Infective endocarditis defination causative agent pathogenesis laboratory diagnosis and treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Now I have comprehensive information. Let me compile the full answer from all sources.
Infective Endocarditis (IE)
1. Definition
Infective endocarditis (IE) is a microbial infection of the heart valves or endocardium that leads to the formation of vegetations composed of thrombotic debris and microorganisms, often associated with destruction of the underlying cardiac tissue. The aorta, aneurysmal sacs, other blood vessels, and prosthetic devices may also become infected. - Robbins & Kumar Basic Pathology, p. 367
More broadly, it is infection of the endovascular surfaces of the heart - most commonly the valves, but also the chamber wall at sites where septal defects create turbulent flow. Infections of cardiac shunts or those related to coarctation of the aorta are considered in the same group due to similar clinical manifestations, microbiology, and management. - Tietz Textbook of Laboratory Medicine, p. 3153
Classification
| Type | Course | Key Feature |
|---|---|---|
| Acute IE | Days to weeks; rapidly destructive | High virulence organisms (e.g., S. aureus); can attack normal valves; high morbidity and mortality |
| Subacute IE | Weeks to months; indolent onset | Lower virulence organisms (e.g., viridans streptococci); almost always on pre-existing abnormal valves; most patients recover with antibiotics |
2. Causative Agents
The vast majority of IE cases are caused by bacteria; fungi, rickettsiae, and Chlamydia are rare causes.
Gram-Positive Organisms (majority)
| Organism | Setting | Type |
|---|---|---|
| S. aureus | Health care-associated, IV drug users, community | Acute; #1 cause worldwide (~31%); attacks normal or damaged valves |
| Viridans group streptococci (S. viridans) | Community-acquired; oral flora | Subacute; ~17%; damaged/deformed valves; dominant in developing countries |
| Streptococcus bovis | Colorectal disease | Subacute; ~6% |
| Enterococci (E. faecalis, E. faecium) | Genitourinary procedures, health care | Subacute; ~10%; elderly patients; VRE strains difficult to treat |
| Coagulase-negative staphylococci | Prosthetic valves, catheters | ~11% of cases |
- Tietz Textbook of Laboratory Medicine, p. 3154
Gram-Negative Organisms (~4%)
HACEK group - fastidious oral flora; cause subacute, community-acquired IE; form large vegetations:
- Haemophilus spp.
- Aggribatibacter actinomycetemcomitans / aphrophilus (formerly Actinobacillus)
- Cardiobacterium hominis
- Eikenella corrodens
- Kingella kingae
Other gram-negatives (E. coli, Klebsiella, Pseudomonas) - rare, acute, high mortality. - Braunwald's Heart Disease, p. 825
Fungi (rare)
Primarily Candida species; also Aspergillus. Health care-associated (CVC, prosthetic valves, IV drug use). Surgical intervention almost always required.
Culture-Negative IE (~10%)
Due to prior antibiotic therapy or fastidious/difficult-to-culture organisms (e.g., Coxiella burnetii [Q fever], Bartonella spp., Tropheryma whipplei). - Robbins & Kumar, p. 368
3. Pathogenesis
IE develops through a sequential chain of events:
Step 1 - Endothelial Damage
Turbulent blood flow (from valvular disease, septal defects, jet lesions) damages the valve endothelium, exposing the subendothelial matrix.
Step 2 - Non-Bacterial Thrombotic Endocarditis (NBTE)
At sites of endothelial disruption, sterile platelet-fibrin deposits form. These serve as a nidus for bacterial colonization. Predisposing sites include pacemaker leads, indwelling catheters, and endocardium damaged by flow jets.
Step 3 - Bacteremia
Microbes enter the bloodstream via:
- Dental or surgical procedures
- IV drug injection
- Infections elsewhere (skin, gut, urinary tract)
- Trivial injuries or occult sources
Step 4 - Microbial Adherence and Colonization
Organisms in the bloodstream adhere to NBTE lesions. The ability to adhere depends on specific microbial virulence factors (surface proteins of staphylococci and streptococci that bind fibronectin, fibrinogen, etc.), explaining why gram-positive cocci cause IE far more often than gram-negative bacilli.
