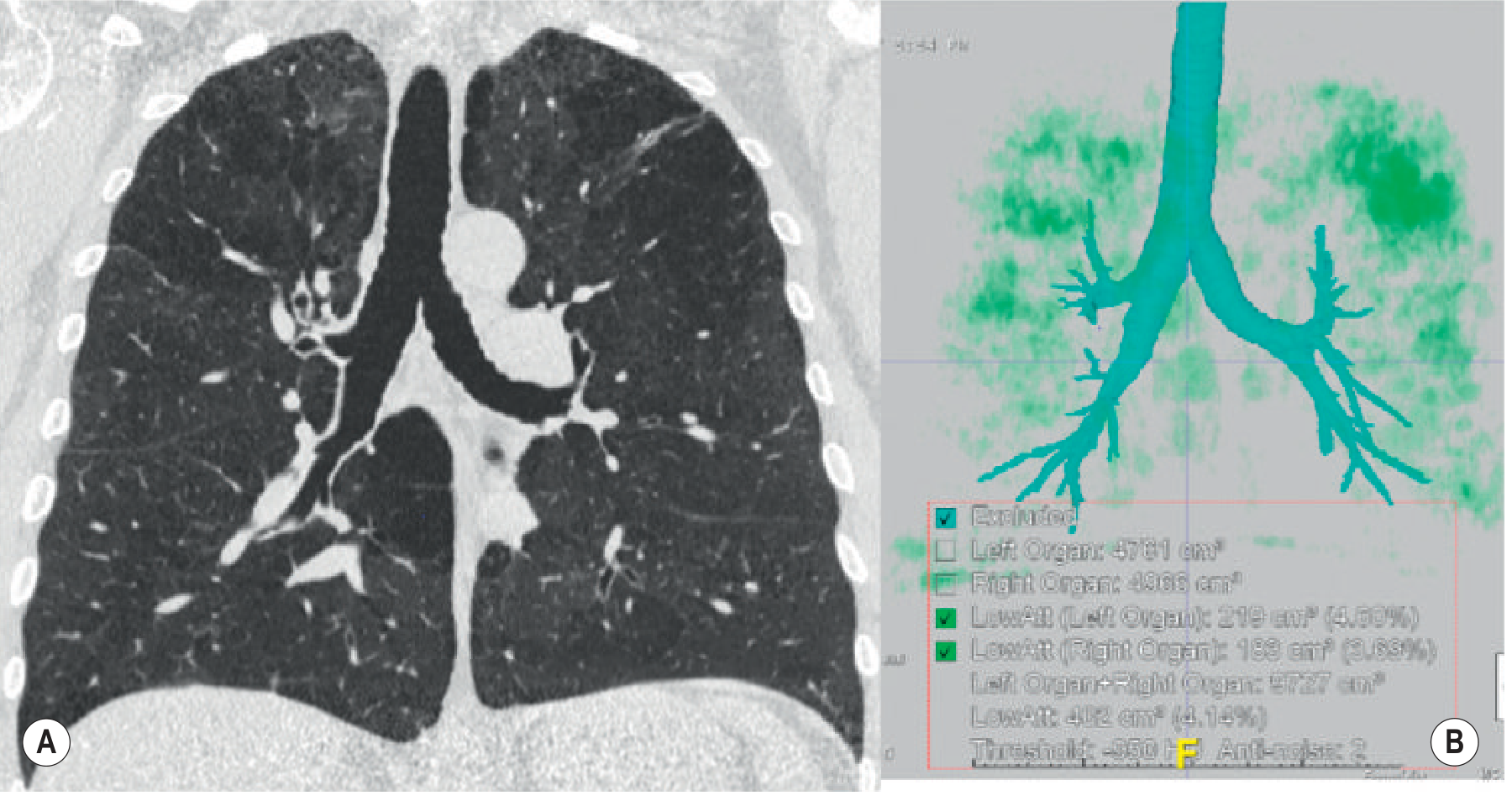
| Quantitative Parenchyma Analysis | Density masks + histogram analysis | Emphysema quantification |
Dual-Energy CT (DECT)
DECT acquires data at two different tube energies simultaneously. Key applications:
- Pulmonary blood volume maps: Surrogate for lung perfusion - identifies perfusion defects in acute/chronic pulmonary embolism
- Virtual unenhanced imaging: Eliminates need for a separate pre-contrast acquisition when evaluating pulmonary nodule enhancement
- Iodine mapping: Differentiates iodinated contrast from calcium/haemorrhage
Dose Reduction Strategies
- Iterative reconstruction (IR): Default in modern CT systems. IR reduces image noise significantly, allowing diagnostically comparable images at lower doses. Especially important in CT lung cancer screening and paediatric patients
- Automatic tube current modulation
- Low kV protocols for vascular studies
2.3 Ultrasound (US)
Key advantages: No ionising radiation, bedside availability, real-time imaging, guidance for procedures.
