Explain Cell injury-causes, mechanism & toxic injuries with special reference to Physical, Chemical, & ionizing radiation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed to compile a comprehensive, well-structured answer. Let me compose the full response.
Cell Injury: Causes, Mechanisms, and Toxic Injuries (Physical, Chemical & Ionizing Radiation)
Based on Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
1. Overview
Cell injury is the basis of all disease. Injurious stimuli damage cells through diverse biochemical mechanisms, but they all tend to induce a stereotypic sequence of morphologic and structural alterations. There is always a time lag between the stress and the morphologic changes - biochemical changes may appear in minutes to hours, while light microscopic changes may take hours to days.
The two fundamental outcomes of cell injury are:
- Reversible injury - the cell can recover if the noxious stimulus is removed
- Irreversible injury (cell death) - the cell passes the "point of no return" and dies by necrosis or apoptosis
2. Causes of Cell Injury
| Category | Examples |
|---|---|
| Hypoxia & Ischemia | Arterial blockage, cardiorespiratory failure, anemia, CO poisoning |
| Physical agents | Mechanical trauma, extremes of temperature, radiation, electric shock, pressure changes |
| Chemical agents & toxins | Glucose/salt in hypertonic concentrations, arsenic, cyanide, mercury, CCl4, alcohol, drugs, environmental pollutants |
| Infectious agents | Viruses, bacteria, fungi, parasites - through toxins & immune responses |
| Immunologic reactions | Autoimmune diseases, allergy, chronic immune responses to microbes |
| Genetic abnormalities | Chromosomal defects (Down syndrome), point mutations (sickle cell anemia), inborn errors of metabolism |
| Nutritional imbalances | Protein-calorie deficiency; vitamin deficiencies; obesity leading to type 2 DM and atherosclerosis |
Robbins & Kumar Basic Pathology, Chapter 1 - Causes of Cell Injury
3. Sequence of Events: Reversible vs. Irreversible Injury
Reversible Cell Injury
Defined as a derangement of function and morphology that cells can recover from. Two consistent features:
