Ventricles of brain anatomy
Ventricles of the Brain - Anatomy
Overview Diagrams (Figure 5.11)
1. Lateral Ventricles (Formerly 1st and 2nd Ventricles)
| Part | Location |
|---|---|
| Frontal (anterior) horn | Extends anteriorly into the frontal lobe; begins anterior to the interventricular foramen of Monro |
| Body | Posterior to the foramen of Monro, within the frontal and parietal lobes |
| Atrium (trigone) | Junction where the occipital horn, temporal horn, and body converge |
| Occipital (posterior) horn | Extends posteriorly into the occipital lobe |
| Temporal (inferior) horn | Extends inferiorly and anteriorly into the temporal lobe |
- The caudate nucleus and thalamus bulge inward from the lateral walls
- The corpus callosum forms the roof
- The septum pellucidum is a thin membrane separating the two lateral ventricles in the midline
- The fornix dangles from the bottom of the septum pellucidum, paralleling the C-shaped curve
- The hippocampal formation lies on the floor and medial wall of the temporal horn
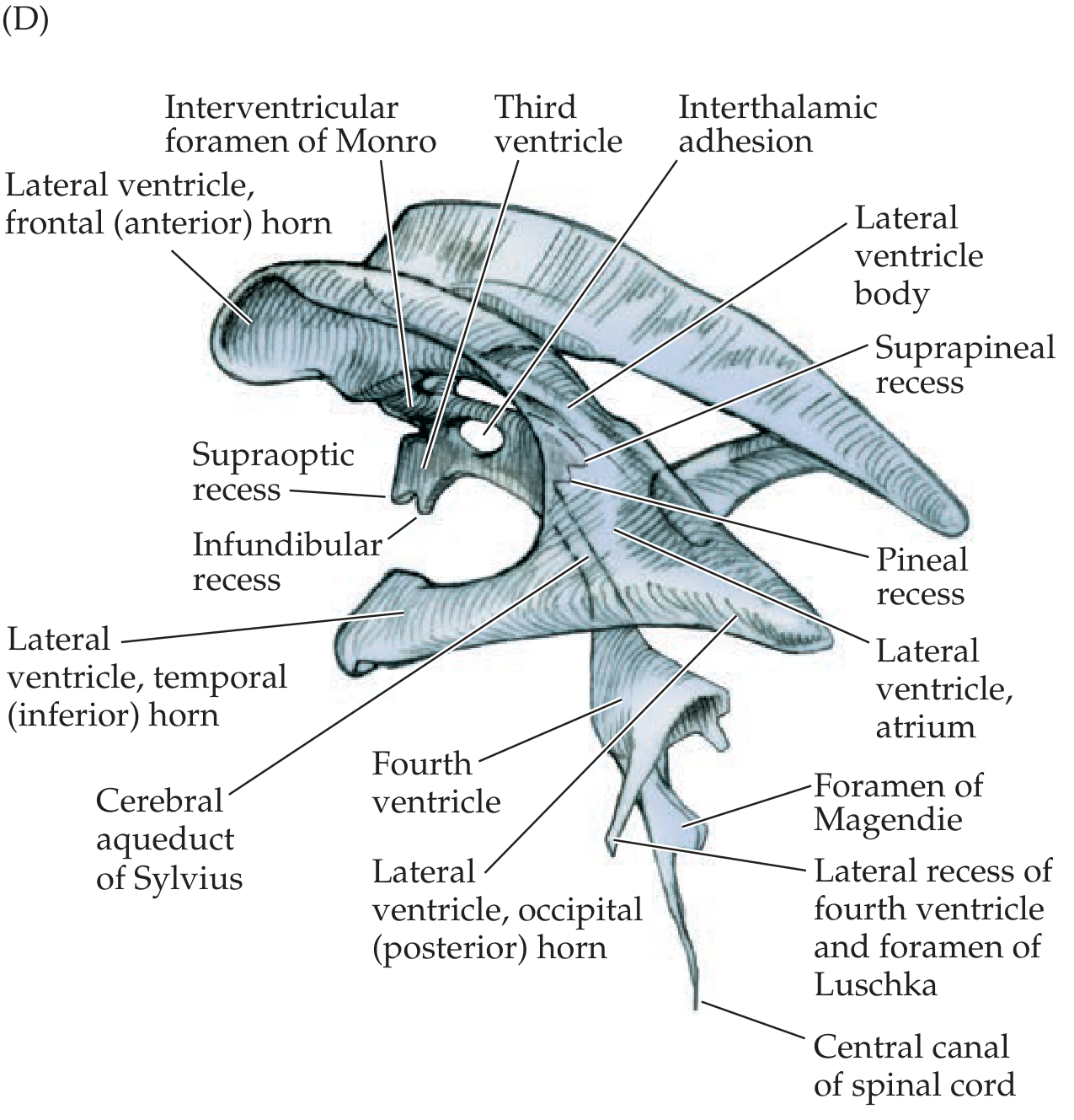
2. Third Ventricle
- Lateral walls: Thalami and hypothalamus
- Superior: Fornix
- Inferior: Hypothalamus
- Anterior: Anterior commissure, fornix, lamina terminalis, hypothalamus
- Posterior: Posterior commissure, pineal region, hypothalamus
- Supraoptic recess
- Infundibular recess
- Suprapineal recess
- Pineal recess
3. Fourth Ventricle
- Floor (rhomboid fossa): Formed by the dorsal surface of the pons (anteriorly) and medulla (posteriorly)
- Roof: Formed by the cerebellum
- Foramen of Magendie (median aperture) - single midline opening
- Foramina of Luschka (lateral apertures) - paired openings at the lateral recesses
Connecting Passages
| Structure | Connects |
|---|---|