Probe Selection:
- High-frequency linear probe (5-7.5 MHz): Chest wall evaluation
- Sector/phased-array probe (3.5 MHz): Pleural and pulmonary disease
Clinical applications in thoracic imaging:
- Pleural effusion - detects small effusions missed on supine radiographs; identifies septations and echogenicity (suggestive of exudate)
- Guided aspiration/drainage - guides thoracocentesis for both simple and loculated collections
- Pneumothorax detection (especially in ICU/supine patients):
- Loss of lung sliding
- Presence of the "lung point" on B- and M-mode (pathognomonic - intermittent visualisation of collapsed lung sliding into view at the pneumothorax border)
- Accentuated reverberation artefacts (A-lines)
- Absent/decreased comet-tail artefacts (B-lines)
- "Stratosphere" sign on M-mode (replaces normal "seashore" sign)
- Alveolar recruitment assessment in ventilated ICU patients with severe respiratory failure
- Endoscopic/Endobronchial Ultrasound (EUS/EBUS): Cornerstone of mediastinal node staging in lung cancer; allows real-time guided needle biopsy of mediastinal lymph nodes and peri-oesophageal structures
2.4 Magnetic Resonance Imaging (MRI)
MRI exploits the behaviour of hydrogen nuclei in strong magnetic fields. It offers excellent soft-tissue contrast and carries no ionising radiation.
Limiting factors in thoracic MRI (historically):
- Low signal-to-noise ratio (lung has few protons)
- Respiratory and cardiac motion artefacts
- Very short T2* decay from heterogeneous magnetic susceptibility at pulmonary interfaces
Technical solutions:
- Single-shot techniques (HASTE, FASE): Entire k-space filled in one breath-hold; yields T2-weighted images
- 3D GRE sequences (VIBE): T1-weighted, fast, with or without fat saturation
- Respiratory triggering + ECG gating: Mitigates motion
- Navigator echoes: Track diaphragmatic motion for respiratory triggering
Established Thoracic MRI Indications:
| Indication | MRI Advantage |
|---|---|
| Cystic vs. solid mediastinal lesion | T2 confirms cystic nature (high signal) even when CT density is elevated |
| Diaphragmatic invasion by pleural mesothelioma | Gadolinium T1 outperforms CT |
| Anterior mediastinal lesion characterisation | Chemical shift imaging identifies fat (vs. recurrent malignancy) |
| Nodal staging in NSCLC | STIR sequences may outperform FDG-PET |
| Thymic hyperplasia vs. malignancy | Fat saturation + chemical shift imaging |
Emerging MRI Techniques:
- UTE/ZTE sequences: Allow lung parenchyma imaging by capturing very short T2* signal - previously impossible
- Diffusion-Weighted Imaging (DWI): Evaluates tumour cellularity (best for lymphoma, small cell lung cancer); differentiating histological subtypes in mesothelioma
- Hyperpolarised gas MRI (³He, ¹²⁹Xe): Reveals subclinical ventilation defects in obstructive lung disease with far greater sensitivity than spirometry; also provides semiquantitative alveolar volume and surface area measurement
2.5 Radionuclide Imaging (Nuclear Medicine)
Radionuclide imaging detects gamma rays emitted by radiopharmaceuticals that are taken up by specific tissues based on their physiological activity.
