Cushing syndrome
Reading File
Finding Sources
Searching PubMed
"Cushing syndrome"[MeSH Terms] AND diagnosis
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from multiple textbooks. Let me compile the full answer.
Cushing Syndrome
Definition and Epidemiology
Cushing syndrome is the clinical state resulting from chronic exposure to excess glucocorticoids, whether from endogenous overproduction or exogenous administration. It is rare, occurring in approximately 2-5 per million people per year. Peak age of onset is in the 20s and 30s, with women affected about four times more often than men in non-iatrogenic cases.
The term Cushing disease specifically refers to the subset caused by an ACTH-secreting pituitary adenoma, while Cushing syndrome is the broader umbrella term.
Causes and Classification
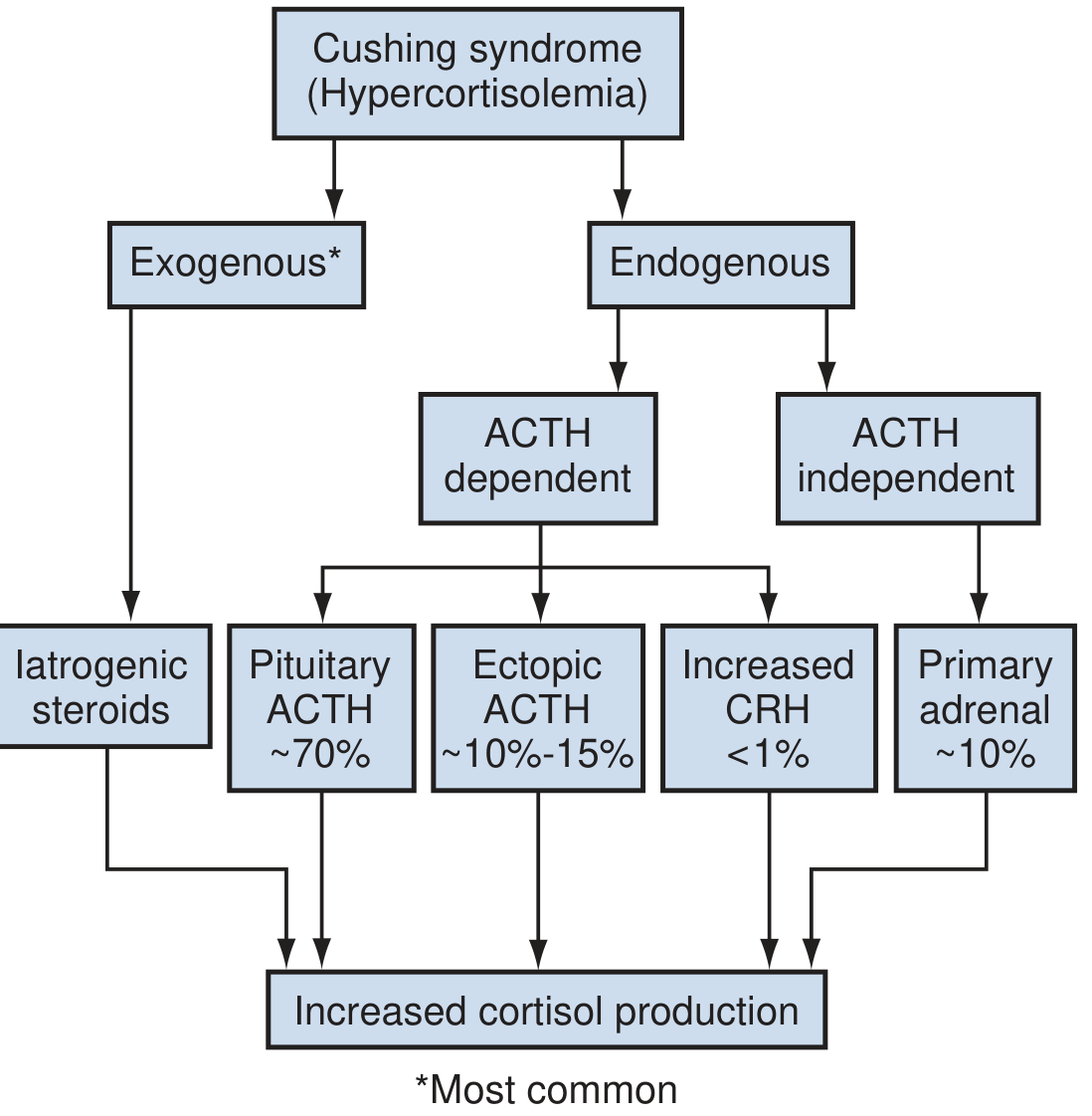
1. Exogenous (Iatrogenic) - Most Common Overall
The most common cause in the Western world. Results from therapeutic glucocorticoids given orally, topically, inhaled, or by injection. Patients may be unaware of steroid exposure (herbal remedies, nasal sprays) or may be surreptitiously self-administering them.
