Mysthenia gravis and Lambert eaton difference
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from authoritative sources. Here is the full, detailed comparison:
Myasthenia Gravis vs. Lambert-Eaton Myasthenic Syndrome (LEMS)
Both are autoimmune disorders of the neuromuscular junction (NMJ), but they differ fundamentally in where the attack occurs (post-synaptic vs. pre-synaptic), the antibodies involved, clinical pattern, and electrodiagnostic findings.
1. Site of Lesion
| Feature | Myasthenia Gravis (MG) | Lambert-Eaton (LEMS) |
|---|---|---|
| Site | Post-synaptic NMJ | Pre-synaptic NMJ |
| Target | Acetylcholine receptors (AChR) on muscle end-plate | Voltage-gated calcium channels (VGCC) on nerve terminal |
| Mechanism | Antibodies block/destroy AChRs; complement activation; destruction of post-junctional folds | Antibodies against P/Q-type VGCCs reduce Ca²⁺ entry → reduced ACh release |
In MG, the amplitude of miniature end-plate potentials (MEPPs) is reduced despite normal quantal frequency, confirming the post-synaptic defect. In LEMS, the problem is upstream - insufficient Ca²⁺ influx means fewer vesicles are released in the first place.
(Medical Physiology, Bradley and Daroff's Neurology in Clinical Practice)
2. Autoantibodies
| Feature | MG | LEMS |
|---|---|---|
| Primary antibody | Anti-AChR (85% of cases); targets α-subunit MIR region | Anti-P/Q-type VGCC (>90% of CA-LEMS; >90% NCA-LEMS) |
| Other antibodies | Anti-MuSK (~5-8%), anti-LRP4, anti-agrin | Anti-SOX1 (64% of LEMS with SCLC; useful tumor marker) |
| Antibody titer correlation | Correlates loosely with disease severity | Does NOT correlate with disease severity |
(Bradley and Daroff's Neurology, Bradley 108)
3. Clinical Features - Key Differences
| Feature | MG | LEMS |
|---|---|---|
| Classic muscles affected | Ocular and bulbar first - ptosis, diplopia, dysarthria, dysphagia | Proximal limb muscles first - legs more than arms |
| Ptosis/diplopia | Very prominent, often presenting symptom (~2/3 of cases) | Present in minority; less prominent |
| Bulbar involvement | Common - chewing, swallowing, speech difficulty | Generally not prominent (though can occur) |
| Respiratory weakness | Can occur (myasthenic crisis) | Uncommon unless severe or surgery with NMJ blockers |
| Autonomic features | Rare | Common - dry mouth, erectile dysfunction, postural hypotension, constipation, blurry vision (~80%) |
| Tendon reflexes | Normal | Absent or diminished (almost always) |
| Fatigability pattern | Weakness WORSENS with repeated effort | Strength may briefly IMPROVE after brief exercise, then weaken with sustained activity |
| Age/sex | Bimodal: young women (20s) and older men (60s); women 3x more in <40 yrs | Usually onset >40 yrs; males and females equally affected |
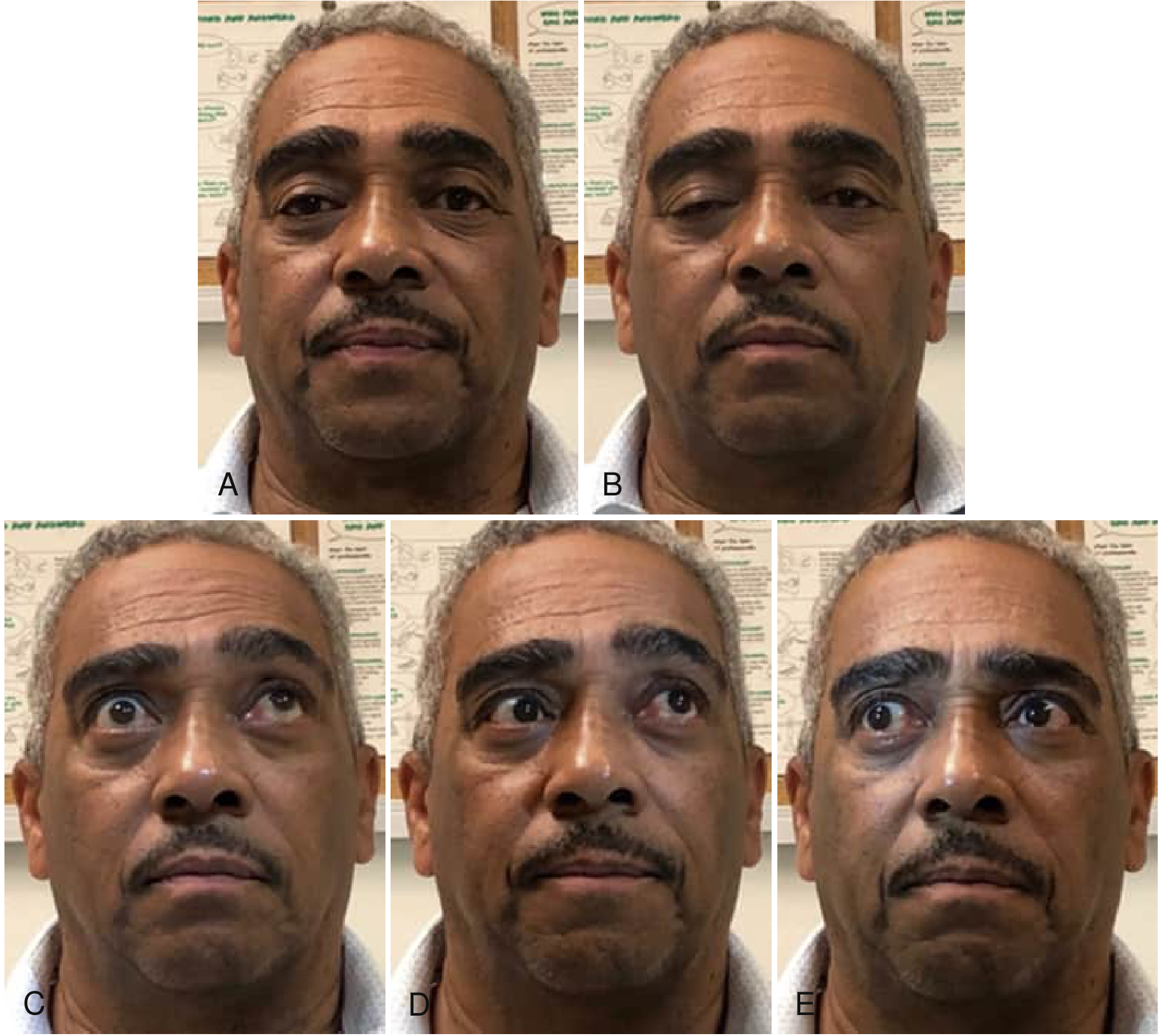
The image below shows ocular motility abnormalities classic for MG - note the restricted eye movements in multiple gaze directions, a hallmark not typically seen in LEMS:
4. Association with Cancer / Underlying Cause
| Feature | MG | LEMS |
|---|---|---|
| Paraneoplastic | ~10-15% have thymoma; occasionally other cancers | ~60% have underlying malignancy |
| Cancer type | Thymoma | Small-cell lung cancer (SCLC) in ~80% of cancer cases |