- Cell swelling (hydropic change) - results from influx of water due to failure of the ATP-dependent Na⁺/K⁺-ATPase pump. Sodium accumulates inside the cell, causing osmotically driven water entry → cell swelling and ER dilation.
- Fatty change - occurs in organs involved in lipid metabolism (especially liver). Toxic injury disrupts metabolic pathways → rapid accumulation of triglyceride-filled lipid vacuoles.
Irreversible Cell Injury
When the injurious stimulus is too severe or prolonged, cells pass the point of no return. Two critical events mark this transition:
- Inability to reverse mitochondrial dysfunction even after restoration of oxygen
- Profound disturbances in membrane function, including permeabilization of plasma and lysosomal membranes
Morphologic features of necrosis:
- Cytoplasmic changes: Increased eosinophilia (denatured proteins), glassy homogeneous appearance (glycogen loss), vacuolated "moth-eaten" cytoplasm, myelin figures
- Nuclear changes (3 patterns):
- Pyknosis - nuclear shrinkage with increased basophilia; DNA condenses into a dark shrunken mass
- Karyorrhexis - fragmentation of the pyknotic nucleus
- Karyolysis - fading of basophilia due to DNase digestion; complete dissolution in 1-2 days
4. Mechanisms of Cell Injury
The four principal sites of damage are illustrated below:
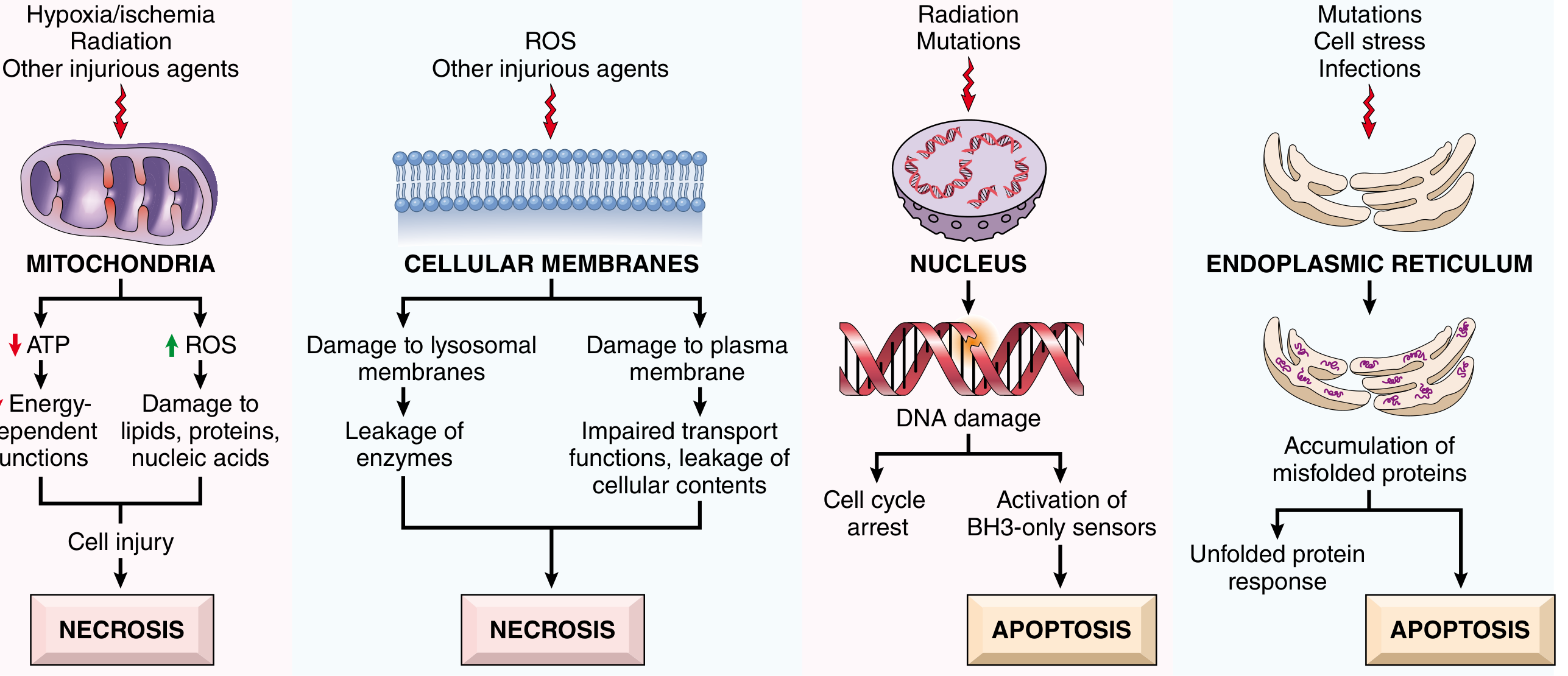
4a. Mitochondrial Damage - ATP Depletion
Mitochondria are the most sensitive targets in cell injury. Their damage produces:
ATP Depletion (to 5-10% of normal) causes widespread cellular effects:
- Failure of Na⁺/K⁺-ATPase → Na⁺ influx + K⁺ efflux → water accumulation → cell swelling
- Anaerobic glycolysis is activated → glycogen stores depleted → lactic acid accumulation → pH falls → chromatin clumping
- Ribosomal detachment from ER → reduced protein synthesis
- Protein misfolding (low pH, lack of energy for chaperones)
- Mitochondrial permeability transition pore (MPTP) opens → loss of membrane potential → failure of oxidative phosphorylation → necrosis
Increased ROS generation from damaged mitochondria damages lipids, proteins, and nucleic acids.
