One lung ventilation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"one-lung ventilation" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have comprehensive, detailed information. Here is a thorough review of one-lung ventilation (OLV).
One-Lung Ventilation (OLV)
Definition and Purpose
One-lung ventilation is a technique in which only one lung is ventilated during thoracic surgery while the other lung is deliberately collapsed and rendered non-ventilated. It is used both for lung separation (improving surgical access) and lung isolation (protecting one lung from contamination by the other). The distinction between these two goals is critical for choosing the correct airway device.
Indications
Absolute Indications (Lung Isolation - life-threatening if not done)
- Isolation of each lung to prevent contamination: massive hemoptysis, empyema, lung abscess, or bronchopleural fistula
- Unilateral pulmonary lavage (e.g., pulmonary alveolar proteinosis)
- Large bronchopleural fistula - where PPV directed to the diseased side results in inadequate ventilation of the normal lung
- Severe bullous/cystic disease - risk of tension pneumothorax
Relative Indications (Lung Separation - for surgical access)
-
Lobectomy, pneumonectomy, segmental resection
-
Esophageal surgery
-
Thoracic aortic surgery
-
Video-assisted thoracoscopic surgery (VATS)
-
Minimally invasive cardiac surgery
-
Transthoracic spine surgery
-
Barash, Clinical Anesthesia, 9e, p. 3173
-
Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1024
Physiology of OLV
The Core Problem: Obligatory Shunt
During OLV, the non-ventilated (nondependent) lung continues to receive blood flow but no ventilation, creating an obligatory right-to-left intrapulmonary shunt. This is in contrast to normal two-lung ventilation where the shunt fraction is only ~10%.
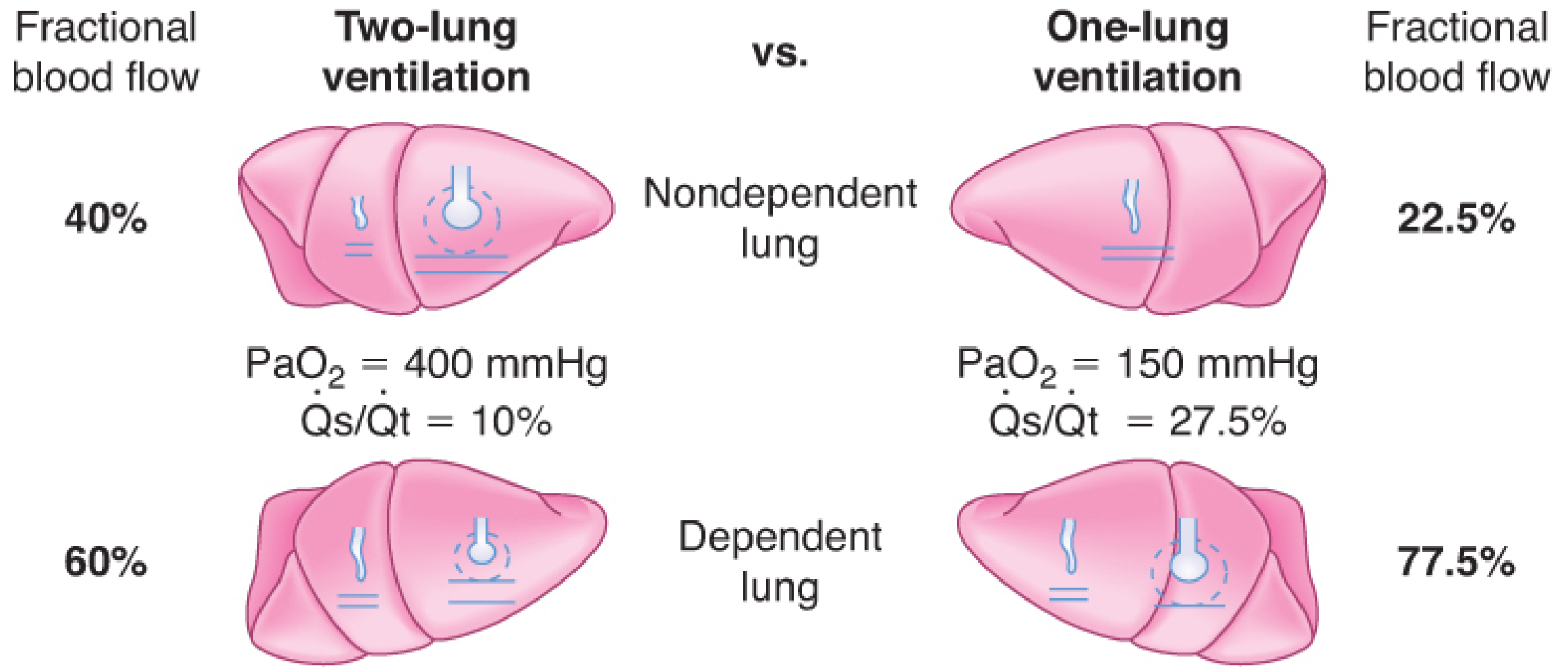
Typical values during two-lung vs. one-lung ventilation (Barash, 9e). Note the shunt fraction (Qs/Qt) increases from 10% to 27.5%, and PaO2 drops from ~400 to ~150 mmHg.
Two Main Causes of Impaired Oxygenation During OLV
- Persisting blood flow through the non-ventilated lung - creating a direct shunt
- Atelectasis in the dependent (ventilated) lung - causing local shunt and low V/Q areas due to lateral position, paralysis, and mediastinal weight
Hypoxic Pulmonary Vasoconstriction (HPV) - The Body's Defense
HPV is the primary autoregulatory mechanism that diverts blood away from the non-ventilated lung. The non-ventilated nondependent lung receives ~40% of total pulmonary blood flow during two-lung ventilation; HPV reduces this to ~22.5% during OLV - a roughly 50% reduction. The anesthesiologist's goal is to maximize PVR in the non-ventilated lung while minimizing PVR in the ventilated lung.
Key principle: PVR is lowest at FRC and increases both above and below FRC. The aim is to keep the ventilated lung near its FRC while facilitating complete collapse of the non-ventilated lung.
Factors that INHIBIT HPV (worsen shunting):
- Pulmonary hypertension
- Hypocapnia / respiratory alkalosis