| Interventricular foramina of Monro | Each lateral ventricle → Third ventricle |
| Cerebral aqueduct (of Sylvius) | Third ventricle → Fourth ventricle (passes entirely through midbrain gray matter) |
| Foramina of Magendie & Luschka | Fourth ventricle → Subarachnoid space |
| Central canal | Fourth ventricle → Spinal cord |
CSF Pathway Summary
Choroid plexus (mainly in lateral ventricles) → Lateral ventricles → Foramina of Monro → Third ventricle → Cerebral aqueduct → Fourth ventricle → Foramina of Magendie/Luschka → Subarachnoid space → Arachnoid granulations → Dural venous sinuses → Bloodstream
- Total volume in an adult: ~150 mL
- Rate of production: ~20 mL/hour (~500 mL/day)
- Produced primarily by the choroid plexus in all four ventricles
Lining
Create a detailed reference diagram comparing ventricles on different imaging planes (axial, coronal, sagittal)
Detailed medical reference diagram comparing brain ventricles on three imaging planes side by side: axial (transverse), coronal (frontal), and sagittal views. Each panel should be a clean anatomical illustration with labeled structures. AXIAL view (top-down cross-section): Show the lateral ventricles (frontal horns, body, occipital horns, temporal horns), third ventricle in midline, caudate nucleus bulging into lateral walls, septum pellucidum between the two lateral ventricles, corpus callosum roof. Label the atrium/trigone. CORONAL view (front-facing cross-section): Show both lateral ventricles side by side with the body and temporal horns, third ventricle in midline between thalami, fourth ventricle below, choroid plexus hanging in the ventricles, thalamus on lateral walls of third ventricle, fornix above third ventricle, corpus callosum arching over lateral ventricles. SAGITTAL view (side profile): Show the entire CSF pathway in sequence — lateral ventricle (frontal horn, body, atrium, occipital horn, temporal horn in C-shape), interventricular foramen of Monro, third ventricle with its recesses (supraoptic, infundibular, suprapineal, pineal), cerebral aqueduct of Sylvius through midbrain, fourth ventricle with its roof (cerebellum) and floor (pons/medulla), foramen of Magendie, central canal of spinal cord. Style: clean, clinical medical illustration on white background, blue-filled ventricles (light blue for fluid spaces), surrounding brain structures in grey/beige tones, black labels with leader lines, bold panel headers "AXIAL", "CORONAL", "SAGITTAL", professional textbook quality, no artistic flourishes
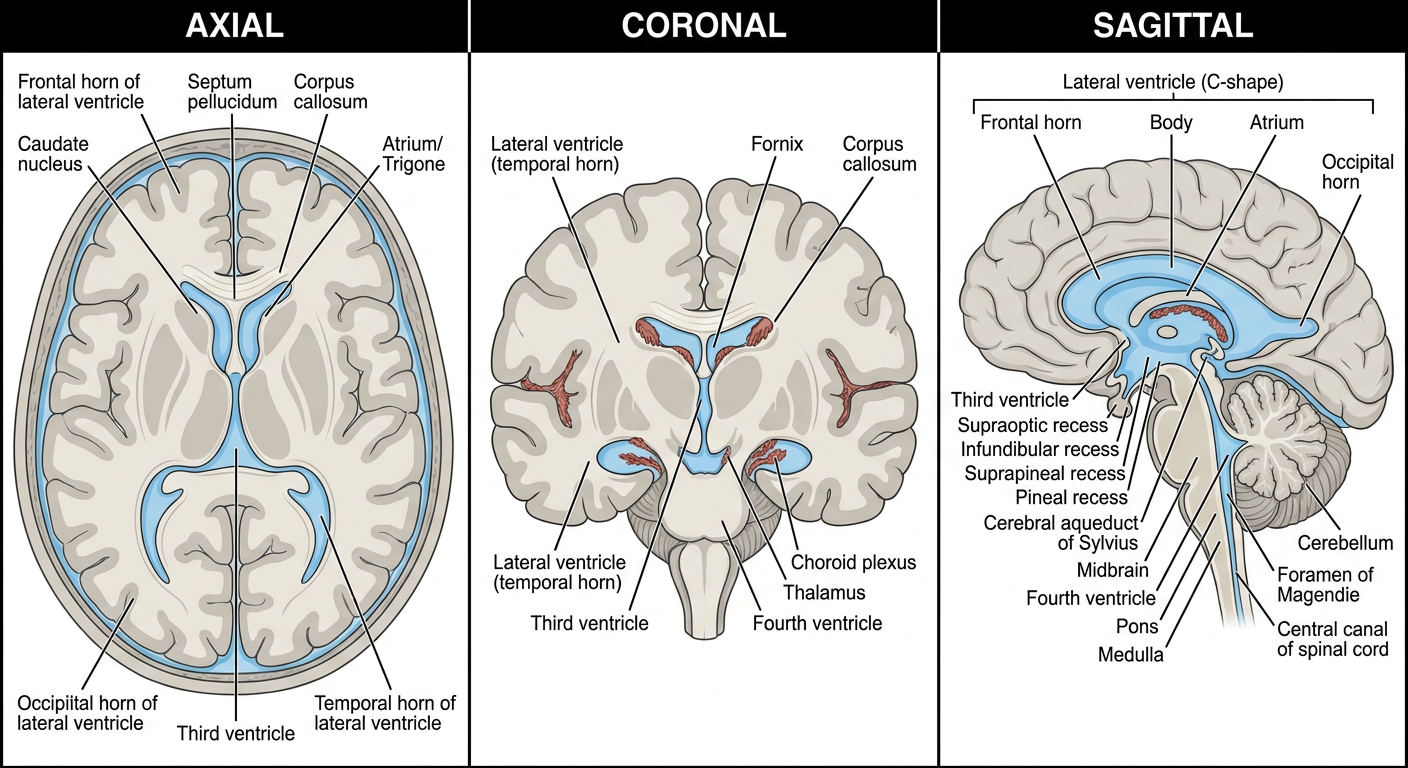
- Best for visualizing the frontal horns, body, and occipital horns of the lateral ventricles side by side
- Shows the septum pellucidum dividing the two lateral ventricles in the midline
- The third ventricle appears as a narrow midline slit between the thalami
- The caudate nucleus and thalamus are seen as impressions on the lateral walls
- Used in routine CT head scans to assess ventricular size and midline shift
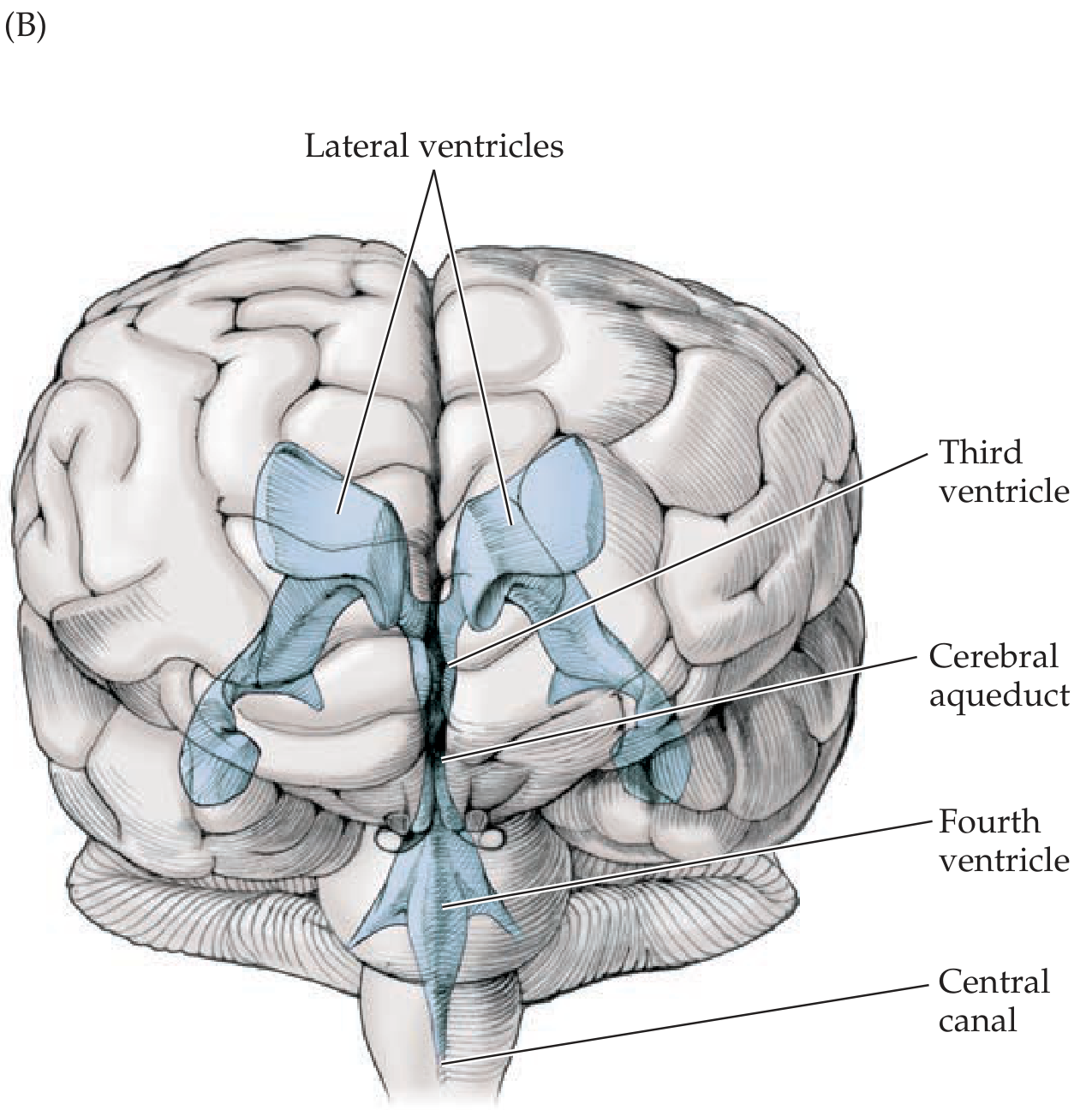
- Best for appreciating the vertical relationship of all four ventricles stacked together
- Lateral ventricles appear as bilateral paired cavities with the corpus callosum arching over them
- Third ventricle is seen sandwiched between the thalami
- Temporal horns are visible sweeping inferolaterally
- Choroid plexus is visible hanging into the body of the lateral ventricles
- Key plane for detecting transependymal edema in hydrocephalus
- Best for visualizing the complete CSF pathway as a continuous circuit
- The C-shape of the lateral ventricle is fully displayed