4b. Membrane Damage
Membranes are damaged by:
- Phospholipid loss - decreased synthesis due to ATP depletion or direct damage
- Lipid peroxidation by ROS - reactive oxygen species attack polyunsaturated fatty acids in membranes
- Cytoskeletal damage - Ca²⁺-activated proteases cleave cytoskeletal anchors, leading to membrane detachment and rupture
- Lysosomal membrane damage - releases lysosomal enzymes (DNases, RNases, proteases) into the cytoplasm → autodigestion of organelles
Plasma membrane damage: Impaired transport functions; leakage of cellular contents (LDH, transaminases, creatine kinase - useful as serum biomarkers of cell death).
4c. Oxidative Stress (Reactive Oxygen Species)
Key ROS in cell injury:
- Superoxide anion (O₂•⁻) - generated by reduction of O₂; converted by superoxide dismutase (SOD) to H₂O₂
- Hydrogen peroxide (H₂O₂) - converted to hydroxyl radical (OH•) by iron via Fenton reaction
- Hydroxyl radical (OH•) - most reactive and damaging ROS
Mechanisms of ROS damage:
- Lipid peroxidation of cell and organelle membranes (autocatalytic chain reaction)
- Oxidation of proteins - sulfhydryl cross-links, polypeptide fragmentation → enzyme inactivation
- DNA damage - single/double-strand breaks, base modifications → mutations
Cellular antioxidant defenses:
- Superoxide dismutase (converts O₂•⁻ → H₂O₂)
- Catalase (breaks down H₂O₂ → H₂O + O₂)
- Glutathione peroxidase (converts H₂O₂ and organic peroxides)
- Vitamins E, A, C; metal-binding proteins (transferrin, ceruloplasmin) - reduce free metal ion availability
4d. Intracellular Calcium Overload
- Normal cytoplasmic Ca²⁺ is very low (~0.1 μM); ischemia and toxins cause influx from extracellular space and release from ER/mitochondria
- Elevated Ca²⁺ activates:
- Phospholipases → membrane damage
- Proteases → cytoskeletal and membrane protein breakdown
- Endonucleases → DNA and chromatin fragmentation
- ATPases → ATP depletion
- Ca²⁺ overload also promotes MPTP opening → further ATP depletion and ROS generation
4e. DNA Damage and p53 Activation
- Damage to nuclear DNA (by radiation, ROS, chemotherapeutic drugs, or spontaneous deamination during aging) activates p53
- p53 arrests cells in G1 phase to allow DNA repair; if repair fails, p53 triggers apoptosis via the mitochondrial pathway
- Cells with TP53 mutations survive with abnormal genomes → malignant transformation
4f. Endoplasmic Reticulum (ER) Stress
- Accumulation of misfolded proteins in the ER activates the Unfolded Protein Response (UPR)
- If stress is not resolved, apoptosis is triggered via the mitochondrial (intrinsic) pathway
- Causes: ischemia, mutations, toxins, viral infections, aging
5. Toxic (Chemical) Injury - Special Reference
"Chemical injury remains a frequent problem in clinical medicine and is an important limitation to drug therapy. Because many drugs are metabolized in the liver, this organ is a major target of drug toxicity."
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Chemicals induce cell injury by two general mechanisms:
5a. Direct Toxicity
Some chemicals injure cells directly by combining with critical molecular components:
| Toxin | Mechanism | Target |
|---|---|---|
| Mercuric chloride (HgCl₂) | Binds sulfhydryl (-SH) groups of membrane proteins → increased permeability + inhibition of ion transport | GI tract, kidney |
| Cyanide | Poisons mitochondrial cytochrome oxidase → blocks oxidative phosphorylation | All cells, especially brain/heart |
| CO (carbon monoxide) | Binds hemoglobin with 200× affinity vs O₂ → functional anemia + direct cytochrome damage | Blood, all tissues |
| Antineoplastic drugs / antibiotics | Direct cytotoxic effects on cellular machinery | Rapidly dividing cells |
5b. Conversion to Toxic Metabolites (Indirect Toxicity)
Most toxic chemicals are biologically inactive in their native form. They are converted to reactive toxic metabolites by cytochrome P-450 mixed-function oxidases in the smooth ER of the liver (and other organs).