2. ACTH-Dependent (80-85% of endogenous cases)
| Cause | Proportion |
|---|---|
| Cushing disease (pituitary ACTH-secreting adenoma) | ~70% of endogenous |
| Ectopic ACTH syndrome (non-pituitary tumors) | ~10-15% |
| Ectopic CRH syndrome | <1% |
- Cushing disease: Described by Harvey Cushing in 1932. Usually a microadenoma (<1 cm); macroadenomas account for only ~5% of cases. Up to 2/3 of patients are female.
- Ectopic ACTH syndrome: ACTH-secreting tumors are nearly always malignant. Small cell lung cancer is the classic example, but carcinoids, medullary thyroid carcinoma, pheochromocytoma, and thymoma are also sources. Adrenal glands are bilaterally enlarged due to high ACTH drive.
3. ACTH-Independent (~10% of endogenous cases)
- Adrenal adenoma: Most common ACTH-independent cause; usually unilateral.
- Adrenal carcinoma: Accounts for ~8% of Cushing syndrome; independent predictor of poor prognosis. Cortisol production often accompanied by androgen excess.
- ACTH-independent macronodular adrenal hyperplasia (AIMAH): <1% of cases; bilateral, large nodules; each gland may weigh >60 g.
- Primary pigmented nodular adrenocortical disease (PPNAD): <1% of cases; adrenal glands remain normal size but contain black/brown cortical nodules; associated with Carney complex (autosomal dominant).
Pathophysiology
The zona fasciculata secretes up to 20 mg of cortisol daily under HPA axis regulation. CRH from the hypothalamic suprachiasmatic nucleus stimulates pituitary ACTH, which drives cortisol secretion. Cortisol feeds back to inhibit both CRH and ACTH. Cortisol secretion follows a circadian rhythm - highest in the morning, nadir at ~11 PM.