- All the recesses of the third ventricle (supraoptic, infundibular, suprapineal, pineal) are visible
- The cerebral aqueduct of Sylvius is seen as a thin channel through the midbrain
- The fourth ventricle and its exit via the foramen of Magendie are clearly shown
- Ideal for detecting aqueductal stenosis (a common cause of obstructive hydrocephalus)
Typhoid and medicine
"typhoid fever"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Typhoid Fever (Enteric Fever) - Complete Clinical Overview
Definition
Etiology and Pathogen
- Causative organism: Salmonella typhi (Gram-negative rod, Enterobacteriaceae)
- Antigens: O antigen (somatic), H antigen (flagellar), and Vi antigen (virulence capsular polysaccharide - important for immune evasion and used in vaccines)
- Reservoir: Humans only - cases and carriers (no animal reservoir)
- Survives intracellularly in mononuclear phagocytes; killed by drying, pasteurization, and common disinfectants
- Pathogenesis differs from NTS: S. Typhi does NOT effectively colonize the intestine but instead penetrates the gut mucosa and becomes a systemic pathogen. Mononuclear cell infiltration (not polymorphonuclear) into small bowel mucosa is characteristic
Epidemiology
- Global burden: 9.2-21 million typhoid cases + ~5 million paratyphoid cases annually; 110,000-280,000 deaths/year
- Most burden in South Asia (India, Pakistan, Bangladesh, Nepal) and parts of Africa - incidence exceeds 1,000/100,000 children in some urban areas
- Linked to fecal-oral transmission via contaminated water and food
- Risk factors: contaminated drinking water/ice, street food, raw vegetables grown in sewage-fertilized fields, lack of hand washing, prior H. pylori infection (gastric acidity reduction)
- Temporary carriers: convalescent (excrete for 6-8 weeks), incubatory
