Ligament of shoulder joint
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full answer:
Ligaments of the Shoulder (Glenohumeral) Joint
The shoulder joint is a ball-and-socket joint with an inherently loose capsule that allows a wide range of motion. Stability depends on several ligaments, which are best divided into intrinsic capsular ligaments and extrinsic/accessory ligaments.
Anatomy Diagrams
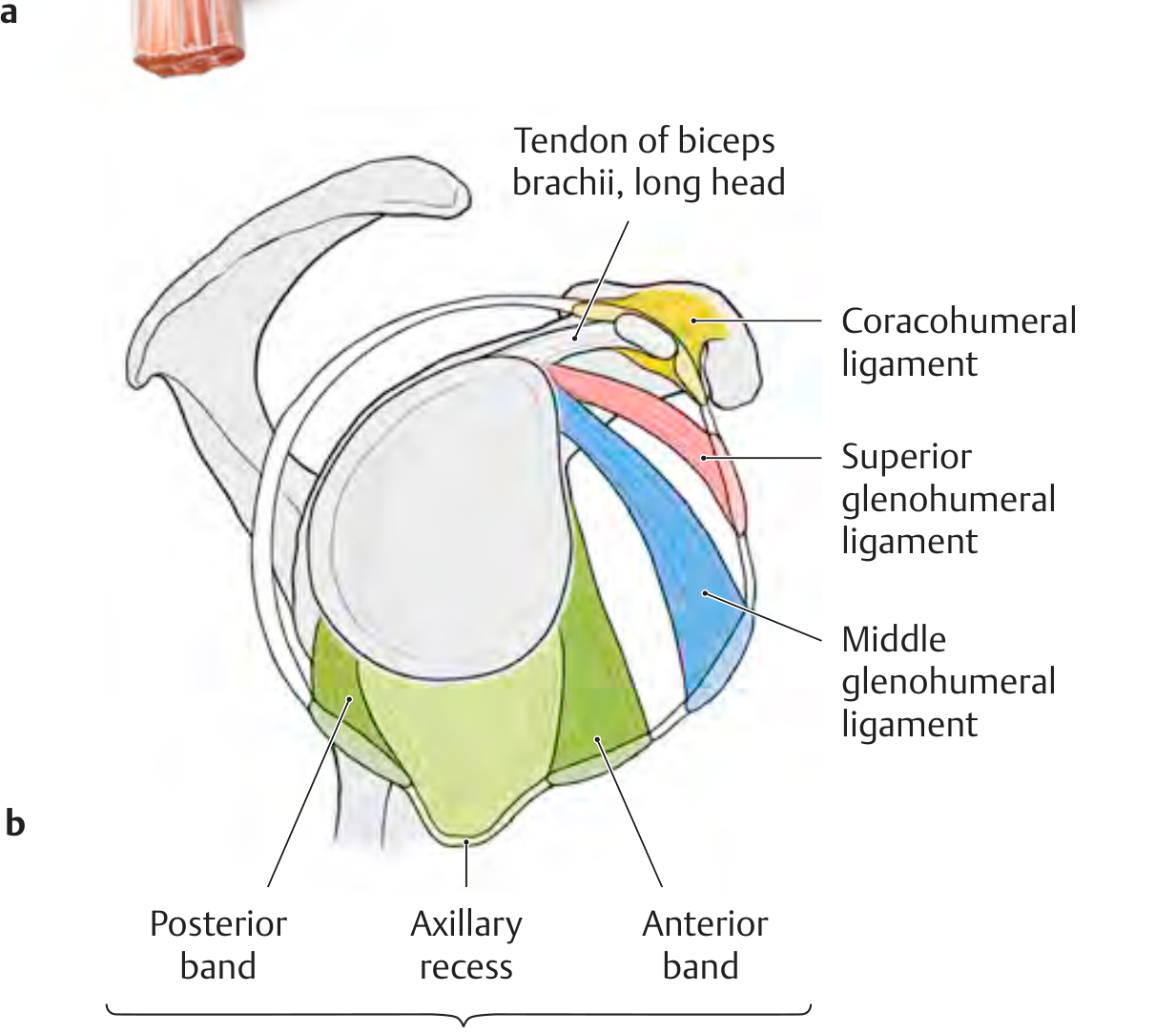
Fig. A - Anterior view of the shoulder joint capsule showing all four main ligaments and the three components of the inferior glenohumeral ligament (THIEME Atlas of Anatomy)