In Cushing syndrome, this feedback loop is disrupted:
- In ACTH-independent disease: autonomous adrenal cortisol production suppresses ACTH (ACTH is low)
- In Cushing disease: pituitary adenoma is relatively insensitive to glucocorticoid feedback (ACTH is elevated)
- In ectopic ACTH: tumor secretes ACTH independently, completely ignoring feedback (ACTH is markedly elevated)
Excess cortisol produces diverse systemic effects:
- Metabolic: hyperglycemia (gluconeogenesis), dyslipidemia, insulin resistance
- Protein catabolism: muscle wasting, thin extremities, poor wound healing, osteoporosis
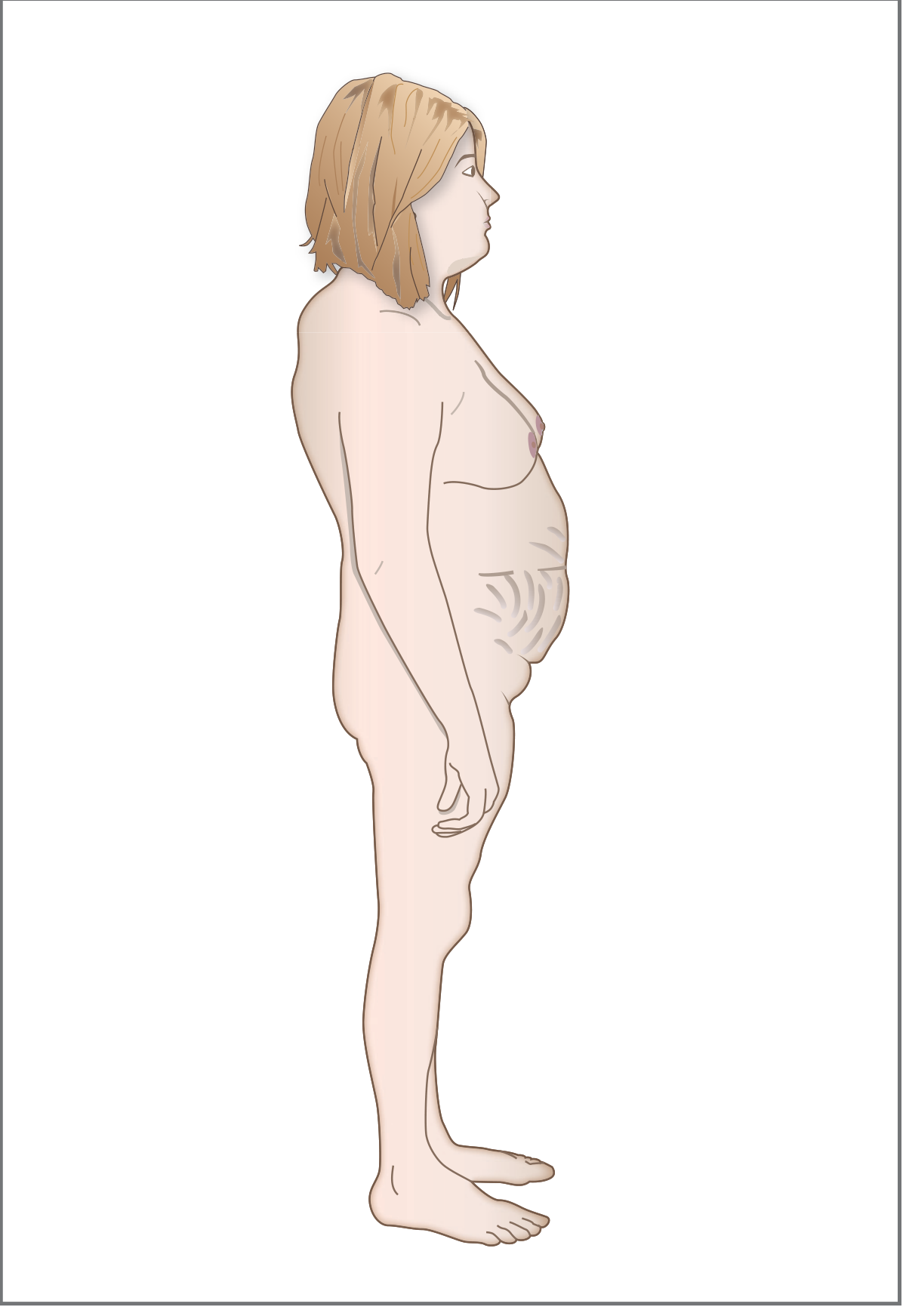
- Fat redistribution: central obesity, moon face, buffalo hump, supraclavicular fat pads
- Cardiovascular: hypertension (via weak mineralocorticoid activity + upregulation of vascular alpha-1 receptors)
- Immune suppression: susceptibility to infections
- Skin: atrophy, striae, easy bruising
- Psychiatric: depression, cognitive impairment, psychosis
Clinical Features
Classic Signs (combination raises suspicion)
| Feature | Description |
|---|---|
| Central obesity | Face, neck, trunk, abdomen spared by limbs |
| Moon facies | Wide, round face; plethora over cheeks, anterior neck, and chest V |
| Buffalo hump | Dorsocervical fat pad; accentuated by kyphosis |
| Supraclavicular fat pads | Characteristic |
| Purple striae | Wide (>1 cm), purplish, atrophic; abdomen, buttocks, thighs, breasts, upper arms |
| Skin thinning | "Cigarette paper" wrinkling; positive Liddle sign (skin tears off with adhesive tape removal) |
| Easy bruising | Ecchymoses with minimal trauma |
| Proximal muscle weakness | Difficulty rising from chair, climbing stairs |
| Hirsutism/virilization | From excess adrenal androgens (women) |
| Menstrual irregularities | Oligo- or amenorrhea |
| Hypertension | Present in majority |
| Osteoporosis/fractures | Kyphosis, vertebral fractures |
| Hyperglycemia/DM | ~20% develop overt diabetes |
| Mood disturbances | Depression, anxiety, cognitive difficulties |
Skin findings (from Andrews' Dermatology)
Hypertrichosis, dryness, acne, susceptibility to dermatophyte and Pityrosporum infections, livedo reticularis, poikiloderma-like changes, and opportunistic fungal infections. Women develop facial lanugo hypertrichosis with scalp hair thinning.