Ventilation-Perfusion (V/Q) Scintigraphy
- Ventilation: Inhaled radiolabelled aerosol or gas (e.g., ⁹⁹ᵐTc-DTPA aerosol, ¹³³Xe)
- Perfusion: IV injection of ⁹⁹ᵐTc-labelled macroaggregated albumin (MAA) - particles lodge in pulmonary capillaries proportional to flow
- Main use: Diagnosis of pulmonary embolism (PE), especially when CT is contraindicated (renal impairment, contrast allergy, pregnancy - lower radiation to gonads)
- Interpreted using PIOPED II criteria
PET and PET-CT
- PET: Detects positron-emitting radiotracers (primarily ¹⁸F-FDG - fluorodeoxyglucose), exploiting the Warburg effect (increased glucose uptake in metabolically active/malignant tissue)
- PET-CT fusion: Combines metabolic information (PET) with anatomical detail (CT) in a single examination
- Established roles:
- Lung cancer staging (N and M staging, detecting unsuspected extrathoracic metastases)
- Differentiating malignant from benign pulmonary nodules
- Assessing treatment response
- Staging lymphoma
- Evaluation of solitary pulmonary nodule (SUV >2.5 suspicious for malignancy)
- Limitations: False positives in active infection/inflammation (e.g., sarcoid, aspergillosis); false negatives in low-metabolic tumours (carcinoid, BAC/AIS)
3. Normal Radiological Anatomy of the Chest
The Lungs and Hila
- The trachea is a midline structure, slightly deviated to the right at the carina. Its right lateral wall forms the right paratracheal stripe (width <4 mm on PA film)
- The carina angle is normally <70°. Widening suggests left atrial enlargement
- Hilar shadows on CXR are predominantly formed by the pulmonary arteries (not lymph nodes). The left hilum is higher than the right in ~97% of patients
- Lung markings extend to the pleural surface; absence suggests pneumothorax
The Mediastinum
Compartments (traditional Felson classification on lateral CXR):
| Compartment | Contents | Key Lesions |
|---|---|---|
| Anterior | Thymus, fat, lymph nodes, great vessels | Thymoma, teratoma, lymphoma, thyroid mass ("4 Ts") |
| Middle | Heart, pericardium, great vessels, trachea, oesophagus | Pericardial cysts, bronchogenic cysts, lymphadenopathy |
| Posterior | Descending aorta, thoracic duct, sympathetic chain, neural foramina | Neurogenic tumours, aortic aneurysm |
Key mediastinal lines and stripes (PA CXR):
- Right paratracheal stripe: <4 mm; widening = lymphadenopathy, thyroid, right-sided aortic arch
- Azygo-oesophageal recess: Concave interface; convexity = subcarinal lymphadenopathy, oesophageal lesion
- Paraspinal lines: Paravertebral soft tissue; widening = haematoma, lymphoma, abscess, aneurysm
- Retrosternal line (lateral view): Anterior mediastinal mass obliterates retrosternal airspace
The Pleura
Normal pleura is not visualised on CXR. The visceral and parietal layers are separated by a few mL of lubricating fluid.
Pleural Effusion - Imaging Findings:
Chest Radiograph:
- PA erect: Blunting of costophrenic angle (>200 mL), meniscus sign, opacification
- Supine (ICU): Haziness of hemithorax (layering fluid) - may be missed
- Subpulmonary effusion: Apparent elevation of hemidiaphragm; distance between lung base and gastric bubble >2 cm (left side)
Ultrasound: Most sensitive for small effusions; identifies septations (suggests exudate/empyema); guides safe aspiration
CT: Fluid attenuation (0-30 HU = transudate; 30-60 HU = exudate/haemothorax); pleural enhancement = empyema; nodular pleural thickening = malignancy
PET-CT: FDG-avid pleural thickening suggests malignant mesothelioma or pleural metastasis
The Diaphragm
- Right hemidiaphragm sits at the anterior end of the right 6th rib; left is ~1.5 cm lower (due to gastric bubble)
- Eventration vs. true paralysis: fluoroscopy (sniff test) - paradoxical movement indicates paralysis
- Diaphragmatic humps (focal elevation): Most commonly Morgagni or Bochdalek hernias, or anterior fat pad
4. Key Radiological Patterns and Their Significance
Airspace (Alveolar) Opacification
Fluffy, confluent, ill-defined opacity with air bronchograms.
- Causes: Pneumonia, pulmonary oedema, haemorrhage, aspiration, alveolar proteinosis
- Distribution matters: Perihilar/bilateral (oedema), unilateral/segmental (pneumonia)
Interstitial Patterns
Fine reticulation, honeycombing, ground-glass opacity - seen on HRCT:
- Ground-glass opacity (GGO): Partial airspace filling; causes include early oedema, pneumocystis, NSIP, atypical pneumonia, COVID-19
- Reticulation: Thickened interlobular septa; IPF, sarcoid, lymphangitic carcinomatosis
- Honeycombing: Destroyed lung architecture in UIP/IPF pattern; subpleural, basal predominant
- Crazy paving: GGO + thickened septa; pulmonary alveolar proteinosis (classic), COVID-19, ARDS
Air Trapping and Emphysema
CT findings:
- Centrilobular emphysema: Focal areas of low attenuation around centrilobular arteriole; smoking-related, upper lobe predominance
- Panlobular emphysema: Uniform destruction of acinus; alpha-1 antitrypsin deficiency, lower lobe predominance
- Paraseptal emphysema: Subpleural, often bullous; associated with spontaneous pneumothorax in young men
- Air trapping: Seen on expiratory CT as persistent low-attenuation lobules (obliterative bronchiolitis, asthma)
Pulmonary Nodules
Management follows Fleischner Society and BTS/BSTI guidelines based on size, morphology, and patient risk:
- Spiculated/irregular border: High risk for malignancy
- Smooth, well-defined, <6 mm: Very low malignancy risk
- Calcification patterns: Popcorn (hamartoma), central/laminar (granuloma - benign), eccentric (potentially malignant)
- Ground-glass nodule: May represent adenocarcinoma-spectrum lesion (AIS/MIA); requires long-term follow-up
5. Interventional Radiology (IR)
Interventional radiology uses imaging guidance (fluoroscopy, CT, ultrasound, MRI) to perform minimally invasive procedures.
