Coronary artery
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have excellent, comprehensive information from multiple authoritative textbooks along with detailed diagrams. Let me compile the full answer.
Coronary Arteries
The coronary arteries are the vessels that supply oxygenated blood to the myocardium. They arise from the aortic sinuses of Valsalva just above the aortic valve and travel along the epicardial surface of the heart before penetrating into the myocardium.
Origin and Overview
Both coronary arteries originate from the ascending aorta:
- The Right Coronary Artery (RCA) arises from the right aortic sinus (right coronary sinus of Valsalva)
- The Left Coronary Artery (LCA/LM) arises from the left aortic sinus (left coronary sinus of Valsalva)
Overall coronary branching patterns are relatively uniform, though individual variation exists.
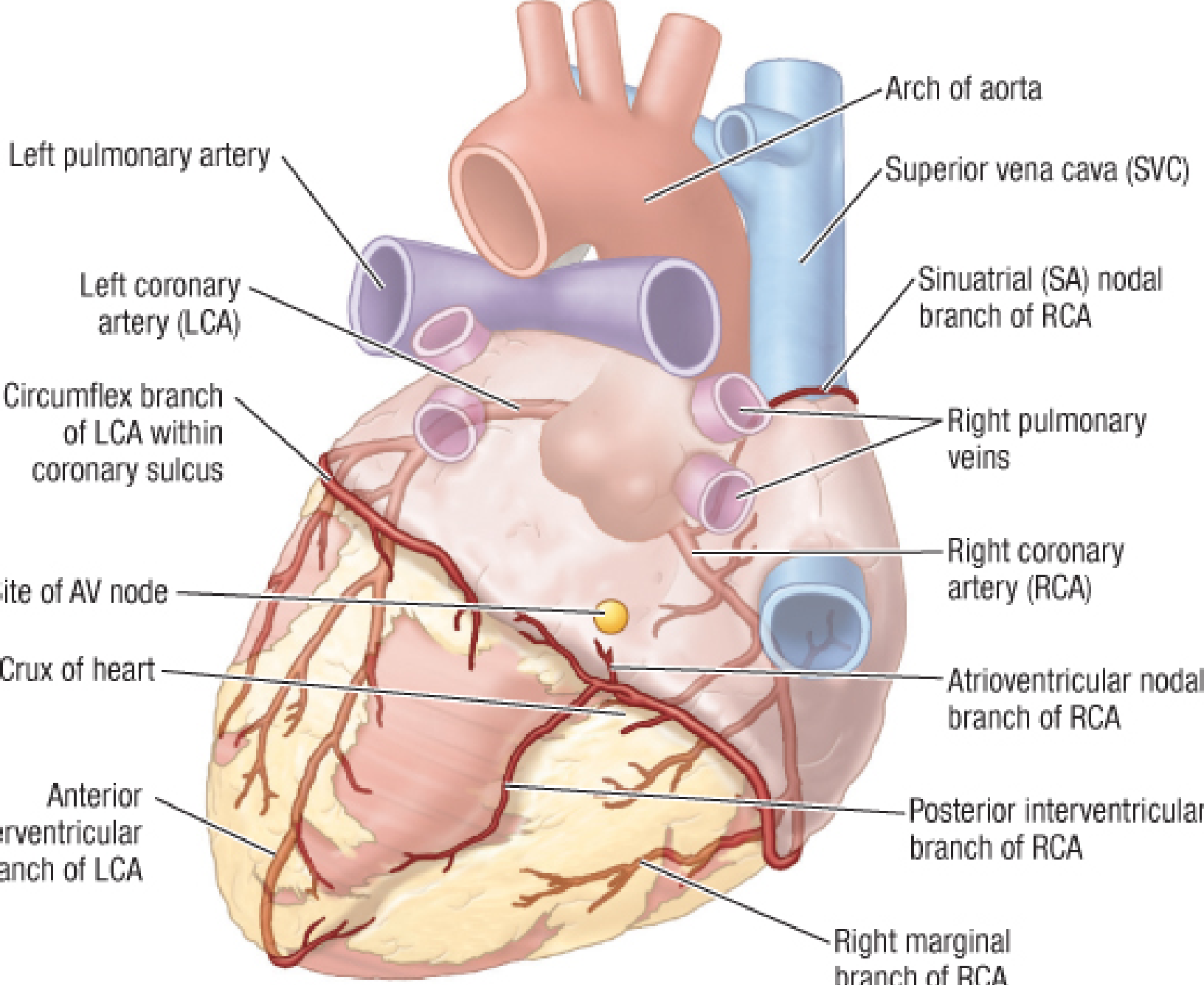
Right Coronary Artery (RCA)
The RCA originates from the right aortic sinus and enters the coronary sulcus (atrioventricular groove). It courses on the anterior surface of the heart supplying the right atrium and right ventricle, then continues posteriorly in the coronary sulcus to anastomose with the left coronary artery.