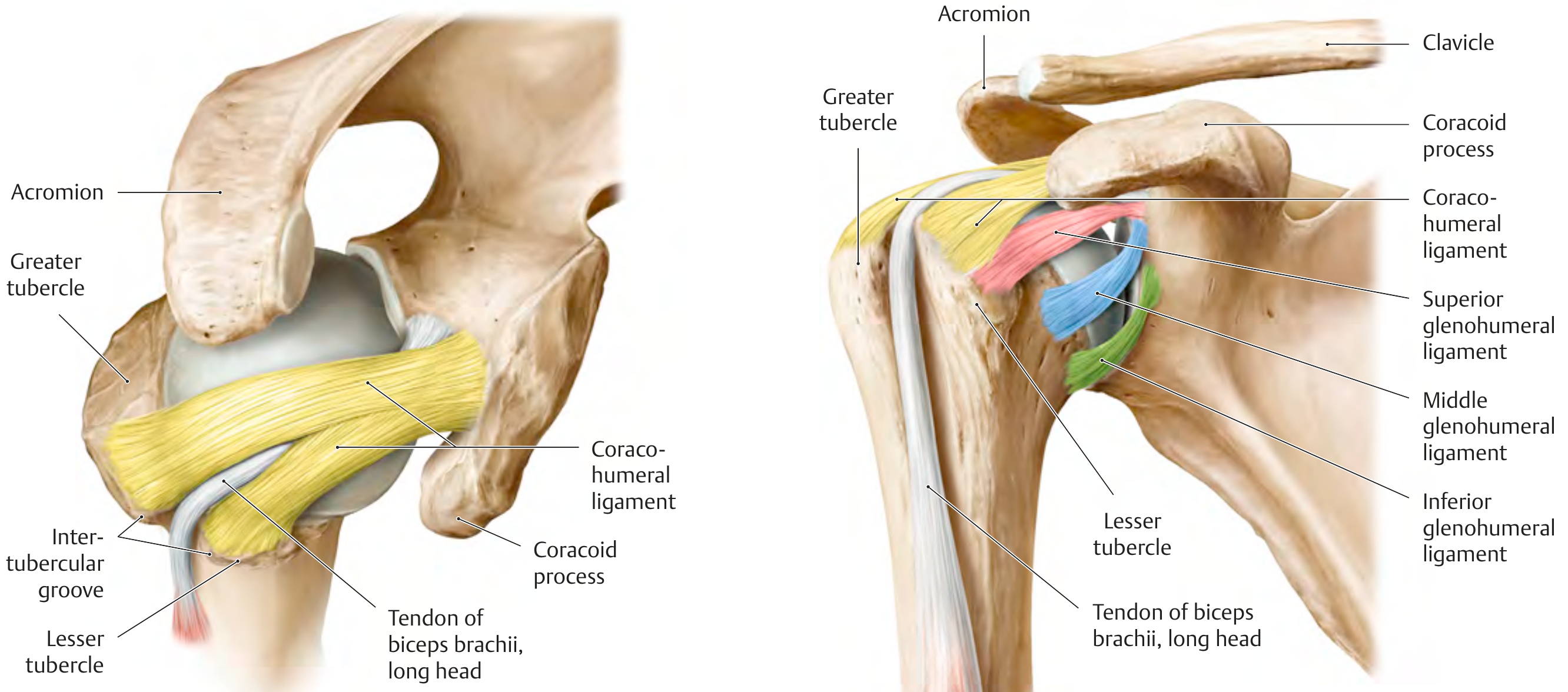
Fig. B - Left: coracohumeral ligament; Right: all three glenohumeral ligaments in relation to the glenoid and humeral head (THIEME Atlas of Anatomy)
1. Glenohumeral Ligaments (GHLs)
These are fibrous thickenings of the anterior joint capsule - three distinct bands visible on the inner surface of the capsule. They are the most important passive stabilizers of the shoulder, acting as restraints at the end range of motion.