Step 5 - Vegetation Formation
Once colonized, organisms become embedded in an enlarging mass of platelets, fibrin, inflammatory cells, and proliferating microbes - the vegetation. These are:
- Friable and bulky
- Contain large numbers of organisms
- Poorly penetrated by host defenses and antibiotics (avascular)
Step 6 - Local and Systemic Complications
- Local: valve destruction, ring abscess (extension into myocardium), conduction abnormalities, perforation
- Embolic: septic emboli lodge in brain, kidneys, spleen, lungs; cause infarcts, abscesses, mycotic aneurysms
- Immunologic: circulating immune complexes cause glomerulonephritis, Osler nodes, Roth spots
Predisposing Conditions
-
Mitral valve prolapse (most common preexistent risk factor today)
-
Rheumatic heart disease, bicuspid aortic valve, calcific stenosis
-
Prosthetic heart valves (10-20% of all IE cases)
-
IV drug use
-
Neutropenia, immunodeficiency, diabetes, malignancy, alcohol use
-
Robbins & Kumar, p. 367-368
4. Vegetation Morphology
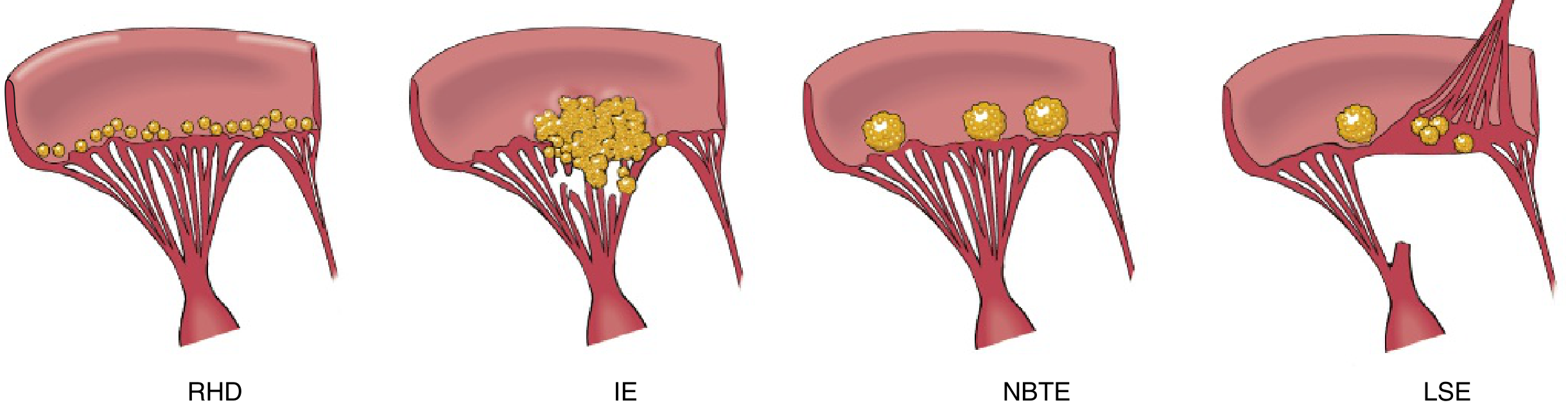
From Robbins & Kumar - comparison of vegetation types: RHD (small beads along the valve line of closure), IE (large irregular destructive masses), NBTE (small sterile thrombi), LSE (Libman-Sacks).
