Nor epinephrine vs epinephrine
Reading File
Finding Sources
Finding Sources
Searching the Web
norepinephrine vs epinephrine pharmacology receptor effects clinical use comparison
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information. Here is the full comparison:
Norepinephrine vs. Epinephrine
Both are endogenous catecholamines synthesized from tyrosine, and both act as neurotransmitters and hormones. Epinephrine (adrenaline) is released mainly from the adrenal medulla; norepinephrine is the primary neurotransmitter of postganglionic sympathetic neurons and is also released from the adrenal medulla in smaller amounts.
1. Structure
They differ by a single methyl group on the amine nitrogen — epinephrine has it, norepinephrine does not. This small difference produces dramatically different receptor profiles.
2. Receptor Activity
| Receptor | Norepinephrine | Epinephrine |
|---|---|---|
| α₁ (vasoconstriction) | +++ (dominant) | ++ |
| α₂ (presynaptic inhibition) | ++ | ++ |
| β₁ (heart: ↑HR, ↑contractility) | ++ | +++ |
| β₂ (vasodilation, bronchodilation) | + (weak) | +++ (strong) |
| β₃ (lipolysis/thermogenesis) | + | + |
Rank order of affinity:
- α receptors: epinephrine ≥ norepinephrine >> isoproterenol
- β₁ receptors: isoproterenol > epinephrine = norepinephrine
- β₂ receptors: isoproterenol > epinephrine >> norepinephrine
(Schwartz's Principles of Surgery, Lippincott Pharmacology)
3. Cardiovascular Effects (the key difference)
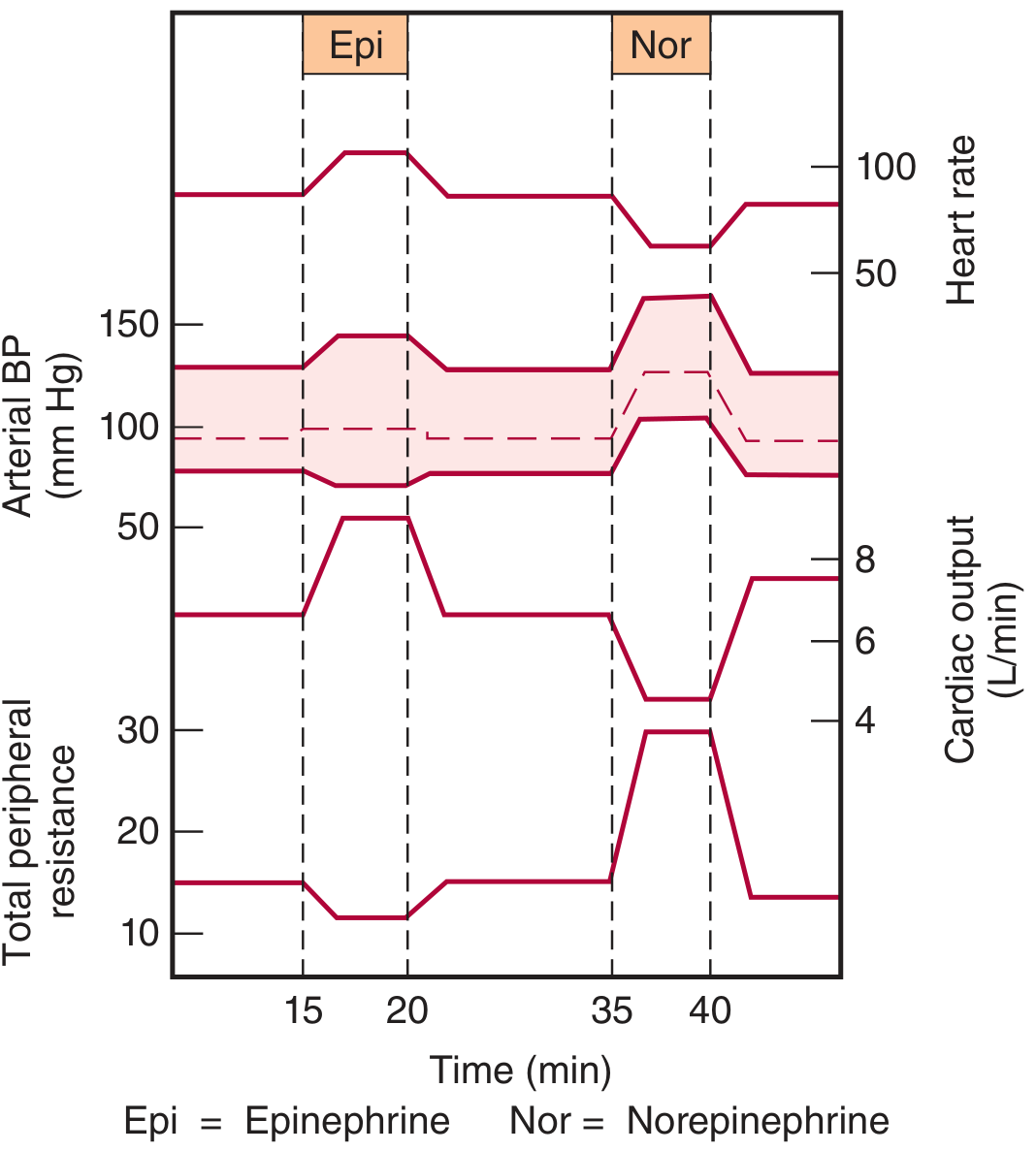
Ganong's Review of Medical Physiology, Fig 19–5: Circulatory changes during slow IV infusion in humans.