- Increased cardiac output; increased mixed venous PO2
- Hypothermia
- Vasodilators: nitroglycerin, nitroprusside, nitric oxide
- Phosphodiesterase inhibitors (milrinone, enoximone, inamrinone)
- Beta-adrenergic agonists
- Calcium channel blockers
- Volatile (inhalation) anesthetics
Factors that DECREASE blood flow to the VENTILATED lung (indirectly worsen shunting):
-
High mean airway pressures (from high PEEP, hyperventilation, or high peak inspiratory pressures)
-
Low FiO2 in the ventilated lung (causes HPV in the ventilated lung)
-
Vasoconstrictors with greater effect on normoxic than hypoxic vessels
-
Intrinsic PEEP from inadequate expiratory times
-
Morgan & Mikhail's, 7e, p. 1024-1025
-
Miller's Anesthesia, 10e, p. 1321-1322
Techniques for OLV (Lung Separation Devices)
Four techniques are available:
1. Double-Lumen Tube (DLT) - Most Commonly Used
- Has two lumens: one for the trachea, one for a mainstem bronchus
- Left-sided DLT preferred in most cases (safer margin to left upper lobe)
- Right-sided DLT needed for: left pneumonectomy, left mainstem bronchial stenosis, left bronchial trauma
- Confirmation of position is mandatory via fiberoptic bronchoscopy - position can shift with patient movement and surgical traction
- Risk: postoperative hoarseness (44% vs. 17% with bronchial blockers), vocal cord lesions, tracheal/bronchial laceration (rare but serious)
- Advantages: Faster placement, more reliable isolation, allows suction of both lungs, best for lung isolation cases
2. Bronchial Blocker (BB)
- A balloon-tipped catheter passed alongside or through a standard single-lumen tube, directed to the target bronchus under bronchoscopic guidance
- Types: Arndt blocker, Cohen Flex-tip blocker, Fuji Uniblocker, EZ Blocker
- Univent tube: single-lumen tube with an integrated movable endobronchial blocker
- Advantages: Useful in difficult airway, tracheostomy patients, morbidly obese, pediatric patients; avoids tube exchange at end of procedure; lower hoarseness/vocal cord injury rate
- Disadvantages: Slower to place; higher risk of displacement intraoperatively; does not provide a protective seal adequate for lung isolation (blood/pus can bypass the high-pressure balloon); limits suctioning; once deflated, the healthy lung may be contaminated
3. Endobronchial Intubation with Single-Lumen Tube
- Conventional ETT advanced into a mainstem bronchus
- Reserved as a last resort - limited control, no easy switching between lungs
4. Tubeless Techniques
- Used for select VATS procedures
- Avoids intubation entirely; relies on spontaneous ventilation with regional anesthesia
DLT vs. BB: A 2025 meta-analysis (PMID 40450255) confirmed bronchial blockers have lower airway injury rates while DLTs provide faster, more reliable placement.
- Barash, 9e, p. 3173-3194
- Morgan & Mikhail's, 7e, p. 1025
Management of OLV: Ventilation Strategy
Tidal Volume
- Old practice: 10 mL/kg (same as two-lung ventilation) - raised PaO2 by recruiting atelectatic regions but caused ventilator-induced lung injury
- Current recommendation: 4-6 mL/kg ideal body weight - lung-protective strategy