- IE vegetations affect aortic and mitral valves most commonly (tricuspid in IV drug users)
- Can be single or multiple, may erode into underlying myocardium causing ring abscess
- Shedding of emboli is common given their friable nature
5. Clinical Features
- Fever - most consistent sign (may be absent in subacute disease in elderly)
- Murmur - present in ~90% of left-sided lesions; new or changing murmur is significant
- Peripheral stigmata (from emboli or immune reactions):
- Splinter hemorrhages (nail bed)
- Janeway lesions - painless erythematous macules of palms/soles (septic emboli)
- Osler nodes - painful tender subcutaneous nodules on fingers/toes (immune complex)
- Roth spots - retinal hemorrhages (immune complex)
- Petechiae
- Splenomegaly (especially subacute)
- Embolic events: stroke, renal/splenic infarcts, septic pulmonary emboli (right-sided IE)
- Glomerulonephritis, hematuria, renal failure
6. Laboratory Diagnosis
A. Blood Cultures (most important)
- 3 sets of blood cultures from separate venipuncture sites, ideally drawn 30-60 minutes apart before starting antibiotics
- 90% of culture-positive cases are identified with the first 3 sets
- Modern automated blood culture systems reliably detect HACEK organisms within 2-3 days (historically took longer)
- Blood cultures should be incubated for ≥5 days
- Repeat cultures 48-72 h after starting therapy to document clearance
B. Duke Criteria (Modified - now Duke-ISCVID Criteria)
Used to classify patients as Definite, Possible, or Rejected IE.
Major Criteria
- Blood culture positive for IE:
- Typical microorganism from 2 separate blood cultures (S. viridans, S. gallolyticus, HACEK group, S. aureus, community-acquired enterococci with no primary focus)
- Persistently positive blood cultures (≥2 cultures drawn >12 h apart, or all 3 of 3, or majority of ≥4)
- Single positive culture for Coxiella burnetii or Phase 1 IgG antibody >1:800
- Evidence of endocardial involvement on echocardiography (vegetation, abscess, new valvular regurgitation, or prosthetic valve dehiscence)
- Imaging criteria: abnormal FDG-PET/CT within 3 months of prosthetic valve implantation
- New valvular regurgitation on auscultation
Minor Criteria
- Predisposing heart condition or IV drug use
- Fever ≥38°C
- Vascular phenomena (emboli, mycotic aneurysm, Janeway lesions, conjunctival hemorrhage)
- Immunologic phenomena (glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor)
- Positive blood culture not meeting major criterion
Classification
-
Definite IE: 2 major, OR 1 major + 3 minor, OR 5 minor (clinical); OR pathologic criteria from surgical/autopsy specimen
-
Possible IE: 1 major + 1 minor, OR 3 minor
-
Rejected: Firm alternative diagnosis, or resolution with <4 days of antibiotics
-
Harrison's Principles of Internal Medicine 22E, p. (Duke-ISCVID section)
C. Echocardiography
- Transthoracic echocardiography (TTE): Highly specific but misses 20-35% of vegetations, especially those <2 mm. Images are inadequate in ~20% of patients.
- Transesophageal echocardiography (TEE): Preferred when TTE is negative/equivocal with high suspicion, in prosthetic valve IE, staphylococcal bacteremia, or complications (abscess, fistula) suspected. More sensitive (TEE detects ~90% of vegetations).
- All patients with suspected IE should have echocardiography. - Braunwald's Heart Disease; Harrison's
D. Non-Culture Laboratory Tests
| Test | Use |
|---|---|
| CBC | Anemia, leukocytosis |
| ESR, CRP | Elevated (markers of inflammation) |
| Rheumatoid factor | Positive in ~50% subacute IE (minor Duke criterion) |
| Urinalysis | Microscopic hematuria, proteinuria (glomerulonephritis) |
| Serology | Coxiella (Q-fever), Bartonella IgG/IgM (IgG ≥1:800 is major criterion) |
| PCR / 16S rRNA | On blood or surgical vegetation; useful in culture-negative IE; detects C. burnetii, Bartonella, T. whipplei |
| Metagenomic sequencing (NGS) | Next-generation sequencing of serum; emerging tool for culture-negative IE; currently minor criterion only (unless identifies the 3 listed organisms) |
| Histopathology | Vegetation from surgery/embolectomy - identifies organisms with special stains |