The toxic metabolites cause membrane damage mainly by:
- Free radical formation → lipid peroxidation
- Direct covalent binding to membrane proteins and lipids
Key examples:
Carbon tetrachloride (CCl₄):
- Previously used in dry cleaning industry
- Converted by cytochrome P-450 to the highly reactive free radical •CCl₃ (trichloromethyl radical)
- •CCl₃ + O₂ → •OOCCl₃ (trichloromethyl peroxy radical)
- Attacks polyunsaturated fatty acids → autocatalytic lipid peroxidation cascade
- Damages: ER membranes (fatty liver), mitochondria, plasma membranes
- Clinical: acute hepatic necrosis
Acetaminophen (Paracetamol):
- Converted in the liver by CYP2E1 to the highly reactive metabolite NAPQI (N-acetyl-p-benzoquinone imine)
- Normally detoxified by conjugation with glutathione
- Overdose depletes glutathione → NAPQI binds covalently to hepatocyte proteins → hepatocellular necrosis
- Clinical: acute liver failure (zone 3/centrilobular necrosis)
Alcohol (Ethanol):
- Converted by alcohol dehydrogenase and CYP2E1 → acetaldehyde + ROS
- Acetaldehyde forms adducts with proteins → cell injury
- CYP2E1 induction → increased ROS production → oxidative stress
- Clinical: fatty liver → alcoholic hepatitis → cirrhosis
6. Physical Injury - Special Reference
Physical agents capable of causing cell injury include:
6a. Mechanical Trauma
- Direct disruption of cell membranes and organelles
- Massive force → tearing of vessels, nerve injury, fractures
6b. Extremes of Temperature
Burns (heat injury):
- Mild heat (41-45°C): increased metabolic activity, reversible denaturation of proteins
- Severe heat (>50°C): Protein denaturation, coagulative necrosis, vascular damage
- Widespread burns cause systemic fluid loss, inflammatory cytokine release, risk of infection and sepsis
Cold (hypothermia):
- Indirect damage: Vasoconstriction → ischemia → hypoxic injury
- Direct damage: Ice crystal formation inside and outside cells → mechanical membrane disruption; concentration of electrolytes in unfrozen water → osmotic injury
- Frostbite: vascular damage + ice crystal formation → gangrene
6c. Sudden Changes in Atmospheric Pressure
- High pressure (dysbarism): Nitrogen dissolves in blood under high pressure; rapid decompression → nitrogen bubble formation in blood and tissues ("decompression sickness" / "the bends") → vascular occlusion, ischemia, joint pain, neurological deficits
- Low pressure (altitude): Reduced O₂ partial pressure → hypoxia
6d. Electric Shock
- Passage of electrical current through tissues generates heat (joule heating) → coagulative necrosis along the current path
- Can cause cardiac arrhythmias (ventricular fibrillation) by depolarizing myocardial cells
7. Ionizing Radiation - Special Reference
Types of Ionizing Radiation
| Type | Nature | Penetration | Damage per Unit |
|---|---|---|---|
| X-rays / Gamma rays | Electromagnetic waves (very high frequency) | Deep, long course | Less damage per unit tissue |
| Alpha particles | 2 protons + 2 neutrons | Restricted area | Heavy damage in restricted area |
| Beta particles | Electrons/positrons | Intermediate | Intermediate |
| High-energy neutrons | Neutral particles | Deep | Very high LET |
~50% of ionizing radiation received by the US population is human-made (mainly medical devices, CT scans, radioisotopes).