- Chronic carriers: defined as excretion >1 year after clinical illness; organisms persist in the gallbladder and biliary tract; develop in 2-5% of cases; may excrete for decades (the famous "Typhoid Mary" caused >1,300 cases in her lifetime)
- Fecal carriers >> urinary carriers; chronic urinary carriage often associated with urinary tract abnormalities
Pathogenesis
| Stage | Event |
|---|---|
| Ingestion | Contaminated food/water; infective dose ~10³-10⁹ organisms |
| Gut penetration | S. Typhi penetrates the epithelium via M cells and enterocytes in the terminal ileum |
| Lymphoid tissue | Colonizes Peyer's patches and mesenteric lymph nodes → mononuclear infiltration, enlargement |
| Primary bacteremia | Spreads to liver, spleen, bone marrow (intracellular survival in macrophages) |
| Secondary bacteremia | Bacteria re-enter blood from reticuloendothelial cells → sustained bacteremia |
| Intestinal re-seeding | Excreted into gut via bile → Peyer's patches ulcerate → risk of perforation/hemorrhage |
Clinical Course (Incubation: 5-21 days, mean 10-14 days)
- Stepladder rising fever (up to 38.8-40.5°C / 101.8-104.9°F)
- Headache, malaise, anorexia, dry cough, constipation (present in ~30% - not always diarrhea)
- Relative bradycardia (pulse-temperature dissociation) - classic sign
- Sustained high fever
- Rose spots - pale pink/red macular rash on the trunk (seen in ~20-30%, mainly fair-skinned patients)
- Splenomegaly and hepatomegaly develop
- Abdominal distention; diarrhea or constipation
- Leukopenia with relative lymphocytosis, elevated liver enzymes
- Possible defervescence spontaneously or complications
Key point: Fever is present at presentation in >75% of cases, but abdominal pain in only 30-40% - so a high index of suspicion is needed in febrile returning travelers.