| FDG-PET/CT | Detects prosthetic valve infection and extracardiac embolic foci |
- Harrison's Principles of Internal Medicine 22E; Tietz Textbook of Laboratory Medicine
7. Treatment
IE management requires a multidisciplinary team approach including infectious disease specialists, cardiologists, and cardiothoracic surgeons. All patients should be managed in an inpatient setting. - Braunwald's Heart Disease
A. Antibiotic Therapy (general principles)
- Use bactericidal agents (not bacteriostatic)
- Prolonged courses are required because organisms within vegetations are metabolically inactive and protected from host defenses - typically 4-6 weeks of IV antibiotics
- Parenteral therapy is standard; oral step-down is considered in selected uncomplicated cases (supported by the POET trial)
- Start empirically only after ≥3 blood culture sets are drawn; delay in hemodynamically stable patients to allow cultures to guide therapy
B. Pathogen-Specific Regimens (Harrison's 22E)
| Organism | First-line | Alternative |
|---|---|---|
| Viridans streptococci / S. bovis (penicillin-susceptible, MIC ≤0.12 μg/mL) | Penicillin G or ceftriaxone × 4 wks; or + gentamicin × 2 wks | Vancomycin × 4 wks (penicillin allergy) |
| Viridans streptococci (relatively resistant, MIC 0.12-0.5 μg/mL) | Penicillin G + gentamicin × 4 wks | Vancomycin × 4 wks |
| MSSA (methicillin-susceptible S. aureus) | Nafcillin/oxacillin × 6 wks (± gentamicin × 3-5 days for native valve) | Cefazolin × 6 wks; vancomycin if penicillin allergy |
| MRSA | Vancomycin × 6 wks | Daptomycin (high dose) |
| Enterococci (susceptible) | Ampicillin + ceftriaxone × 6 wks, or ampicillin/penicillin + gentamicin × 4-6 wks | Vancomycin + gentamicin (penicillin allergy) |
| HACEK organisms | Ceftriaxone × 4 wks | Ampicillin-sulbactam or ciprofloxacin |
| Candida | Liposomal amphotericin B ± flucytosine; step-down to fluconazole | Echinocandin (initial); surgical valve replacement almost always required |
C. Empirical Therapy (before cultures available)
- Native valve, community-acquired: Cover streptococci + staphylococci - ampicillin + cloxacillin + gentamicin OR vancomycin + gentamicin
- Health care-associated or prosthetic valve: Vancomycin + gentamicin ± rifampicin (prosthetic) to cover MRSA and coagulase-negative staphylococci
D. Surgical Indications
Surgery is recommended for:
- Heart failure from valve dysfunction (most common indication - urgent/emergency)
- Uncontrolled infection: abscess, fistula, enlarging vegetation despite therapy, persistent bacteremia >5-7 days
- Prevention of embolism: large mobile vegetations (>10 mm), especially with prior embolic event
- Fungal IE (almost all cases require surgery)
- Prosthetic valve endocarditis with dehiscence or new regurgitation
E. Antibiotic Prophylaxis (Updated 2021 AHA Guidelines)
Prophylaxis is recommended only for high-risk cardiac conditions before invasive dental procedures:
- Prosthetic cardiac valve or material
- Previous IE
- Certain congenital heart diseases (unrepaired cyanotic CHD, repaired with prosthetic material within 6 months, repaired with residual defects)
- Cardiac transplant with valve abnormalities
- Ventricular assist devices and implantable hearts (added in 2021)
Preferred regimen: Amoxicillin 2 g orally 30-60 min before procedure
True penicillin allergy: Doxycycline (added 2021) or azithromycin/clarithromycin (clindamycin removed in 2021 due to C. difficile risk)
- Braunwald's Heart Disease, p. 824; Harrison's Principles of Internal Medicine 22E
Summary Table
| Feature | Acute IE | Subacute IE |
|---|---|---|
| Main organism | S. aureus | Viridans streptococci |
| Valve | Normal or damaged | Damaged (MVP, RHD) |
| Course | Days-weeks | Weeks-months |
| Vegetations | Destructive, large | Less destructive |
| Peripheral signs | May be absent | Osler nodes, Roth spots prominent |
| Prognosis | Worse | Better |
Sources: Robbins & Kumar Basic Pathology; Braunwald's Heart Disease (11e); Tietz Textbook of Laboratory Medicine (7e); Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.