Radiation Units
| Unit | Definition |
|---|---|
| Curie (Ci) | Disintegrations per second of a radionuclide; 1 Ci = 3.7 × 10¹⁰ disintegrations/sec |
| Gray (Gy) | Energy absorbed per unit mass; 1 Gy = 10⁴ erg/g tissue; cGy = 100 Rad (R) |
| Sievert (Sv) | Equivalent dose accounting for biologic effects; Sv = Gy × relative biologic effectiveness |
Determinants of Biologic Effects
- Rate of delivery (dose rate): Fractionated doses allow repair between exposures - normal cells recover faster than tumor cells (exploited in cancer radiotherapy)
- Field size: Smaller fields are tolerated at higher doses; large field irradiation with smaller doses can be lethal
- Rate of cell division: Dividing cells are MORE vulnerable; nondividing cells (neurons, muscle) can survive DNA damage that would be lethal in dividing cells
- Oxygen levels: Hypoxic tissues (e.g., center of tumors) are LESS sensitive - oxygen enhances free radical production by radiolysis of water
Mechanisms of Cell Injury by Ionizing Radiation
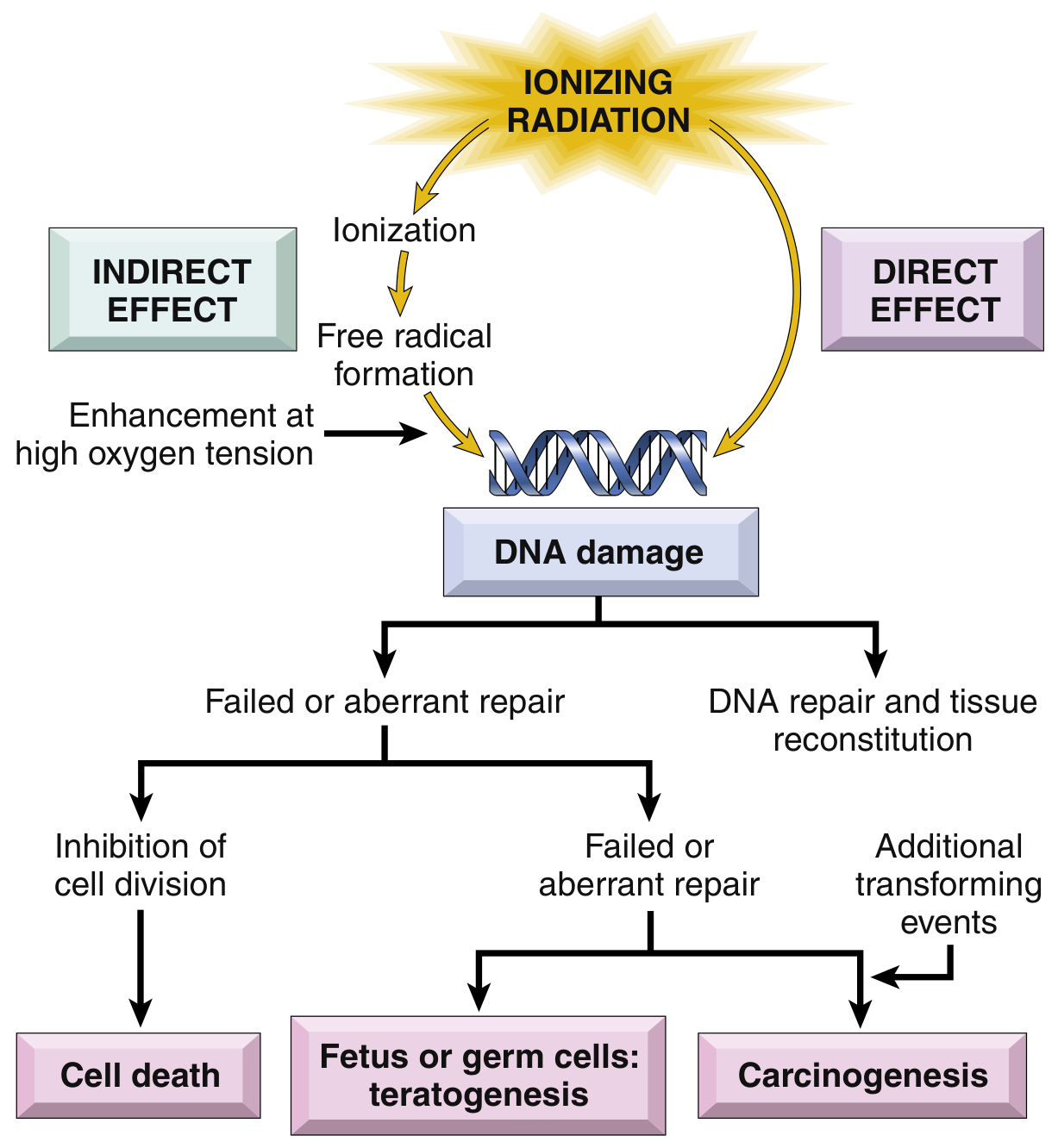
Two major mechanisms:
1. Indirect effect (predominant - ~70% of damage):
- Ionizing radiation causes radiolysis of water → free radicals (H•, OH•, O₂•⁻)
- OH• is the most damaging - attacks DNA bases, causes strand breaks, and DNA-protein crosslinks
- Enhanced at high oxygen tension (oxygen fixation hypothesis)
2. Direct effect:
- Radiation energy is directly absorbed by DNA or other macromolecules
- Causes base damage, single-strand breaks (SSBs), double-strand breaks (DSBs)
- DSBs are the most serious - repair is error-prone via non-homologous end joining
DNA Damage and Consequences:
- Simple defects may be corrected by enzyme repair systems
- ATM (ataxia-telangiectasia mutated) acts as the sensor for DNA damage
- p53 acts as the effector → cell cycle arrest → allows DNA repair
- If irreparable → p53 triggers apoptosis via the mitochondrial pathway
- If checkpoints are impaired (e.g., TP53 mutations) → cells with abnormal genomes survive → carcinogenesis
Consequences of Radiation Injury
Short-term effects:
- Cell death in rapidly dividing tissues: bone marrow, GI epithelium, gonads