Pseudo-Cushing Syndrome
Alcohol abuse can clinically and biochemically mimic Cushing syndrome. Depression and obesity (metabolic syndrome) overlap significantly with Cushing features.
Diagnosis
Diagnosis is one of the most complex tasks in clinical endocrinology. It proceeds in two stages: (1) confirm hypercortisolism, then (2) determine the cause.
Step 1 - Confirming Hypercortisolism (Screening Tests)
At least two of the following should be abnormal before proceeding:
| Test | Principle | Normal Cutoff |
|---|---|---|
| 24-hour urinary free cortisol (UFC) | Integrates free bioavailable cortisol over 24 hours; independent of cortisol-binding globulin | >3x upper limit of normal is highly suggestive |
| Overnight low-dose DST (1 mg dexamethasone at 11 PM, cortisol at 8 AM) | Probes glucocorticoid negative feedback; dexamethasone not detected by cortisol assay | Cortisol <50 nmol/L (1.8 mcg/dL) essentially rules out Cushing |
| Late-night salivary cortisol | Exploits absent circadian nadir in Cushing syndrome | Elevated at 11 PM is abnormal |
Second-line tests: 2-day low-dose DST, midnight plasma cortisol.
Tests no longer recommended: random serum cortisol, plasma ACTH for screening, urinary 17-ketosteroids, insulin tolerance testing, loperamide testing.
Note: UFC lacks sufficient sensitivity for subclinical Cushing syndrome (e.g., in adrenal incidentaloma workup). The Endocrine Society recommends against it in that setting.
Step 2 - Determining the Cause (ACTH Level is Central)
| ACTH Level | Interpretation | Next Step |
|---|---|---|
| Low (<5 pg/mL) | ACTH-independent - adrenal origin | CT/MRI adrenals |
| Normal-high (>15-20 pg/mL) | ACTH-dependent | High-dose DST + MRI pituitary + CRH stimulation test |
| Very high (>100-200 pg/mL) | Suggests ectopic ACTH | Search for occult tumor (chest CT, octreotide scan) |
High-dose DST (8 mg dexamethasone):
- In Cushing disease: cortisol and ACTH are suppressed by high-dose but NOT by low-dose dexamethasone (pituitary adenoma retains some sensitivity)
- In ectopic ACTH and adrenal tumors: cortisol is NOT suppressed by either dose
Inferior petrosal sinus sampling (IPSS): Gold standard for differentiating pituitary from ectopic ACTH source when imaging is equivocal.