| Thymus association | Thymic hyperplasia (young women) or thymoma (older men) | SCLC cells are neuroectodermal origin, express VGCCs, triggering autoimmunity |
| Non-paraneoplastic | Most cases are primary autoimmune | ~40% NCA-LEMS; associated with other autoimmune diseases (thyroiditis, T1DM) |
| Tumor survival | - | MG in SCLC patients is associated with improved tumor survival |
In LEMS, 91% of SCLCs are detected within 3 months of LEMS onset and 96% within 1 year - so aggressive tumor screening is mandatory immediately after LEMS diagnosis. (Bradley and Daroff's Neurology)
5. Electrodiagnostic Findings (KEY EXAM POINT)
This is the most testable differentiating feature:
| Feature | MG | LEMS |
|---|---|---|
| Baseline CMAP amplitude | Normal or mildly reduced | Low amplitude (small CMAPs) |
| Slow repetitive nerve stimulation (2-5 Hz) | Decremental response (>10% decrement) | Also decremental |
| Rapid repetitive nerve stimulation (20-50 Hz) or post-exercise | No significant increment | Incremental response (≥100% increase in CMAP) - pathognomonic |
| Post-exercise brief facilitation | No | Yes - CMAPs transiently increase |
| EMG single fiber | Increased jitter | Increased jitter |
The key mnemonic: MG = decrement only; LEMS = decrement at slow + INCREMENT at fast stimulation.
The mechanism: in LEMS, rapid stimulation accumulates Ca²⁺ at the nerve terminal progressively, which compensates for the VGCC blockade and releases more ACh - hence facilitation. In MG, rapid stimulation exhausts depleted post-synaptic AChRs further - hence decrement. (Medical Physiology; Bradley and Daroff's Neurology)
6. Response to Edrophonium (Tensilon Test)
| Feature | MG | LEMS |
|---|---|---|
| Response | Positive (dramatic improvement) | Not robust or consistent - less reliable |
7. Treatment
| Feature | MG | LEMS |
|---|---|---|
| Symptomatic | Acetylcholinesterase inhibitors (pyridostigmine) | Amifampridine (3,4-DAP) - increases Ca²⁺ entry by blocking K⁺ channels, prolonging AP duration |
| Immunotherapy | Corticosteroids, azathioprine, mycophenolate, IVIG, plasmapheresis | Corticosteroids, IVIG, plasmapheresis, rituximab |
| Surgical | Thymectomy (if thymoma or generalized MG) | Treat underlying SCLC first - weakness may improve with cancer treatment |
| Targeted biologics | Eculizumab (anti-C5), efgartigimod (FcRn inhibitor), rozanolixizumab | - |
8. Summary Comparison Table
| Feature | MG | LEMS |
|---|---|---|
| Site | Post-synaptic | Pre-synaptic |
| Antibody | Anti-AChR (or anti-MuSK) | Anti-VGCC (P/Q type) |
| Muscles | Ocular > bulbar > limb | Proximal limb (legs > arms) |
| Ptosis | Prominent | Mild/absent |
| Autonomic | Absent | Present (dry mouth, etc.) |
| Reflexes | Normal | Absent/diminished |
| Brief exercise effect | Worsens weakness | Transiently improves |
| EMG (fast RNS) | Decrement | Increment (≥100%) |
| Cancer link | Thymoma (10-15%) | SCLC (60%) |
| Tensilon test | Positive | Unreliable |
| Treatment | Pyridostigmine + immunosuppression | Amifampridine + treat cancer |
Sources: Bradley and Daroff's Neurology in Clinical Practice (9e), Chapter 108; Medical Physiology (Boron & Boulpaep); Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.