- Hematopoietic and lymphoid systems: Most sensitive; radiation directly destroys lymphocytes in blood, lymph nodes, spleen, thymus; high doses → bone marrow aplasia → pancytopenia → hemorrhage + infection
- GI tract: Mucosal cell loss → ulceration, malabsorption, diarrhea, infection
- Gonads: Spermatogonia and oogonia are highly radiosensitive → sterility
Long-term effects:
- Fibrosis: Endothelial cell damage → vascular narrowing/occlusion → ischemia → parenchymal cell death replaced by connective tissue (weeks to months post-irradiation); inflammatory cytokines and chemokines activate fibroblasts
- Carcinogenesis: Mutations accumulate over years/decades → cancer (leukemia, thyroid cancer, solid tumors)
- Mutagenesis & Teratogenesis: Germ cell mutations; fetal exposure → teratogenic effects
Tissues ranked by radiosensitivity (most to least sensitive):
- Gonads
- Hematopoietic / lymphoid tissue
- GI tract epithelium
- Skin, oral/respiratory mucosa
- Kidney, liver, lung
- Bone, cartilage, nerve, muscle (least sensitive)
8. Summary: Comparison of Toxic Injury Types
| Feature | Chemical/Toxic | Physical | Ionizing Radiation |
|---|---|---|---|
| Primary target | Membranes, enzymes, DNA | Membranes, organelles, vasculature | DNA (primary), membranes |
| Key mechanism | Direct toxicity OR metabolic conversion → free radicals | Mechanical disruption, thermal denaturation, ice crystal formation | Radiolysis → free radicals; direct DNA strand breaks |
| Key mediator | Cytochrome P-450 metabolites, free radicals | Temperature, pressure, electrical current | OH• radical (indirect); direct ionization |
| Reversibility | Dose-dependent; low doses often reversible | Depends on extent; severe burns irreversible | Low dose: reversible; high dose → necrosis, apoptosis |
| Long-term risks | Organ-specific toxicity (liver, kidney) | Scarring, ischemic atrophy | Fibrosis, mutagenesis, carcinogenesis, teratogenesis |
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology), Chapter 1 - Cell Injury, Cell Death, and Adaptations; Chapter 7 - Environmental and Nutritional Diseases
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 2 - Cellular Responses to Stress and Toxic Insults; Chapter 9 - Environmental and Nutritional Diseases
This is a shared conversation. Sign in to Orris to start your own chat.