Treatment
Treatment is directed at the underlying cause:
Cushing Disease (Pituitary)
- First-line: Transsphenoidal surgical resection of pituitary adenoma (80% remission in microadenomas)
- If surgery fails: repeat surgery, stereotactic radiation (gamma knife), bilateral adrenalectomy
- Medical therapy (bridging or adjunct): ketoconazole, metyrapone, cabergoline, pasireotide
Adrenal Adenoma
- Unilateral laparoscopic adrenalectomy - treatment of choice; Cushingoid phenotype resolves in 7-9 months (may persist years in some patients)
- Post-operative adrenal insufficiency must be managed with glucocorticoid replacement (contralateral adrenal is suppressed)
Adrenal Carcinoma
- Surgical resection (open adrenalectomy preferred for large tumors)
- Mitotane (adrenolytic agent) for unresectable or metastatic disease
- Adjuvant mitotane post-operatively to reduce recurrence
Ectopic ACTH Syndrome
- Remove primary tumor if possible
- Bilateral adrenalectomy for refractory hypercortisolism when tumor is occult or unresectable
- Medical adrenal blockade: ketoconazole, metyrapone, etomidate (emergency), mifepristone
Exogenous/Iatrogenic
- Taper and minimize glucocorticoid dose
- Switch to alternate-day dosing where possible
Steroidogenesis Inhibitors (Medical Therapy Summary)
| Drug | Mechanism |
|---|---|
| Ketoconazole | Blocks adrenal steroid biosynthesis (multiple enzymes) |
| Metyrapone | Blocks 11β-hydroxylase (last step in cortisol synthesis) |
| Osilodrostat | 11β-hydroxylase inhibitor (newer, approved for Cushing disease) |
| Pasireotide | Somatostatin analog; reduces ACTH from pituitary |
| Mifepristone | Glucocorticoid receptor antagonist (does not lower cortisol levels) |
| Mitotane | Adrenolytic; also inhibits steroidogenesis |
Complications and Comorbidities
- Cardiovascular disease (leading cause of mortality)
- Thromboembolic events (DVT/PE - increased risk perioperatively)
- Diabetes mellitus and metabolic syndrome
- Osteoporotic fractures
- Immunosuppression and opportunistic infections
- Neuropsychiatric disorders (depression, cognitive decline)
- Adrenal insufficiency after treatment (requires replacement)
- Nelson syndrome (after bilateral adrenalectomy for Cushing disease - pituitary adenoma may enlarge dramatically due to lost cortisol feedback, with marked skin hyperpigmentation)
Special Notes
- Subclinical Cushing syndrome: Biochemical evidence of autonomous cortisol secretion without classic clinical features; increasingly recognized in adrenal incidentalomas. Recent meta-analyses (2024) confirm increased fracture risk and bone density loss even in this mild form.
- Carney complex: PPNAD + atrial myxoma + spotty skin pigmentation + Sertoli cell tumors (autosomal dominant, PRKAR1A mutation)
- McCune-Albright syndrome: Bilateral macronodular adrenal hyperplasia + polyostotic fibrous dysplasia + café-au-lait spots
- MEN type I: Rare association with Cushing syndrome via pituitary or adrenal adenomas
Sources: Campbell Walsh Wein Urology, pp. 3134-3138 | Costanzo Physiology 7e, p. 443 | Andrews' Diseases of the Skin, p. 578 | Fitzpatrick's Dermatology Vol. 1
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 38888685) highlights ongoing challenges in differentiating true Cushing syndrome from non-neoplastic hypercortisolism (pseudo-Cushing states). Another 2024 meta-analysis (PMID 38703381) confirms significantly elevated fracture risk even in mild autonomous cortisol secretion/subclinical hypercortisolism from adrenal adenomas.
This is a shared conversation. Sign in to Orris to start your own chat.