Main branches of the RCA:
| Branch | Course & Supply |
|---|---|
| Sinoatrial (SA) nodal branch | Ascending branch near the RCA origin; supplies the SA node in ~60% of people (remaining 40% from the circumflex) |
| Right marginal branch | Courses along the right margin of the heart |
| Posterior interventricular branch (PDA) | In right-dominant hearts; runs in the posterior interventricular sulcus, supplies the posterior one-third of the interventricular septum and inferior free wall |
| AV nodal branch | Supplies the AV node (from the RCA in ~55% of patients) |
The RCA and its branches supply most of the RV; the anterior wall of the RV also receives branches from the LAD.
Left Coronary Artery (LCA / Left Main)
The left main coronary artery arises from the left coronary sinus of Valsalva and bifurcates (occasionally trifurcates) into two major vessels:
1. Left Anterior Descending (LAD)
Travels in the anterior interventricular sulcus toward the apex, sometimes wrapping around it:
- Septal perforating branches - supply the anterior two-thirds of the interventricular septum
- Diagonal branches - supply the anterior LV wall
- Supplies the medial half of the LV anterior wall and the apex
2. Circumflex Artery (Cx)
Follows the coronary sulcus around the left border of the heart to the posterior surface:
- Obtuse marginal branches - supply the lateral LV wall (anterior and inferior aspects)
- Left marginal branch - courses along the left margin
- SA nodal branch - in ~40% of people, courses on the posterior atrial surface to supply the SA node
- Provides coronary blood flow to the LA
Coronary Dominance
Dominance is defined by which artery gives rise to the Posterior Descending Artery (PDA), which runs in the inferior interventricular groove:
| Dominance | PDA Origin | Prevalence |
|---|---|---|
| Right dominant | RCA | ~80% of patients |
| Left dominant | Circumflex (Cx) | ~15-20% |
| Co-dominant | Both RCA and Cx | Minority |
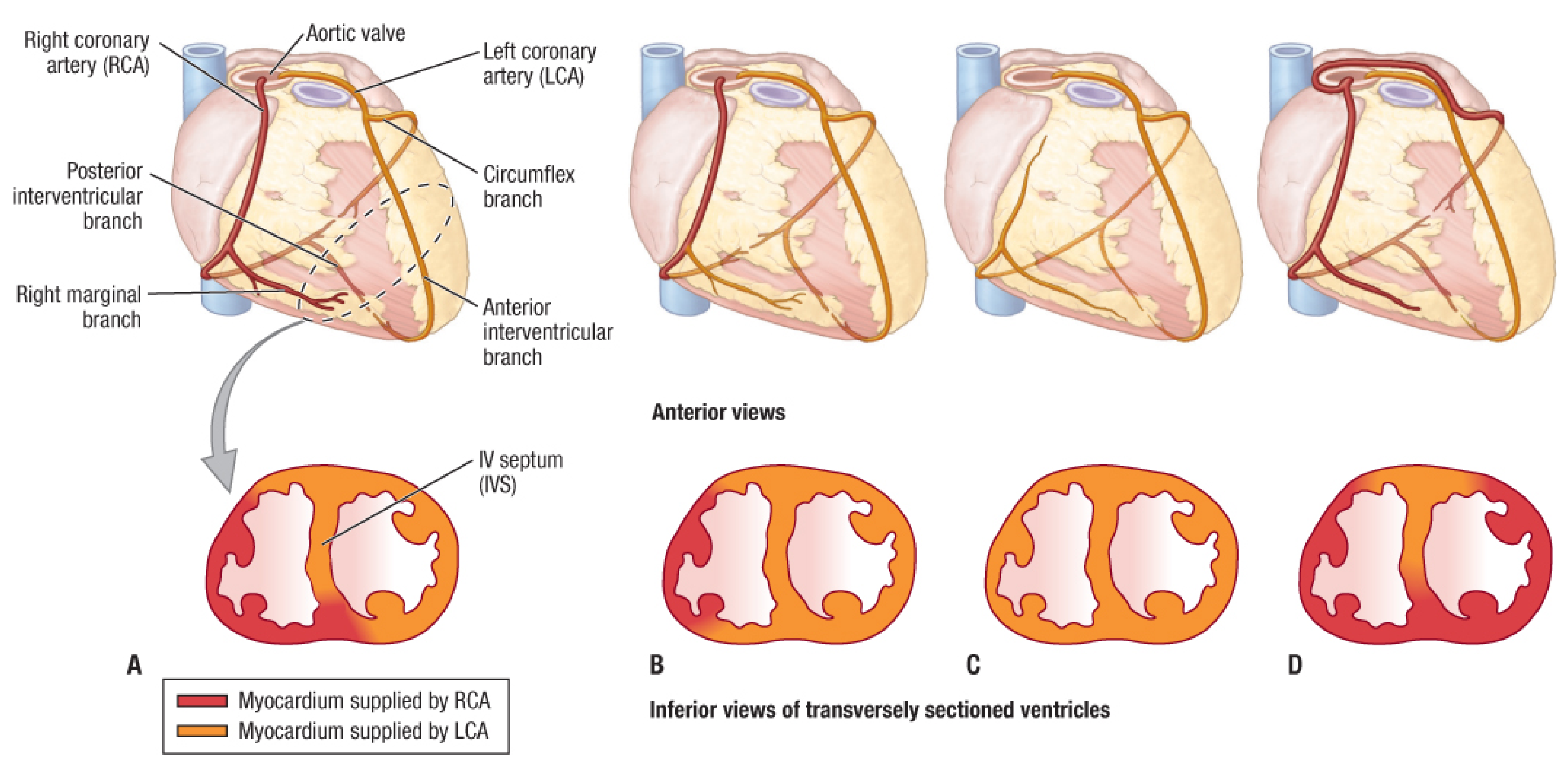
Territory of Supply (LV Wall Segments)
| Coronary Artery | Myocardial Territory |
|---|---|
| LAD | Anterior LV wall, anterior 2/3 of interventricular septum, LV apex |
| Circumflex (Cx) | Lateral LV wall (anterior and inferior aspects); LA |
| RCA | RV, medial inferior LV wall, posterior 1/3 of septum |
| PDA | Inferior aspect of ventricular septum, inferior free wall |
Papillary muscles:
- Posterior-medial papillary muscle: usually supplied by either RCA or Cx alone (ratio ~2:1), making it highly vulnerable to ischemia
- Anterior-lateral papillary muscle: dual supply from LAD and Cx, so ischemia here is unusual
Conduction system:
- SA node: RCA in 55-60%, Cx in 40-45% of patients
- AV node: RCA branches most commonly, or less commonly Cx
Microanatomy and Functional Compartments
The coronary vascular system has three functionally distinct compartments:
-
Large epicardial conduit arteries (0.5-5 mm diameter) - the RCA, LAD, Cx and their proximal branches. They act as low-resistance conduits; do NOT significantly resist blood flow unless atherosclerosis is present. They respond to flow-mediated vasodilation.
-
Prearterioles (100-500 μm diameter) - intermediate vessels that maintain pressure at the origin of arterioles during changes in perfusion pressure; regulated by a myogenic mechanism.
-
Intramural arterioles (<100 μm) - the major site of coronary vascular resistance; have significant vasodilator reserve and are highly sensitive to vasoactive metabolites produced by the myocardium in response to metabolic demand.
The capillary density in the myocardium is exceptionally high (3,000-4,000/mm²) with approximately a 1:1 ratio of capillaries to muscle fibers, reflecting the heart's high metabolic demands.
Venous Drainage
The heart is drained primarily by veins emptying into the coronary sinus, which runs in the posterior coronary sulcus and drains into the right atrium:
| Vein | Course |
|---|---|
| Great cardiac vein | Starts at apex, travels in anterior interventricular sulcus with the LAD, then turns posteriorly into the coronary sinus |
| Middle cardiac vein | Starts at apex, travels in the posterior interventricular sulcus with the PDA |
| Small cardiac vein | Accompanies the right marginal branch, then turns posteriorly to drain into the coronary sinus |
Small anterior cardiac veins also drain the RV directly into the right atrium.
Clinical Significance
- Atherosclerosis of the epicardial coronary arteries is the most common cause of myocardial ischemia. The proximal LAD (the "widow-maker") is the most clinically significant single vessel.
- Coronary artery spasm can cause vasospastic (Prinzmetal) angina independent of fixed stenosis.
- Collateral circulation may develop between branches of the same or different coronary arteries, providing alternative flow routes when a stenosis is present.