| Parameter | Norepinephrine | Epinephrine |
|---|---|---|
| Systolic BP | ↑↑ | ↑ |
| Diastolic BP | ↑↑ | ↓ (β₂ vasodilation) |
| Pulse pressure | Narrow | Widened |
| Total peripheral resistance (TPR) | ↑↑ (α₁ dominant) | ↓ (β₂ vasodilation overrides α in skeletal muscle/liver) |
| Heart rate | ↓ (reflex bradycardia from baroreceptors) | ↑ (direct β₁ + baroreceptor effect insufficient to counteract) |
| Cardiac output | ↓ or unchanged | ↑ |
Key mechanism of heart rate difference:
- Norepinephrine raises BP enough to strongly activate baroreceptors → reflex vagal bradycardia dominates its direct β₁ tachycardia.
- Epinephrine: baroreceptor stimulation is insufficient to obscure the direct β₁ effect → net tachycardia and increased cardiac output.
4. Other Systemic Effects
| Effect | Norepinephrine | Epinephrine |
|---|---|---|
| Bronchial smooth muscle | Minimal (weak β₂) | Bronchodilation (strong β₂) |
| Blood glucose | Glycogenolysis (moderate) | Marked hyperglycemia (β₂ glycogenolysis in liver + ↑glucagon + ↓insulin via α₂) |
| Metabolic rate | ↑ | ↑↑ |
| CNS | Alertness | Alertness + more anxiety/fear |
| Mast cell mediator release | — | Inhibits histamine release |
5. Clinical Uses
| Indication | Drug of Choice | Rationale |
|---|---|---|
| Septic shock (first-line vasopressor) | Norepinephrine | Potent α₁ → ↑SVR → ↑MAP; also has β₁ inotropic support |
| Anaphylaxis | Epinephrine | α₁ (vasoconstriction), β₁ (↑HR/contractility), β₂ (bronchodilation + mast cell inhibition) — reverses all anaphylaxis mechanisms |
| Cardiac arrest (ACLS) | Epinephrine | Restores cardiac rhythm; β₁ + α₁ effects |
| Bronchospasm/asthma emergency | Epinephrine (or selective β₂ agents) | Strong β₂ bronchodilation |
| Adjunct to local anesthesia | Epinephrine | Vasoconstriction prolongs block, reduces systemic absorption |
| Post-cardiac arrest shock | Norepinephrine preferred | Lower re-arrest risk vs. epinephrine (recent meta-analysis) |
Harrison's (2025): "Norepinephrine is the first-choice vasopressor in septic shock... At higher doses, epinephrine has a similar profile... Vasopressin should be added as a second agent, and epinephrine as a third agent."
6. Pharmacokinetics
Both are rapidly metabolized by MAO and COMT → metabolites (metanephrine, normetanephrine, VMA) excreted in urine. Both have a very short duration of action and are given as IV infusions in acute settings.
7. Adverse Effects
| Effect | Norepinephrine | Epinephrine |
|---|---|---|
| Arrhythmias/angina | Yes | Yes (more pronounced) |
| Hypertension | Yes (dominant) | Yes |
| Tissue necrosis on extravasation | Yes — significant risk (treat with phentolamine or topical nitroglycerin) | Less prominent |
| Anxiety/tremor | Less | More |
| Hyperglycemia | Moderate | More marked |
| Pulmonary edema | Less | Yes (↑afterload) |
Quick Memory Hook
Norepinephrine = mostly α → Narrows vessels, No β₂ bronchodilation, Net bradycardia (reflex). Epinephrine = α + strong β → Elevates heart rate and output, Expands bronchi, Essential for anaphylaxis.
Sources: Lippincott Illustrated Reviews: Pharmacology; Ganong's Review of Medical Physiology; Basic Medical Biochemistry (Lieberman); Harrison's Principles of Internal Medicine 22e; Rosen's Emergency Medicine; Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.