- Tidal volumes < 3 mL/kg per lung may paradoxically cause derecruitment, atelectasis, and hypoxemia
FiO2
- Start with FiO2 1.0 in patients at risk; a lower FiO2 of 50-80% is preferred when possible
- High FiO2 carries risk of oxygen toxicity and absorption atelectasis
Ventilatory Pressures
- Plateau pressure < 25 cm H2O
- Peak airway pressure < 35 cm H2O
- Pressure-controlled ventilation may reduce peak pressures and improve gas distribution
PEEP
- PEEP to the ventilated (dependent) lung maintains it near FRC and prevents atelectasis
- PEEP must be individualized - excessive PEEP raises airway pressures, compresses alveolar vessels, and can redistribute blood flow toward the non-ventilated lung, worsening oxygenation
- Titrate PEEP to optimal compliance
Pre-OLV: Denitrogenation
- Before collapsing the non-ventilated lung, ventilate it with 100% oxygen to wash out nitrogen
- Nitrogen has low blood-gas solubility and delays collapse (especially problematic in emphysema and at start of VATS)
- Nitrous oxide accelerates collapse further but is generally avoided in thoracic cases (risk of bullae)
Recruitment Maneuvers
- Perform a recruitment maneuver to the dependent lung immediately after initiating OLV (hold at 20 cmH2O for 15-20 seconds)
- Counteracts atelectasis that accumulates during the pre-OLV two-lung phase
Permissive Hypercapnia
- Acceptable in patients with elevated CO2 despite adequate SpO2 and reasonable minute ventilation
- Hypercarbia slightly increases HPV but the net benefit is minimal and can raise PAP in the ventilated lung
Reinflation
-
At end of procedure: reinflate operative lung gradually to peak inspiratory pressure < 30 cm H2O to avoid disrupting staple lines
-
Miller's Anesthesia, 10e, p. 7189-7204
-
Morgan & Mikhail's, 7e, p. 1046
Management of Hypoxemia During OLV
Hypoxemia during OLV (SpO2 < 90% / PaO2 < 60 mmHg) requires a stepwise approach:
| Step | Intervention |
|---|---|
| 1 | Confirm correct DLT/BB position with fiberoptic bronchoscopy; suction both lumens |
| 2 | Increase FiO2 to 1.0 |
| 3 | Recruitment maneuver on the dependent (ventilated) lung |
| 4 | Apply PEEP (but not excessive) to the dependent lung |
| 5 | Apply CPAP or blow-by O2 to the non-ventilated (operative) lung - reduces shunt but may impair VATS visualization; use cautiously |
| 6 | Resume two-lung ventilation for severe hypoxemia |
| 7 | Surgeon clamps the pulmonary artery to the non-ventilated lung (ultimate measure during pneumonectomy) |
Pharmacologic options:
- Almitrine (IV pulmonary vasoconstrictor) - potentiates HPV, reduces shunt flow to non-ventilated lung; most effective when combined with inhaled NO
- Inhaled NO - vasodilates ventilated regions, improving V/Q; minimal effect alone but synergistic with almitrine
- Inhaled NO alone has little benefit
Acceptable SpO2 during OLV: Generally ≥ 90% (PaO2 > 60 mmHg). Transiently into high 80s may be acceptable in healthy patients. Target higher in patients with coronary artery disease, cerebrovascular disease, anemia, or limited cardiopulmonary reserve.