Vascular IR
- Angiography: Diagnostic and therapeutic; coronary, cerebral, peripheral
- Embolisation: Haemostasis (trauma, GI bleeding, haemoptysis, fibroids, arteriovenous malformations)
- Angioplasty and stenting: Renal artery stenosis, peripheral arterial disease, carotid stenosis
- Thrombolysis/thrombectomy: PE (catheter-directed), DVT, ischaemic stroke
- TIPS (Transjugular Intrahepatic Portosystemic Shunt): Portal hypertension management
- TACE/TARE: Transarterial chemoembolisation/radioembolisation for hepatocellular carcinoma
Non-Vascular IR
- Biopsy guidance: CT-/US-guided lung, liver, renal, lymph node, bone biopsies
- Drainage: Percutaneous abscess drainage, nephrostomy, biliary drainage, pleural drainage
- Ablation: Radiofrequency, microwave, cryoablation for liver, lung, renal tumours
- Vertebroplasty/Kyphoplasty: Cement injection for osteoporotic vertebral fractures
- Spinal procedures: Nerve blocks, discography, facet joint injections
6. Radiation Safety and Dose
| Procedure | Typical Effective Dose |
|---|---|
| CXR (PA) | 0.02 mSv |
| CT Chest (diagnostic) | ~6-7 mSv |
| CT Chest (lung cancer screening) | ~0.9-1.5 mSv (with LDCT protocols) |
| CT Abdomen/Pelvis | ~8-12 mSv |
| PET-CT | ~14-25 mSv |
| V/Q scan | ~1-2 mSv |
| Natural background (annual UK) | ~2.7 mSv |
ALARA Principle (As Low As Reasonably Achievable):
- Justification: Benefit must outweigh risk
- Optimisation: Use minimum dose for diagnostic quality
- Dose limitation: Legislative dose limits for workers and public
Iterative reconstruction in CT allows ~40-60% dose reduction while maintaining diagnostic image quality (particularly valuable in lung cancer screening and paediatric CT).
7. Subspecialties of Radiology
| Subspecialty | Focus |
|---|---|
| Cardiothoracic Radiology | Heart, lungs, mediastinum, great vessels |
| Neuroradiology | Brain, spine, head and neck |
| Musculoskeletal Radiology | Bones, joints, soft tissues |
| Gastrointestinal/Abdominal Radiology | GI tract, liver, pancreas, spleen |
| Genitourinary Radiology | Kidneys, adrenals, bladder, reproductive organs |
| Breast Imaging | Mammography, breast MRI, US |
| Paediatric Radiology | Congenital anomalies, paediatric pathology |
| Interventional Radiology | Minimally invasive image-guided procedures |
| Nuclear Medicine | Functional/metabolic imaging, radiotherapy |
| Emergency Radiology | Trauma, acute presentations |
8. Emerging Technologies
| Technology | Description | Status |
|---|---|---|
| AI / Deep Learning | Computer-aided diagnosis (CAD) for nodule detection, fracture identification, ECG interpretation | Increasingly validated; regulatory approved in several domains |
| Photon-Counting CT | Next-generation detectors converting X-rays directly to electrical pulses; superior contrast, lower dose, spectral imaging | Clinically deployed (first systems ~2021-2024) |
| Hyperpolarised Gas MRI | ³He/¹²⁹Xe ventilation mapping | Research-to-clinical translation ongoing |
| Radiomics | High-dimensional feature extraction from images for predictive modelling | Active research |
| Digital Breast Tomosynthesis | 3D mammography; reduces recall rate, improves cancer detection | Now standard in many centres |
Source: Grainger & Allison's Diagnostic Radiology - A Textbook of Medical Imaging, Chapters 1-3 and selected sections.
This is a shared conversation. Sign in to Orris to start your own chat.