A. Superior Glenohumeral Ligament (SGHL)
- Origin: Anterosuperior glenoid rim, conjoined with the biceps labral anchor
- Insertion: Proximal edge of the lesser tubercle / intertubercular groove
- Orientation: Runs nearly horizontal, parallel to the biceps tendon, almost perpendicular to the MGHL
- Function: Limits inferior translation and external rotation of the adducted shoulder (taut at 0° abduction); together with the coracohumeral ligament, it forms the biceps pulley in the rotator interval
- Note: Absent in 3-10% of healthy subjects
B. Middle Glenohumeral Ligament (MGHL)
- Origin: Upper margin of the glenoid cavity / glenoid neck
- Insertion: Anatomic neck of the humerus
- Orientation: Passes at almost a right angle to the subscapularis tendon insertion
- Function: Limits external rotation and anterior translation at 45-60° abduction
- Clinical note: Highly variable - the Buford complex involves a cord-like MGHL with congenital absence of the anterosuperior labrum (seen in ~1.5-2% of individuals)
C. Inferior Glenohumeral Ligament (IGHL)
- Origin: Inferior glenoid rim and labrum (anteromedial aspect)
- Insertion: Distal lesser tubercle and proximal humeral shaft
- Structure: Has three components - an anterior band (AB-IGHL), a posterior band (PB-IGHL), and an intervening axillary recess/pouch between the two bands
- Function: The primary restraint to anterior, posterior, and inferior translation with the arm in abduction (90°). Acts as a hammock during abduction; the anterior band is the most important restraint to anterior glenohumeral dislocations
- Clinical significance: The AB-IGHL is the most commonly injured ligament in anterior shoulder dislocations (Bankart lesion)
2. Coracohumeral Ligament (CHL)
- Origin: Base/lateral border of the coracoid process (broad, strong band)
- Insertion: Two slips go to the greater and lesser tubercles of the humerus (bridges the rotator interval)
- Function:
- Stabilizes the long head of the biceps tendon as it passes through the intertubercular groove (forms the roof of the biceps pulley with the SGHL)
- Together with the SGHL, limits inferior translation and external rotation of the adducted arm
- Reinforces the capsule superiorly
- Rotator interval: The CHL and SGHL together form the rotator interval - the capsular gap between the anterior edge of supraspinatus and the superior edge of subscapularis. Rotator interval closure reduces external rotation in adduction and posteroinferior translation.
3. Coracoacromial Ligament (CAL)
- Origin: Undersurface of the medial acromion
- Insertion: Superolateral border of the coracoid process
- Function: Acts as a tension band supporting the acromion and coracoid; forms the coracoacromial arch (along with acromion and coracoid process) which serves as a roof over the subacromial space. It limits upward displacement of the humeral head and transmits force from surrounding muscles.
- Clinical note: The CAL is not a true joint ligament but is functionally important; it is the primary structure involved in subacromial impingement. Its integrity becomes even more critical after acromioplasty.
4. Transverse Humeral Ligament
- Attachment: Bridges the greater and lesser tubercles of the humerus across the intertubercular (bicipital) groove
- Function: Acts as a retinaculum, holding the tendon of the long head of biceps brachii in the intertubercular groove, preventing it from subluxing medially
Summary Table
| Ligament | Origin | Insertion | Key Function |
|---|---|---|---|
| Superior GHL (SGHL) | Anterosuperior glenoid / labrum | Lesser tubercle | Limits inferior translation + ER at 0° abduction |
| Middle GHL (MGHL) | Upper glenoid / glenoid neck | Anatomic neck of humerus | Limits ER + anterior translation at 45-60° abduction |
| Inferior GHL (IGHL) - 3 parts | Inferior glenoid / labrum | Distal lesser tubercle / shaft | Primary restraint at 90° abduction; prevents anterior dislocation |
| Coracohumeral (CHL) | Coracoid process (base) | Greater + lesser tubercles | Stabilizes biceps pulley; limits ER + inferior translation in adduction |
| Coracoacromial (CAL) | Acromion undersurface | Coracoid process | Forms coracoacromial arch; limits upward humeral migration |
| Transverse humeral | Greater tubercle | Lesser tubercle | Retains long head of biceps in groove |
Functional Correlation: Position-Dependent Stability
The GHLs tighten at different positions of arm abduction:
- 0° (adduction): SGHL + CHL are taut
- 45-60° abduction: MGHL becomes taut
- 90° abduction: IGHL (especially anterior band) becomes the primary restraint
The posterior capsule is notably thin and not reinforced by ligaments, relying instead on the rotator cuff muscles for stability. The axillary recess (redundant fold of inferior capsule) provides a reserve capacity essential for full abduction. With prolonged immobility, this recess can become obliterated by adhesions, causing the characteristic stiffness of adhesive capsulitis (frozen shoulder).
Sources: THIEME Atlas of General Anatomy and Musculoskeletal System, p. 284-285; Imaging Anatomy Text and Atlas Vol. 3, p. 481-482; Rheumatology 2-Volume Set (Elsevier, 2022), p. 79
This is a shared conversation. Sign in to Orris to start your own chat.