Intraoperative position: Lateral decubitus position gives significantly better PaO2 during OLV compared to supine, due to gravity-assisted perfusion matching to the dependent ventilated lung.
- Miller's Anesthesia, 10e, p. 7191
- Morgan & Mikhail's, 7e, p. 1046-1047
Acute Lung Injury (ALI) After OLV
ALI has replaced hypoxemia as the primary concern in modern thoracic anesthesia:
- Overall incidence: 2.5% of all lung resections
- After pneumonectomy: 7.9%
- When ALI occurs: ~40% mortality or major morbidity
Protective ventilation is the key preventive strategy - low tidal volumes, lower FiO2, lower ventilatory pressures. Both the ventilated lung (hyperfusion + barotrauma risk) and the non-ventilated lung (ischemia-reperfusion injury + surgical trauma) are at risk.
A 2025 systematic review (PMID 40637441) evaluated volatile vs. IV anesthetics on inflammatory markers in thoracic surgical patients - an evolving area relevant to ALI prevention.
Monitoring During OLV
- Pulse oximetry - continuous SpO2 monitoring is essential
- Arterial blood gas - periodic ABG for PaO2 and PaCO2
- End-tidal CO2 - useful as a trend but underestimates PaCO2 due to increased dead space; the A-ET CO2 gradient is unpredictable during OLV
Special Situations
| Situation | Consideration |
|---|---|
| Difficult airway | Use bronchial blocker with fiberoptic intubation; avoids need for DLT exchange at end |
| Tracheostomy | DLT cannot be used; bronchial blocker through trach tube is preferred |
| Morbid obesity | Consider bronchial blocker; DLT placement may be difficult |
| Pediatric patients | Standard DLTs not available for small children; use bronchial blocker (Arndt) or endobronchial intubation |
| COPD | Delayed lung collapse; careful denitrogenation mandatory; intrinsic PEEP a concern |
| Pneumonectomy | Surgeon can clamp pulmonary artery if severe hypoxemia persists |
Summary Points
- OLV creates an obligatory shunt (20-30%) from persistent perfusion of the non-ventilated lung
- HPV is the main defense - inhibited by volatiles, vasodilators, and alkalosis
- DLT is the gold standard for most cases; bronchial blocker preferred in difficult airway and tracheostomy
- Fiberoptic confirmation of DLT/BB position is mandatory
- Lung-protective ventilation: 4-6 mL/kg TV, low pressures, individualized PEEP
- Acceptable SpO2 ≥ 90% during OLV; treat stepwise if hypoxemia occurs
- ALI is the primary modern concern: protective ventilation strategy reduces risk
- Miller's Anesthesia, 10e | Morgan & Mikhail's Clinical Anesthesiology, 7e | Barash, Clinical Anesthesia, 9e
This is a shared conversation. Sign in to Orris to start your own chat.