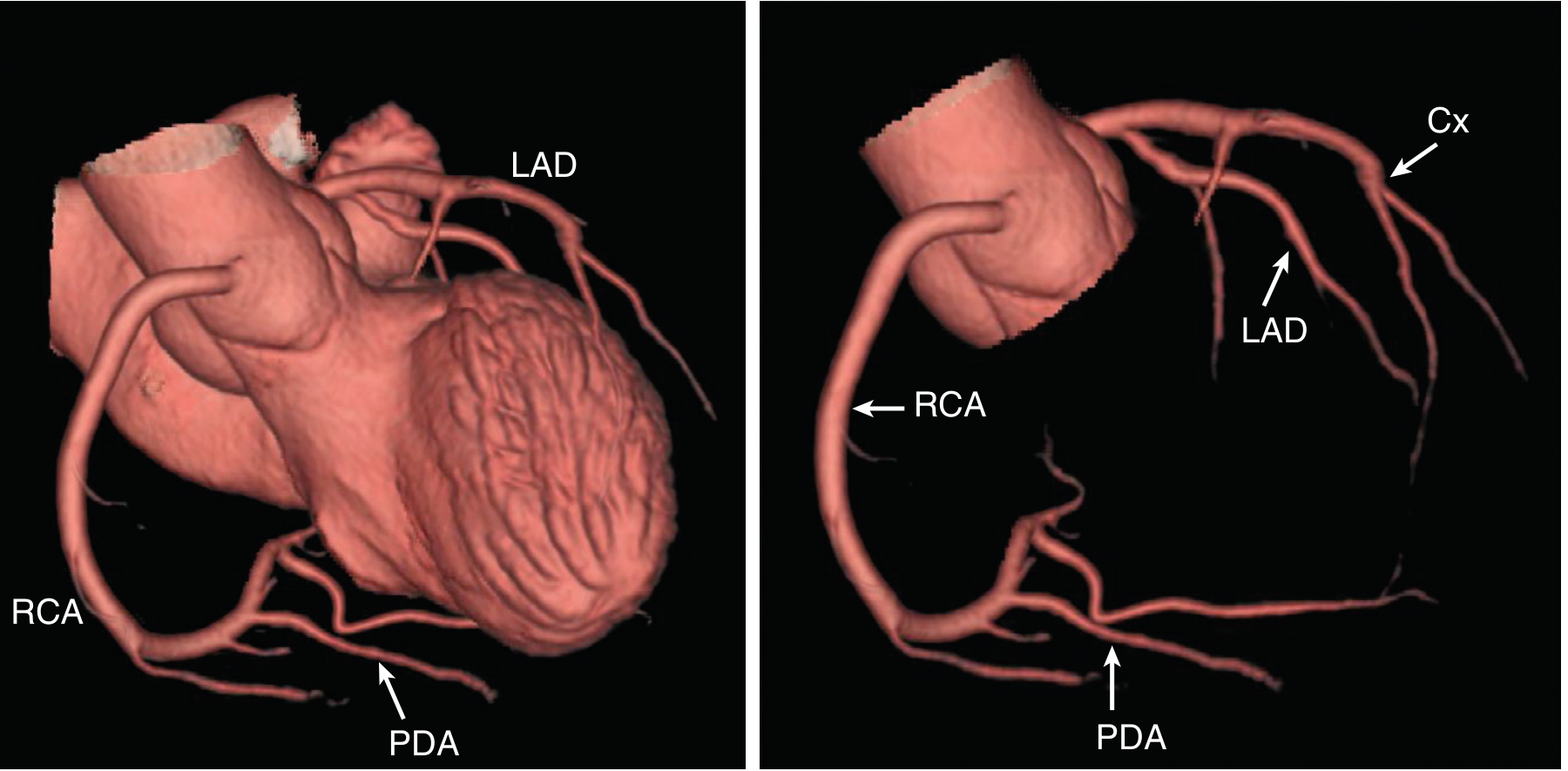
- Coronary CT angiography (CCTA) provides non-invasive assessment of coronary anatomy; invasive coronary angiography remains the gold standard, especially when combined with intervention (PCI).
- Regional wall motion abnormalities on echocardiography can localize the culprit coronary artery, as myocardial segments correspond closely to the coronary territory.
Sources: Fischer's Mastery of Surgery, 8th ed. | Barash's Clinical Anesthesia, 9th ed. | Textbook of Clinical Echocardiography | Braunwald's Heart Disease, 12th ed.
This is a shared conversation. Sign in to Orris to start your own chat.