Complications
| System | Complication |
|---|---|
| GI (most important) | Intestinal perforation (most serious), GI hemorrhage |
| Hematologic | Anemia, DIC |
| Neurologic | Meningitis, encephalopathy, psychosis, ataxia, seizures, deafness |
| Cardiovascular | Myocarditis, mycotic aneurysm |
| Respiratory | Pneumonia |
| Hepatobiliary | Cholecystitis (chronic carriers) |
| Renal | Renal failure |
| Other | Septic arthritis, relapse (10-15% of untreated cases) |
Diagnosis
| Method | Details |
|---|---|
| Blood culture (gold standard week 1-2) | 60-80% sensitivity; most useful in first week |
| Bone marrow culture | Most sensitive (~90%); positive even after antibiotic treatment |
| Stool culture (week 2 onwards) | Useful in second/third week |
| Urine culture | Less sensitive; useful in second week |
| Widal test | Rising agglutinin titers (O and H antigens); limited by low sensitivity/specificity; can be false-positive in endemic areas |
| Rapid antigen tests | Available; useful in field settings |
| CBC | Leukopenia common; thrombocytopenia, elevated LFTs |
Treatment
First-line antibiotics (uncomplicated typhoid)
| Drug | Dose/Route | Notes |
|---|---|---|
| Azithromycin | 500-1000 mg/day PO × 5-7 days | Drug of choice for uncomplicated typhoid, especially in areas with fluoroquinolone resistance; effective against XDR strains |
| Ceftriaxone | 2-3 g/day IV × 7-14 days | Preferred for severe/complicated typhoid; parenteral |
| Cefixime | 20 mg/kg/day PO × 7-14 days | Oral option for uncomplicated disease |
| Ciprofloxacin | 500 mg BD PO × 7-10 days | Now unreliable in South/Southeast Asia due to rising DSC and XDR strains; still used where susceptibility confirmed |
Drugs now generally unreliable (resistance)
- Chloramphenicol, Ampicillin, Trimethoprim-sulfamethoxazole - first-line drugs until MDR emergence; now unreliable globally
Severe typhoid / typhoid with meningitis or shock
- Ceftriaxone IV + Dexamethasone (0.3 mg/kg IV loading dose, then 0.1 mg/kg q6h × 8 doses) - shown to reduce mortality in severe disease with altered consciousness or shock
Supportive care
- IV fluids for rehydration
- Blood transfusion if significant GI hemorrhage
- Surgical consultation for intestinal perforation
Carrier treatment
- Ciprofloxacin 750 mg BD × 4 weeks for chronic carriers (combined with cholecystectomy if gallstones present)
Drug Resistance - Current Threat
| Resistance Type | Definition | Key Drugs Affected |
|---|---|---|
| MDR (multidrug-resistant) | Resistant to chloramphenicol + ampicillin + cotrimoxazole | All three first-line drugs |
| DSC (decreased susceptibility to ciprofloxacin) | MIC 0.125-0.5 µg/mL | Fluoroquinolones unreliable |
| XDR (extensively drug-resistant) | MDR + fluoroquinolone resistant + ESBL (cephalosporin resistant) | Emerged 2016, Sindh, Pakistan; azithromycin remains active |
XDR S. Typhi (H58 clone, Pakistan) is now spreading internationally via air travel. Azithromycin resistance is also emerging in some areas.
Vaccines
| Vaccine | Type | Route | Duration | Notes |
|---|---|---|---|---|
| Ty21a (Vivotif) | Live attenuated oral | PO, 3-4 doses | ~5 years | Avoid with antibiotics or immunosuppression |
| Vi polysaccharide (Typhim Vi) | Purified Vi antigen | IM, single dose | 2-3 years | Not for children <2 years |
| Typhoid Conjugate Vaccine (TCV) | Vi conjugated to tetanus toxoid | IM, single dose | Longer-lasting | WHO preferred for children; effective from 6 months; single dose |
- Protection is not complete - revaccination required and food/water precautions must be maintained
- Not effective against paratyphoid
- WHO recommends TCV for routine immunization programs in high-burden countries
Prevention and Control
- Safe water supply and sewage treatment (most impactful)
- Food hygiene and hand washing
- Identification and treatment of chronic carriers
- Vaccination for travelers and endemic populations
- Notification to public health authorities (typhoid is a notifiable disease)